Pain Assessment in ICU Settings
"pain assessment" AND "intensive care unit"
ICU pain assessment tools CPOT BPS PICS-ICU guidelines 2024 2025
https://www.guidelinecentral.com/guideline/25064
Pain Assessment in ICU Settings
Why Pain Assessment is Challenging in the ICU
- Intubated and unable to speak
- Sedated (deeply or lightly)
- Delirious - affecting their ability to perceive and report pain accurately
- Cognitively impaired from acute illness or pre-existing conditions
The Assessment Hierarchy (SCCM PADIS Guidelines)
- Patient self-report (gold standard when feasible)
- Behavioral observation (validated tools)
- Surrogate/family report - family members can identify pain behaviors based on prior knowledge of the patient
- Assume pain is present - especially after painful procedures or conditions, and trial an analgesic to see if suspected pain-related behaviors decrease
Self-Report Scales (Communicative Patients)
| Scale | How it Works | Use |
|---|---|---|
| Numeric Rating Scale (NRS) | Patient rates pain 0-10 verbally or in writing | Preferred by SCCM for patients who can self-report |
| Visual Analog Scale (VAS) | Patient marks a 100mm line from "no pain" to "worst pain" | Requires adequate motor function |
| Wong-Baker FACES | Patient points to a face matching their pain | Useful when language barriers exist |
Behavioral Pain Assessment Tools (Non-Communicative Patients)
1. Critical-Care Pain Observation Tool (CPOT)
| Clinical Indicator | Descriptor | Score |
|---|---|---|
| Facial expression | Relaxed | 0 |
| Tense (frowning, brow lowering) | 1 | |
| Grimacing (eyelids tightly closed) | 2 | |
| Body movements | Absent / normal position | 0 |
| Protective (rubbing, seeking attention) | 1 | |
| Restless/agitated (pulling tubes, striking staff) | 2 | |
| Muscle tension | Relaxed, no resistance to passive movement | 0 |
| Tense/rigid, resists passive movement | 1 | |
| Very tense/rigid, strong resistance | 2 | |
| Ventilator compliance (intubated) | Tolerating ventilator, no alarms | 0 |
| Coughing but tolerating | 1 | |
| Fighting ventilator, frequent alarms | 2 | |
| Vocalization (non-intubated) | Normal talking or silent | 0 |
| Sighing, moaning | 1 | |
| Crying out, sobbing | 2 |
2. Behavioral Pain Scale (BPS)
| Item | Description | Score |
|---|---|---|
| Facial expression | Relaxed | 1 |
| Partially tightened (brow lowering) | 2 | |
| Fully tightened (eyelid closing) | 3 | |
| Grimacing | 4 | |
| Upper limb movements | No movement | 1 |
| Partially bent | 2 | |
| Fully bent with finger flexion | 3 | |
| Permanently retracted | 4 | |
| Ventilator compliance | Tolerating movement | 1 |
| Coughing but tolerating most of the time | 2 | |
| Fighting ventilator | 3 | |
| Unable to control ventilation | 4 |
3. Behavioral Pain Assessment Tool (BPAT)
Comparison of BPS vs. CPOT
| Feature | CPOT | BPS |
|---|---|---|
| Score range | 0-8 | 3-12 |
| Domains | 4 (including muscle tension) | 3 |
| Includes muscle tension | Yes | No |
| Validated in delirium | Yes | No |
| Works in non-intubated | Yes (vocalization item) | Limited (max score drops) |
| Sensitivity | ~76.5% | ~62.7% |
| Preference in most studies | Slightly higher | Equally recommended (SCCM) |
Physiologic Measures
Integration with the ABCDEF Bundle
- A - Assess, prevent, and manage pain
- B - Both spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT)
- C - Choice of analgesia and sedation
- D - Daily delirium monitoring (CAM-ICU, ICDSC)
- E - Early exercise and mobility
- F - Family engagement
Special Populations
- Neonates/Pediatrics: Separate validated scales exist - NIPS (Neonatal Infant Pain Scale), FLACC (Faces, Legs, Activity, Cry, Consolability). The CPOT has been adapted for pediatric ICU use.
- Patients with cognitive impairment/dementia: Behavioral tools remain preferred; pain behaviors may differ and require individualized baseline assessment.
- Palliative/end-of-life ICU patients: Pain is frequently undertreated - the landmark SUPPORT trial found ~50% of dying patients had moderate-to-severe pain. Opioid titration remains the standard; adequately dosed opioids do not hasten death when used appropriately.
Key Clinical Takeaways
- Self-report is always first choice - never skip asking a patient who might be able to communicate.
- Do not use vital signs alone - they are unreliable pain proxies.
- Use CPOT or BPS for non-communicative patients - both are SCCM-endorsed.
- CPOT is preferred when the patient has delirium or when flexibility across intubated/non-intubated states is needed.
- Assess frequently and document - routine assessment improves analgesic use, reduces mechanical ventilation time, and shortens ICU stays.
- Treat pain before adding sedatives - analgesia-first approach reduces sedative burden and delirium risk.
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set - Chapter 151 (Prendergast, Girard, Brummel)
- Miller's Anesthesia, 10e - Chapter on Pain in the ICU
- Current Surgical Therapy, 14e - ABCDEF Bundle
- 2025 SCCM PADIS Focused Update (Lewis, Balas, Stollings et al., Crit Care Med 2025)
- Frontiers in Pain Research 2024 - CPOT narrative review
Emotional circuit in comatise patient
"emotional processing" AND "coma" AND "limbic"
emotional circuits limbic system comatose patients brain activity amygdala fMRI neuroscience
"disorders of consciousness" AND "emotional" AND "amygdala"
PMID: 18789930
"disorders of consciousness" AND "emotional stimuli" AND brain
PMID: 39892079
"disorders of consciousness" AND "EEG" AND "pain" OR "nociception"
Emotional Circuits in the Comatose Patient
1. Understanding Coma: What is Disrupted First
The Ascending Reticular Activating System (ARAS)
- Alertness - brainstem/diencephalic arousal circuits
- Attention - frontoparietal networks
- Awareness - subjective, unified experience integrating sensory, motor, emotional, and mnemonic information
| ARAS Component | Transmitter | Projections |
|---|---|---|
| Pontomesencephalic reticular formation | Glutamate, acetylcholine | Thalamus, hypothalamus, basal forebrain → cortex |
| Locus coeruleus (rostral pons) | Norepinephrine | Cortex, limbic structures |
| Raphe nuclei (midbrain) | Serotonin | Amygdala, septal nuclei, limbic lobe |
| Ventral tegmental area | Dopamine | Medial forebrain bundle, nigrostriatal pathway |
| Posterior hypothalamus | Histamine, orexin | Cortex and subcortical targets |
| Intralaminar/medial thalamic nuclei | Glutamate | Cerebral cortex |
2. The Emotional Circuit: Anatomy and Connections
The Papez Circuit (Core Emotional Loop)
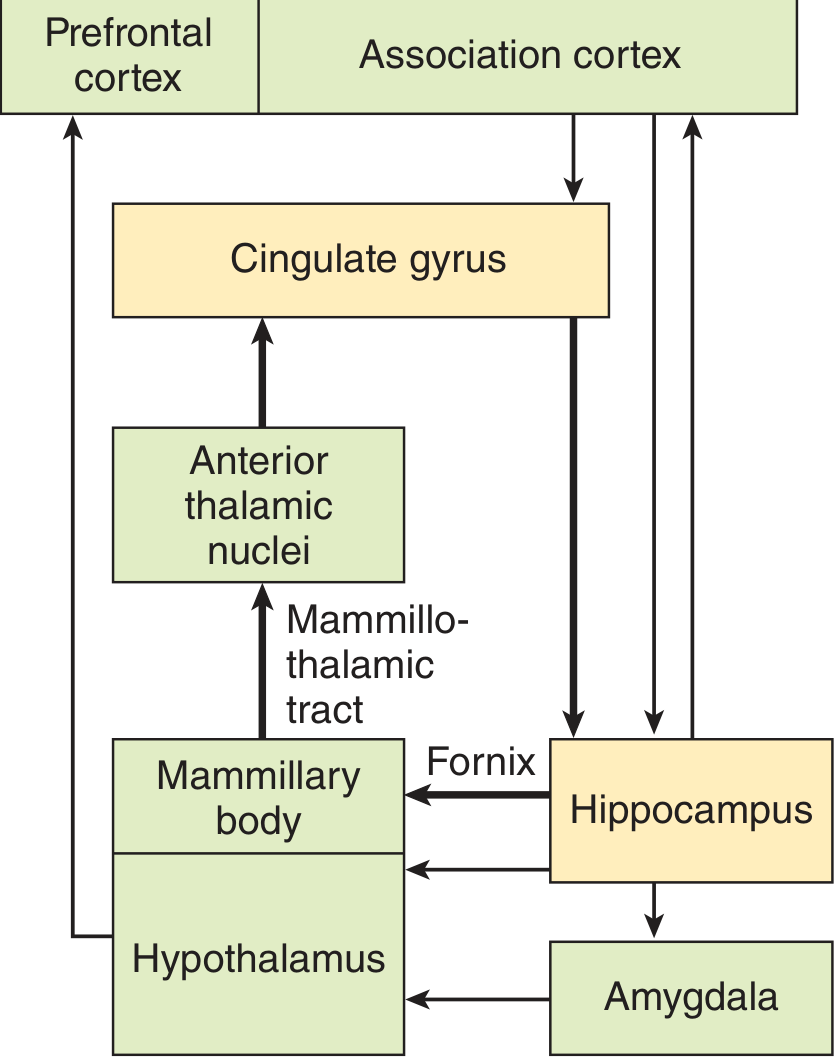
Key Limbic Structures and Their Emotional Roles
- The most critical structure for emotional salience detection - especially fear, threat, and social/emotional significance
- Three nuclear groups:
- Basolateral complex - functions like multimodal cortex; receives direct inputs from temporal, insular, and prefrontal cortices; bidirectionally connected to mediodorsal thalamus
- Centromedial group (extended amygdala) - connects to brainstem viscerosensory/visceromotor regions and lateral hypothalamus; governs autonomic/somatic emotional output
- Medial subdivision - connects to medial/endocrine hypothalamus
- The amygdala can receive emotional stimuli via a fast "low road" (direct thalamo-amygdala pathway - bypassing cortex) and a slower "high road" (cortical processing)
- Subgenual anterior cingulate (area 25): connected to amygdala, hypothalamus, hippocampus; overactive in depression
- Stimulation produces autonomic effects (HR increase, BP rise, pupil dilation, piloerection) - the visceral correlates of emotion
- Bilateral cingulectomy causes overall diminution of emotional reactions
- Critical for encoding and contextualizing emotional memories
- Funnels processed cortical information to and from entorhinal cortex
- Integrates autonomic, endocrine, and somatic outputs of emotion
- Contains fight-or-flight circuitry; stimulation produces "sham rage" (as shown by Bard's 1928 cat experiments)
- Connects to brainstem visceral nuclei and pituitary gland
- Septohippocampal pathway: anxiety regulation
- Reciprocally connects hippocampus, amygdala, hypothalamus, and brainstem
- Top-down modulation and regulation of emotional responses
- Receives direct projections from basolateral amygdala
Key Neurotransmitters of the Emotional Circuit
| Transmitter | Source | Target |
|---|---|---|
| Norepinephrine | Locus coeruleus, medullary nuclei | Hypothalamus (highest concentration), medial limbic structures |
| Serotonin | Midbrain raphe (reticular formation) | Amygdala, septal nuclei, lateral limbic lobe |
| Dopamine | Ventral tegmental area | Medial forebrain bundle, nigrostriatal pathway |
| Acetylcholine | Nucleus basalis (basal forebrain) | Cortex (arousal); amygdala outflow influences cortical arousal |
3. What Happens to Emotional Circuits in Coma
Structural Preservation vs. Functional Disruption
- Whether arousal inputs (from ARAS) still reach them
- Whether the cortex can integrate and consciously experience the output
- Whether subcortical processing continues without awareness
The "Fast" Subcortical Emotional Pathway
- Emotionally salient stimuli (threat, pain, familiar voices) can reach the amygdala even when cortical processing is compromised
- The amygdala can trigger autonomic responses (tachycardia, hypertension, stress hormone release) without conscious awareness
- Grimacing to painful stimuli in comatose patients
- Tachycardia/hypertension during procedures (suggestive of subcortical nociceptive-emotional processing)
- Spontaneous facial expressions in vegetative states
fMRI Evidence: Residual Emotional Processing in Coma
- fMRI showed robust cortical responses to visual, auditory, and tactile stimulation
- Speech stimuli activated Broca's and Wernicke's areas
- Familiar voices and direct addressing produced significantly stronger amygdala activation than unfamiliar voices and neutral phrases
- This demonstrates that emotional significance (familiarity) modulates amygdala activity even in behaviorally unresponsive comatose patients
EEG Evidence: The P300 and Emotional Stimuli
- Presence of a P300 to the patient's own name is associated with good prognosis for recovering to wakefulness in post-anoxic coma
- However, prognostic performance is insufficient alone - some patients without P300 still recover
- Stimuli with emotional valence (familiar voice, "smiling" vs. "rough" voice quality) recruit additional brain networks beyond auditory and attentional ones, potentially improving prognostic value
- This highlights that emotional familiarity - processed in part via limbic networks - adds information beyond pure auditory processing
4. Clinical Implications
Pain and Emotional Distress in the Comatose Patient
- Comatose patients may have subcortical pain processing without behavioral reporting
- This is why analgesic treatment is ethically and clinically important even in deeply comatose or vegetative patients
- Behavioral signs (grimacing, autonomic changes) reflect subcortical emotional-nociceptive circuit activity, not necessarily conscious suffering - but they cannot rule it out either
Emotional Stimuli as Diagnostic and Prognostic Tools
| Technique | What It Detects | Clinical Use |
|---|---|---|
| EEG / P300 (own-name) | Auditory-emotional processing in temporal/frontal cortex | Prognosis in post-anoxic coma |
| fMRI (familiar voice) | Amygdala activation to emotional salience | Residual consciousness assessment |
| Task-based fMRI (Rindex) | Spatial overlap of neural activation across tasks | Predicts arousal recovery (2025 JCN data) |
| Behavioral observation | Autonomic/facial responses to emotional stimuli | Bedside clinical assessment |
Vegetative State vs. Minimally Conscious State
- Vegetative state (unresponsive wakefulness syndrome): ARAS partially intact (eyes open, sleep-wake cycles present), but no behavioral evidence of awareness. Subcortical emotional circuits may still function.
- Minimally conscious state: Some cortical processing preserved; emotional stimuli may trigger purposeful or semi-purposeful behavioral responses.
- The distinction matters clinically: minimally conscious patients show more robust emotional circuit activity on fMRI/EEG, and their responses to familiar vs. unfamiliar emotional stimuli are more consistent.
Family/Caregiver Role
- Family presence and speaking to comatose patients has a neurobiological rationale - it activates emotional circuits more powerfully than unfamiliar voices
- This supports practices of encouraging family communication and familiar auditory environments in ICU
Summary
| Aspect | In Coma |
|---|---|
| ARAS (arousal) | Severely disrupted |
| Amygdala (emotional salience) | May remain active via thalamo-amygdala shortcut |
| Hypothalamus (autonomic emotion) | Often preserved if lesion is rostral |
| Papez circuit (emotional memory loop) | Variable - depends on lesion location |
| Conscious emotional experience | Absent (by definition) |
| Subcortical emotional responses | Can persist - autonomic, hormonal |
| Response to familiar emotional stimuli | Detectable by fMRI and EEG in some patients |
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - Limbic System (anatomy, amygdala, cingulate, hippocampus, hypothalamus)
- Adams and Victor's Principles of Neurology, 12th Edition - Physiology of the Limbic System; Emotional Disturbances
- Neuroanatomy through Clinical Cases, 3rd Edition - The Consciousness System; ARAS; coma localization
- Eickhoff SB et al. (2008) - fMRI reveals cognitive and emotional processing in a long-term comatose patient. Experimental Neurology. PMID 18789930
- Pruvost-Robieux E et al. (2025) - Emotion and familiarity in own-name oddball paradigms in disorders of consciousness. Neurophysiologie Clinique. PMID 39892079
CNS Examination
CNS neurological examination complete systematic approach clinical neurology 2024
Central Nervous System (CNS) Examination
The experienced neurologist uses a focused exam guided by the history, plus a screening exam to check the remainder of the nervous system. The goal is to confirm, refute, or modify hypotheses about lesion location and causation. - Bradley & Daroff's Neurology in Clinical Practice
Components of the CNS Examination
1. Mental Status
Level of Consciousness
- Alert, drowsy (lethargic), stuporous, comatose
- Use the Glasgow Coma Scale (GCS) for quantification: Eye (1-4) + Verbal (1-5) + Motor (1-6) = 3-15
Orientation
- Person, place, time, situation
Attention and Concentration
- Digit span (forward ≥5, backward ≥4)
- Serial 7s (subtract from 100)
- Months of year in reverse
Language (Screen for Aphasia)
| Aphasia Type | Fluency | Comprehension | Repetition | Lesion |
|---|---|---|---|---|
| Broca's | Non-fluent | Intact | Impaired | Inferior frontal (Broca's area, BA 44/45) |
| Wernicke's | Fluent (paraphasias) | Impaired | Impaired | Superior temporal (BA 22) |
| Global | Non-fluent | Impaired | Impaired | Large MCA territory |
| Conduction | Fluent | Intact | Impaired | Arcuate fasciculus |
| Anomic | Fluent | Intact | Intact | Variable |
Memory
- Immediate recall: repeat 3 words
- Short-term (5 min): recall those 3 words after delay
- Long-term: remote personal and public events
Cognitive Screening
- MMSE (Mini-Mental State Examination): 0-30; <24 suggests cognitive impairment
- MoCA (Montreal Cognitive Assessment): more sensitive; 0-30; <26 abnormal
Other Higher Cortical Functions
- Praxis: demonstrate brushing teeth, saluting (screens for apraxia - parietal lobe)
- Neglect: double simultaneous stimulation (touch both hands - parietal lesion causes extinction contralaterally)
- Frontal lobe: go-no-go tasks, Luria sequences, abstract thinking
- Calculation, right-left orientation, finger naming (Gerstmann's syndrome: angular gyrus)
2. Cranial Nerve Examination
| CN | Name | Tests | Key Findings |
|---|---|---|---|
| I | Olfactory | Identify smell (coffee, toothpaste) with eyes closed, each nostril | Anosmia: frontal lobe meningioma, Parkinson's, post-viral, head injury |
| II | Optic | Visual acuity (Snellen); visual fields by confrontation; fundoscopy; swinging flashlight test (RAPD) | Optic neuritis, papilloedema, visual field defects |
| III | Oculomotor | Pupil size/reactivity; eyelid (ptosis); adduction/elevation/depression of eye | Dilated pupil + ptosis + "down-and-out" eye: CN III palsy (uncal herniation) |
| IV | Trochlear | Downward/inward gaze; ask about vertical diplopia | Head tilt (away from lesion); worse on down-gaze |
| V | Trigeminal | Pinprick/touch: ophthalmic, maxillary, mandibular divisions bilaterally; corneal reflex (afferent limb); jaw clench (masseter) | Loss of corneal reflex, facial numbness, jaw deviation to weak side |
| VI | Abducens | Lateral gaze; ask about horizontal diplopia | Failure of abduction → convergent squint; false localizing sign (raised ICP) |
| VII | Facial | Raise eyebrows; close eyes tightly; show teeth; puff cheeks | UMN lesion: lower 2/3 weakness (forehead spared); LMN lesion: entire hemiface (Bell's palsy) |
| VIII | Vestibulocochlear | Whispered voice; finger rub; Rinne (AC vs BC); Weber (lateralizes) | Sensorineural vs conductive hearing loss |
| IX/X | Glossopharyngeal / Vagus | Palate elevation (say "Aah"); gag reflex; voice quality; swallowing | Uvula deviation away from lesion; dysphonia, dysphagia |
| XI | Accessory | Shoulder shrug (trapezius); head rotation against resistance (SCM) | Weakness of SCM → cannot turn head toward lesion side |
| XII | Hypoglossal | Tongue protrusion; tongue movements | Deviation toward lesion side (LMN); toward opposite side (UMN) |
Pupil Assessment in Detail
- Parasympathetic (pupilloconstriction): CN III - runs on the outside of the nerve; compressed first in CN III palsy (blown pupil)
- Sympathetic (pupillodilation): hypothalamus → ciliospinal center (C8-T2) → superior cervical ganglion → pupil; loss = Horner's syndrome (miosis + ptosis + anhidrosis)
| Pupil Finding | Interpretation |
|---|---|
| Unilateral dilated, unreactive | CN III compression (uncal herniation, posterior communicating artery aneurysm) |
| Bilateral dilated, unreactive | Severe midbrain damage, atropine, deep anesthesia |
| Bilateral pinpoint, still reactive | Pontine lesion (destroys sympathetics; parasympathetics intact) |
| RAPD (afferent defect) | Optic nerve or severe retinal disease ipsilateral |
| Horner's syndrome | Disruption of sympathetic pathway at any level |
3. Motor Examination
Inspection
- Muscle wasting/atrophy (LMN lesion, disuse, myopathy)
- Fasciculations at rest (LMN lesion, especially motor neuron disease)
- Involuntary movements:
| Movement | Character | Association |
|---|---|---|
| Tremor (resting) | 4-6 Hz, pill-rolling | Parkinson's disease |
| Tremor (intention) | Worse approaching target | Cerebellar disease |
| Tremor (postural) | With maintained posture | Essential tremor |
| Chorea | Random, flowing, non-patterned | Huntington's, Sydenham's |
| Athetosis | Slow, writhing, distal | Basal ganglia lesions |
| Myoclonus | Sudden, brief jerks | Metabolic, epileptic |
| Dystonia | Sustained muscle contractions → abnormal postures | Idiopathic, drug-induced |
| Tics | Patterned, semi-voluntary, suppressible | Tourette's |
Tone
| Tone Type | Character | Lesion |
|---|---|---|
| Normal | Slight, smooth resistance | - |
| Spasticity | Velocity-dependent; "clasp-knife" | Corticospinal (UMN) |
| Rigidity | Uniform resistance in all directions; "lead-pipe" | Extrapyramidal (basal ganglia) |
| Cogwheel rigidity | Ratchety interruptions on passive movement | Parkinsonism |
| Paratonia (Gegenhalten) | Fluctuating resistance | Frontal lobe; difficulty relaxing |
| Hypotonia/Flaccidity | Reduced or absent resistance | LMN, cerebellar, acute UMN |
Strength (MRC Scale)
| Grade | Description |
|---|---|
| 0 | No contraction |
| 1 | Flicker/trace of contraction, no joint movement |
| 2 | Movement possible only with gravity eliminated |
| 3 | Movement against gravity, not against resistance |
| 4- / 4 / 4+ | Movement against mild / moderate / strong resistance |
| 5 | Full normal power |
| Pattern | Localization |
|---|---|
| Unilateral UE extensors + LE flexors (pyramidal) | Corticospinal tract lesion |
| Proximal bilateral | Myopathy |
| Distal bilateral | Peripheral neuropathy |
| Single nerve distribution | Mononeuropathy |
| Dermatomal/Root pattern | Radiculopathy |
4. Reflexes
Deep Tendon Reflexes (DTRs)
| Reflex | Nerve Root | Technique |
|---|---|---|
| Biceps | C5-C6 | Tap biceps tendon |
| Brachioradialis (Supinator) | C5-C6 | Tap brachioradialis |
| Triceps | C7 | Tap triceps tendon |
| Knee (Patellar) | L3-L4 | Tap patellar tendon |
| Ankle (Achilles) | S1-S2 | Tap Achilles tendon |
- 0 = absent (even with reinforcement)
- 1+ = diminished
- 2+ = normal
- 3+ = brisk
- 4+ = clonus
Superficial Reflexes
| Reflex | Method | Normal | Significance if absent |
|---|---|---|---|
| Abdominal (upper T8-T10 / lower T10-L1) | Stroke each abdominal quadrant | Umbilicus moves toward stimulus | Absent in corticospinal lesions, multiple sclerosis |
| Cremasteric | Stroke inner thigh | Ipsilateral testicular elevation (L1-L2) | Absent in UMN lesion or L1-L2 root |
| Plantar | Stroke lateral sole, curve inward | Plantar flexion of toes | Absent in S1 lesion |
Pathological Reflexes (UMN Signs)
| Sign | Test | Positive Response | Significance |
|---|---|---|---|
| Babinski | Stroke lateral sole with blunt object | Extension of big toe + fanning of other toes | Corticospinal tract lesion (always abnormal in adults) |
| Hoffmann | Flick distal phalanx of middle finger | Flexion of thumb + index finger | UMN lesion in upper limbs (C-spine or intracranial) |
| Oppenheim | Firm pressure down tibia | Same as Babinski | UMN lesion |
| Gordon | Squeeze calf | Same as Babinski | UMN lesion |
| Chaddock | Stroke lateral foot/ankle | Same as Babinski | UMN lesion |
5. Sensory Examination
Primary Modalities
| Modality | Pathway | Test | Tract |
|---|---|---|---|
| Light touch | Anterior spinothalamic + dorsal column | Cotton wool / fingertip | Both |
| Pain | Lateral spinothalamic | New pin (do not reuse) | Lateral spinothalamic |
| Temperature | Lateral spinothalamic | Tuning fork (warm/cold) or warm/cold water | Lateral spinothalamic |
| Vibration | Dorsal column-medial lemniscus | 128-Hz tuning fork to bony prominence (great toe, medial malleolus, shin, fingers) | Dorsal columns |
| Proprioception (Joint Position Sense) | Dorsal column-medial lemniscus | Grasp digit laterally, move up/down 1-2mm | Dorsal columns |
Cortical Sensation
| Test | Parietal Function |
|---|---|
| Double simultaneous stimulation | Touch both hands - contralateral sensory extinction with parietal lesion |
| Two-point discrimination | Discriminate two closely placed stimuli as separate |
| Stereognosis | Identify object by touch alone (coin, key) |
| Graphesthesia | Identify number/letter written on skin |
6. Coordination
Upper Limb Tests
- Finger-nose-finger: touch own nose → examiner's moving finger → repeat. Look for intention tremor, dysmetria (past-pointing)
- Finger-nose (eyes closed): proprioception + cerebellar
- Rapid alternating movements (dysdiadochokinesia): tap index finger on thumb rapidly. Slow = pyramidal; imprecise/irregular = cerebellar
Lower Limb Tests
- Heel-knee-shin: slide heel from knee down shin smoothly
- Toe-to-examiner's-finger: raise leg, touch examiner's finger with great toe
- Dysdiadochokinesia
- Ataxia (truncal)
- Nystagmus (horizontal, fast phase toward lesion)
- Intention tremor
- Slurred speech (dysarthria / scanning speech)
- Hypotonia
7. Gait Examination
| Gait Pattern | Features | Localization |
|---|---|---|
| Hemiplegic (circumduction) | Arm flexed, leg circumducts outward | Contralateral corticospinal |
| Spastic (scissor) | Both legs stiff, small steps, crossing | Bilateral corticospinal (spinal cord) |
| Parkinsonian | Shuffling, small steps, stooped, reduced arm swing, festination | Basal ganglia |
| Cerebellar (ataxic) | Wide-based, staggering, irregular | Cerebellum / spinocerebellar tracts |
| Sensory ataxia | Wide-based, "stamping," looks at floor, worse in dark | Dorsal columns / peripheral neuropathy |
| Steppage (foot drop) | High stepping to clear foot off ground | Peripheral (common peroneal / L5) |
| Waddling | Pelvis drops on unsupported side (Trendelenburg) | Proximal muscle weakness (myopathy) |
| Apraxic | "Feet glued to floor," normal leg strength | Frontal lobe (normal pressure hydrocephalus) |
8. Signs of Meningeal Irritation
| Sign | Technique | Positive Finding |
|---|---|---|
| Neck stiffness | Passive neck flexion | Resistance / inability to flex chin to chest |
| Kernig's sign | Flex hip 90° then extend knee | Pain/spasm preventing full extension (>135°) |
| Brudzinski's sign | Passive neck flexion | Spontaneous hip/knee flexion |
| Jolt accentuation | Ask patient to shake head 2-3 Hz horizontally | Worsening headache (sensitive for bacterial meningitis) |
UMN vs. LMN: The Critical Distinction
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Reflexes | Hyperreflexia, clonus | Hyporeflexia / areflexia |
| Babinski | Present (extensor) | Absent |
| Wasting | Minimal (disuse) | Marked |
| Fasciculations | Absent | Present |
| Weakness distribution | Pyramidal pattern | Root / nerve distribution |
Anatomical Localization Summary
| Finding | Level |
|---|---|
| Hemiplegia + aphasia / hemianopia | Contralateral cerebral hemisphere |
| Hemiplegia + crossed cranial nerve palsy | Ipsilateral brainstem (e.g., Weber's syndrome: CN III palsy + contralateral hemiplegia = midbrain) |
| Quadriplegia + sensory level + UMN signs | Cervical spinal cord |
| Paraplegia + sensory level | Thoracic/lumbar cord |
| LMN + dermatomal sensory loss | Nerve root (radiculopathy) |
| Distal symmetric weakness + sensory loss | Peripheral neuropathy |
| Proximal weakness only, no sensory loss | Myopathy |
- Bradley and Daroff's Neurology in Clinical Practice - Chapter 1: Neurological Examination
- Harrison's Principles of Internal Medicine, 22nd Edition - Cranial Nerve, Motor, Sensory, Coordination, and Gait Examinations
- Goldman-Cecil Medicine - Cranial Nerve Examination and Pupillary Assessment in Coma
Why lichentenstein mesh is white in colour for hernia repair
why is polypropylene mesh white color Lichtenstein hernia repair material properties
polypropylene white colour chemistry polymer optical properties surgical mesh
Why Is the Lichtenstein Mesh White?
The Material: Polypropylene (PP)
Why Polypropylene Appears White: The Physics
1. Semicrystalline Microstructure - Light Scattering
- Snow white (ice crystals with air interfaces)
- Milk white (fat globule-water interfaces)
- Paper white (cellulose fibre interfaces)
2. No Chromophore Groups
3. Opacity Rather Than Transparency
4. Titanium Dioxide (TiO₂) Stabilizer
Why This Matters Clinically
| Property | Basis | Clinical Benefit |
|---|---|---|
| Semicrystalline structure | White colour, light scattering | High tensile strength; resists deformation under intra-abdominal pressure |
| No chromophores / pure hydrocarbon | No visible absorption | Chemically inert; resistant to body fluids, acids, alkalis |
| Hydrophobic surface | Non-polar C-H bonds | Resists bacterial colonisation; low infection risk |
| Monofilament knit | White fibres visible | Easy to inspect, cut to shape, and suture without fraying |
| Macroporous structure | Large pores in knit mesh | Allows fibroblast and tissue ingrowth (incorporated into host tissue) |
Other Mesh Colours and What They Mean
| Colour | Material | Example |
|---|---|---|
| White / off-white | Polypropylene (PP) | Prolene (Ethicon), Premilene (B Braun) |
| Blue | PP with blue dye (visibility aid) | Parietene (Covidien) - blue threads added for intraoperative visibility |
| Titanium-grey | Titanized PP (TiMesh) | PP coated with titanium to reduce foreign body reaction |
| Translucent / yellow | Polyester (Mersilene) | Different polymer - aromatic ester bonds give slightly yellow hue |
| Black | Carbon-reinforced or charcoal meshes | Experimental/specialty applications |
Summary
- Polypropylene is intrinsically white in its native semicrystalline form
- The semicrystalline microstructure scatters all wavelengths of visible light equally (Mie scattering)
- PP has no chromophore groups - its C-C and C-H bonds absorb only UV, not visible light
- Optional TiO₂ stabilizer reinforces the white opacity and provides UV protection
- Bailey and Love's Short Practice of Surgery, 28th Edition - Lichtenstein's Repair
- Wikipedia: Polypropylene - Optical Properties ("It is a white, mechanically rugged material")
- Which mesh for hernia repair? (PMC) - material properties comparison
How do we see secretion on ventilator waveforms and loop with images
ventilator waveform secretions sawtooth flow-volume loop images airway secretions ICU
https://pmc.ncbi.nlm.nih.gov/articles/PMC7782574
sawtooth pattern ventilator flow waveform secretions airway pressure time scalar loop site:pmc.ncbi.nlm.nih.gov OR site:journals.lww.com
ventilator sawtooth waveform secretions image flow time scalar expiratory limb serrations
Secretions on Ventilator Waveforms and Loops
Understanding the Basics: Scalars vs Loops
| Type | What it plots | Purpose |
|---|---|---|
| Scalar (Flow-Time) | Flow (L/min) vs Time | See airflow delivery and resistance over time |
| Scalar (Pressure-Time) | Airway pressure vs Time | See compliance, PIP, Pplat |
| Scalar (Volume-Time) | Volume (mL) vs Time | See tidal volume delivery and leaks |
| Loop (Flow-Volume) | Flow vs Volume per breath | Assess mechanics, obstruction, secretions |
| Loop (Pressure-Volume) | Pressure vs Volume per breath | Assess compliance, overdistension |
The Hallmark of Secretions: The Sawtooth Pattern
Why It Happens
- The pattern appears and disappears dynamically as secretions move
- It resolves after suctioning - this is the key diagnostic confirmation
- It can appear on both inspiratory and expiratory limbs because secretions obstruct airflow in both directions (unlike bronchospasm which primarily affects expiration)
1. Flow-Time Scalar: Sawtooth Oscillations
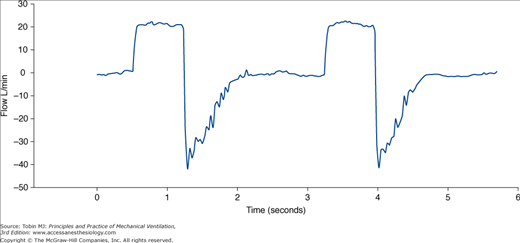
What to Look For on the Flow-Time Scalar:
- Inspiratory limb: smooth square (VC mode) or decelerating (PC/PS mode)
- Expiratory limb: smooth exponential decay back to zero
- Sawtooth/serrated oscillations - repetitive spikes superimposed on the expiratory flow curve
- Present predominantly on the expiratory limb (where passive airflow moves past secretion pools)
- Can also appear on the inspiratory limb if secretions are thick and bilateral
- The oscillations are irregular and variable between breaths (unlike the regular pattern of circuit water, which tends to be more rhythmic)
- Reduced peak expiratory flow rate (PEFR) - overall expiratory flow is reduced
- Expiratory flow takes longer to return to baseline (prolonged expiratory time) due to increased resistance
Normal Expiratory Flow:
Flow ↓
|╲
| ╲___________ ← smooth exponential decay
| ╲__→ baseline (zero)
With Secretions:
Flow ↓
|╲
| ╲/\/\/\/\/\/\/╲___ ← sawtooth oscillations
| ╲__→ baseline
2. Pressure-Time Scalar

- Peak Inspiratory Pressure (PIP) increases - more pressure needed to push air past the obstruction
- Plateau pressure (Pplat) remains normal (unchanged) - this is the critical distinction from decreased compliance, where Pplat rises too
- The difference ΔP = PIP - Pplat widens, indicating increased airway resistance (Raw)
- In severe secretion plugging, PIP may spike sharply
Key distinction:
- PIP↑ + Pplat normal → increased airway resistance (secretions, bronchospasm, kinked ETT)
- PIP↑ + Pplat↑ → decreased compliance (pneumothorax, pulmonary oedema, ARDS)
3. Volume-Time Scalar
- Expiratory curve is prolonged - returns to baseline more slowly
- May not return fully to zero before next breath → auto-PEEP / air trapping
- Reduced exhaled tidal volume if secretions cause a significant plug (some gas stays trapped)
4. Flow-Volume Loop: Reverberations on the Expiratory Limb
Normal Flow-Volume Loop:
- Inspiratory limb (above x-axis): smooth arc peaking at peak inspiratory flow
- Expiratory limb (below x-axis): smooth curve from peak expiratory flow back to zero volume
With Secretions - Three Key Changes:
"A sawtooth pattern is observed in both inspiratory and expiratory limbs and indicates the presence of secretions in the airways." - Respiratory Mechanics, PMC 2021
"The flow-volume curve can provide an indication of excessive secretions more reliably than clinical examination, with the presence of excessive secretions in the airways producing a sawtooth pattern on both the inspiratory and expiratory V̇-V curves." - Oxford Textbook of Critical Care (cited in PMC 2021)
Normal F-V Loop: With Secretions:
Flow↑ Flow↑
___ __
/ \ Insp /\/\/\ ← sawtooth on insp
/ \ /
------Volume→ --------Volume→
\ / \
\___/ Exp \/\/\/_ ← sawtooth on exp
(reduced PEFR, scooped)
5. Pressure-Volume (P-V) Loop
- The inspiratory and expiratory limbs separate further
- Increased expiratory resistance causes the expiratory limb to bulge to the left
- Increased inspiratory resistance bulges to the right
- Expiratory resistance is more commonly elevated with secretions
Differentiating Secretions from Other Causes of Sawtooth
| Feature | Secretions | Circuit Water | Bronchospasm | Kinked ETT |
|---|---|---|---|---|
| Sawtooth on F-T scalar | Yes | Yes | No | No |
| Sawtooth on F-V loop | Both limbs | Both limbs | Expiratory only | Variable |
| Clears with suctioning | Yes | No | No | No |
| Clears after tilting circuit | No | Yes | No | No |
| Resolves with bronchodilator | No | No | Yes | No |
| Resolves with repositioning ETT | No | No | No | Yes |
| PIP increase | Yes (moderate) | Mild | Yes (significant) | Yes (significant) |
| Pplat increase | No | No | No | No |
The key bedside test: perform endotracheal suctioning - if the sawtooth pattern disappears, secretions were the cause. This was validated in a landmark study (Jubran & Tobin, 1994, Chest) with sensitivity 76-86% and specificity 86-90%.
Summary: What to Observe on Each Graphic
| Waveform | Sign of Secretions |
|---|---|
| Flow-Time scalar | Sawtooth oscillations on expiratory limb (most sensitive) |
| Pressure-Time scalar | PIP↑, Pplat unchanged → ΔP widened |
| Volume-Time scalar | Prolonged expiration; possible air trapping |
| Flow-Volume loop | Sawtooth/reverberations on both limbs; reduced PEFR; scooped expiratory limb |
| Pressure-Volume loop | Wider loop; expiratory limb bulging left |
Clinical Action When Secretion Pattern Is Identified
- Confirm - check if pattern correlates with auscultation (coarse crackles, rhonchi)
- Suction endotracheally - watch for waveform normalisation
- Instill saline (if secretions thick) then suction
- Increase humidification - ensure heated humidifier or HME is working
- Chest physiotherapy / positioning - lateral positioning, vibration
- Mucolytics (e.g., N-acetylcysteine, nebulised hypertonic saline) if secretions are very tenacious
- Reassess waveforms post-suctioning to confirm resolution
- Tobin MJ: Principles and Practice of Mechanical Ventilation, 3rd Edition (McGraw-Hill) - sawtooth waveform image
- PMC: Respiratory Mechanics, 2021 - sawtooth = secretions on both F-V limbs
- PMC: The Basics of Ventilator Waveforms, 2021 - loop patterns
- Jubran A & Tobin MJ (1994): Flow-volume curves in detecting secretions in ventilator-dependent patients. Chest - Sensitivity 76-86%, Specificity 86-90%
Pneumothorax after subclavian centra line insertion
pneumothorax after subclavian central line insertion incidence management prevention ultrasound
"subclavian" AND "central venous catheter" AND "pneumothorax"
Pneumothorax After Subclavian Central Line Insertion
Why the Subclavian Route Carries the Highest Risk
Relevant Anatomy
- The pleural dome rises above the clavicle by ~2.5 cm at the midpoint
- The lung apex occupies the space just posterior and inferior to the vein
- The subclavian artery lies posterior to the vein; the phrenic nerve and thoracic duct (left side) lie in close proximity
- There is no fat or tissue buffer between the vein and the pleura - they are essentially adjacent structures
Incidence
| Access Site | Pneumothorax Rate (Landmark) | With Ultrasound Guidance |
|---|---|---|
| Subclavian vein | 1.5% - 12% (most studies 2-3%) | ~0% (Fragou 2011 RCT) |
| Internal jugular vein | 0.2 - 0.5% | <0.1% |
| Femoral vein | ~0% | ~0% |
"The most common technical complication of central venous catheter placement is pneumothorax, which can happen with either subclavian or internal jugular access but is more common with subclavian access (1.5% vs. 0.5%)." - Fischer's Mastery of Surgery, 8th Edition
"The reported risk ranges from 2% to 12% (most studies <3%) when using anatomic landmarks for guidance. Subclavian catheterization carries a higher risk than internal jugular catheterization." - Fishman's Pulmonary Diseases and Disorders
- Emergency situations
- Large catheter size (dialysis catheters)
- Multiple needle passes (risk increases sixfold with ≥3 attempts)
- Operator inexperience
- Patient anatomy (obesity, short neck, barrel chest from COPD)
Mechanism of Injury
- Direct pleural puncture by the introducer needle - the most common mechanism. The needle tip penetrates the parietal pleura, creating a pleural breach.
- Guidewire or dilator injury - the guidewire or dilator kinks at the subclavian/SVC junction and deflects downward into the lung parenchyma.
- Delayed presentation - a micro-perforation in the pleura sealed temporarily by clot or tissue, which later decompresses - this can present 12-48 hours post-procedure. Particularly dangerous in mechanically ventilated patients where positive pressure can convert a small pneumothorax to a tension pneumothorax.
Clinical Presentation
Onset Timing
- Immediate (most common): oxygen desaturation, dyspnoea, or respiratory distress within minutes of line insertion
- Delayed (up to 24-48 hours): insidious onset of respiratory compromise, particularly on positive pressure ventilation
Symptoms and Signs
| Feature | Finding |
|---|---|
| Symptoms | Chest pain (ipsilateral, pleuritic), dyspnoea, shoulder tip pain |
| General | Tachypnoea, tachycardia, hypoxia (SpO₂ drop) |
| Inspection | Reduced chest expansion on affected side |
| Palpation | Trachea deviation away (tension), reduced vocal fremitus |
| Percussion | Hyper-resonance ipsilateral |
| Auscultation | Reduced or absent breath sounds ipsilateral |
Signs of Tension Pneumothorax (Emergency)
- Severe respiratory distress and hypoxia
- Hypotension - impaired venous return, reduced cardiac output
- Tracheal deviation away from the affected side
- Distended neck veins (elevated JVP)
- Cardiovascular collapse if untreated
Tension pneumothorax on the ventilated patient may present with sudden rise in peak airway pressure, falling tidal volumes, and haemodynamic deterioration before clinical signs are apparent.
Radiological Diagnosis
Chest X-Ray (Erect PA, or AP in ICU)
- Confirm catheter tip position (should be at SVC-RA junction)
- Exclude pneumothorax, haemothorax, hydrothorax
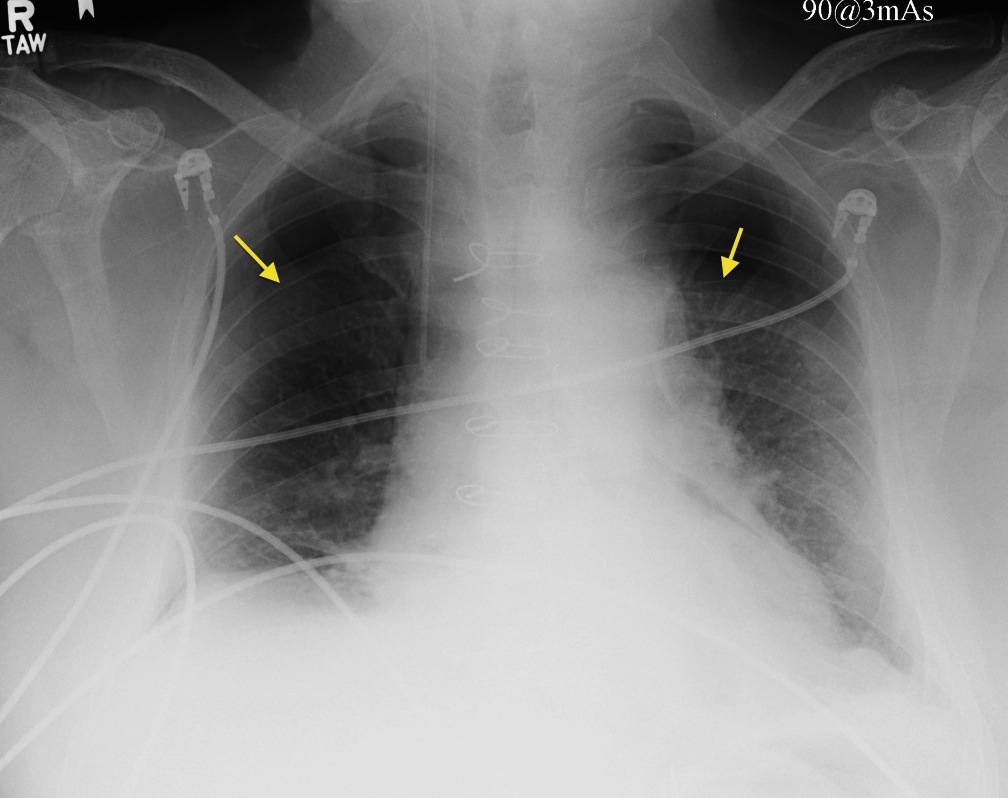
- Visceral pleural line - a thin white line (the visceral pleura) visible lateral to which there are no lung markings
- Absent lung markings in the periphery of the affected hemithorax
- Lung collapse toward the hilum (in larger pneumothorax)
- Mediastinal shift away from the pneumothorax (suggests tension)
- Deep sulcus sign (supine AP) - abnormally deep and lucent costophrenic angle
- Small: <20% or rim <2 cm (Collins formula: ≤15% collapse on CXR)
- Large: >20% or rim ≥2 cm
"A chest radiograph should be taken routinely to assess the position of a central venous catheter introduced via the subclavian or internal jugular route. This confirms placement of the catheter and can show potential complications of the procedure." - Roberts and Hedges' Clinical Procedures in Emergency Medicine
POCUS (Bedside Ultrasound)
| Ultrasound Sign | Normal | Pneumothorax |
|---|---|---|
| Lung sliding | Present (shimmering motion at pleural line) | Absent |
| B-lines | Present (comet-tail artefacts) | Absent |
| Seashore sign (M-mode) | Present | Absent → "Barcode/stratosphere sign" |
| Lung point | Not seen | Pathognomonic - junction between sliding and non-sliding lung |
Management
Decision Algorithm
Pneumothorax confirmed
↓
Is it TENSION? → YES → IMMEDIATE needle decompression
↓ NO (2nd ICS, MCL) then chest drain
↓
Patient on ventilator or symptomatic?
↓ YES → Chest drain insertion
↓ NO
↓
Small (<2cm rim on CXR) and stable?
↓ YES → Conservative (observation, high-flow O₂)
↓ NO
↓
Moderate/Large or worsening → Aspiration or chest drain
1. Tension Pneumothorax - Immediate Needle Decompression
- Needle decompression: 14-16G cannula inserted at 2nd intercostal space, mid-clavicular line (or 4th/5th ICS, anterior axillary line per ATLS)
- Insert perpendicular to skin, over the superior border of the rib (to avoid neurovascular bundle)
- A rush of air confirms diagnosis
- Followed immediately by chest drain insertion (needle decompression is temporary)
2. Chest Drain (Intercostal Tube Thoracostomy)
- Tension pneumothorax (after needle decompression)
- Large pneumothorax (>2 cm rim)
- Symptomatic pneumothorax
- Patient on mechanical ventilation (even small pneumothorax - high risk of tension)
- Bilateral pneumothorax
- Associated haemothorax
- Position: 4th or 5th ICS, anterior axillary line (triangle of safety)
- Size: 20-24F sufficient for simple pneumothorax; 28-32F if haemothorax present
- Connect to underwater seal drain; apply low-pressure suction (-20 cmH₂O) if not re-expanding
3. Simple Aspiration
- Small (< 2cm rim), minimally symptomatic, non-ventilated patient
- 14-16G cannula at 2nd ICS MCL, aspirate with 50mL syringe until resistance felt or 2.5L aspirated
- Repeat CXR to confirm re-expansion
- Lower re-expansion rate than chest drain; not appropriate for ventilated patients
4. Conservative Management with Observation
- Small pneumothorax (<15%), asymptomatic, not ventilated
- High-flow oxygen (15 L/min via non-rebreather mask) - increases rate of pleural air resorption ~4-fold by creating a nitrogen washout gradient
- Repeat CXR at 4-6 hours, then 24 hours
- Must admit for monitoring
Prevention
1. Ultrasound Guidance (Most Effective Single Intervention)
- Fragou 2011 RCT: landmark 4.8% pneumothorax vs. ultrasound 0%
- NICE (UK) and major society guidelines recommend ultrasound guidance for all elective CVC insertions
- In-plane (longitudinal): needle visualized along full length; preferred
- Out-of-plane (transverse): visualize needle tip at each advance
2. Correct Technique (Landmark Method)
- Patient positioning: Trendelenburg (15-25°), shoulder roll under spine, head turned away - distends the SCV and lowers the lung apex
- Needle angle: enter just lateral to the midpoint of the clavicle; advance parallel to the floor, hugging the inferior surface of the clavicle - never angle the needle inferiorly toward the lung
- Continuous negative suction on the syringe as you advance
- Limit attempts: stop at 2-3 unsuccessful passes; risk increases sixfold with ≥3 attempts
- Choose the right side when possible: left-sided approach risks thoracic duct injury; bilateral attempts risk bilateral pneumothorax
3. Site Selection
| Site | Pneumothorax Risk | Other Considerations |
|---|---|---|
| Subclavian | Highest (1.5-12%) | Lowest CLABSI; no compression if arterial puncture |
| Internal jugular | Lower (0.2-0.5%) | CLABSI risk higher; can compress arterial bleed |
| Femoral | Negligible | Highest CLABSI, DVT risk; not near pleura |
Other Thoracic Complications of Subclavian CVC (Differential Consideration)
| Complication | Mechanism | Presentation |
|---|---|---|
| Haemothorax | SCV laceration, subclavian artery puncture | Dullness on percussion, haemodynamic instability |
| Hydrothorax | IV fluid infused into pleural space (malpositioned catheter) | Dullness, gradual onset, detected on CXR |
| Chylothorax | Left subclavian - thoracic duct laceration | Milky/lymphatic fluid on drain; triglyceride-rich |
| Air embolism | Air enters open needle/hub during insertion | Mill-wheel murmur, sudden cardiovascular collapse |
| Cardiac tamponade | Guidewire/catheter perforation of SVC or right atrium | Beck's triad (hypotension, distended neck veins, muffled heart sounds) |
Key Takeaways
- Pneumothorax is the most common technical complication of subclavian CVC insertion (2-3% landmark; ~0% ultrasound-guided)
- Anatomy: the pleural dome and lung apex are directly adjacent to the subclavian vein - the needle must be kept parallel to the clavicle, not angled inferiorly
- Always check: mandatory post-procedure CXR to confirm tip position and exclude pneumothorax; POCUS is faster and more sensitive
- Ventilated patients: even a small pneumothorax mandates chest drain - positive pressure converts it to tension rapidly
- Tension pneumothorax: clinical emergency - decompress immediately, do not wait for imaging
- Ultrasound guidance: the single most effective preventive measure - reduces pneumothorax rate from 4.8% to 0% in RCTs
- Fishman's Pulmonary Diseases and Disorders - Iatrogenic Pneumothorax (Table 79-2)
- Fischer's Mastery of Surgery, 8th Edition - CVC Complications
- Roberts and Hedges' Clinical Procedures in Emergency Medicine - Mechanical Complications (Fig. 22.22)
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - CVC Placement
- Tsotsolis et al. - Pneumothorax as a complication of CVC insertion, Annals of Translational Medicine
Bell's palsy
"Bell's palsy" treatment prognosis
Bell's palsy 2024 2025 guidelines treatment corticosteroids antiviral diagnosis