Discuss the role of external and middle ear in the physiological
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer:
Role of the External and Middle Ear in the Physiology of Hearing
Overview
The external and middle ears together serve one primary physiological purpose: amplify sound and convert the mechanical energy of airborne sound waves into pressure changes in the fluid-filled inner ear - a process that sets the stage for the electrochemical transduction carried out by the cochlear hair cells. In the absence of these structures, nearly 99.9% of acoustical energy would be reflected at the air-fluid interface and never heard. Together, the eardrum and ossicles boost sound energy nearly 200-fold by the time it reaches the inner ear.
- Harrison's Principles of Internal Medicine, 22E, p. 287
- Costanzo Physiology, 7th Ed., p. 98
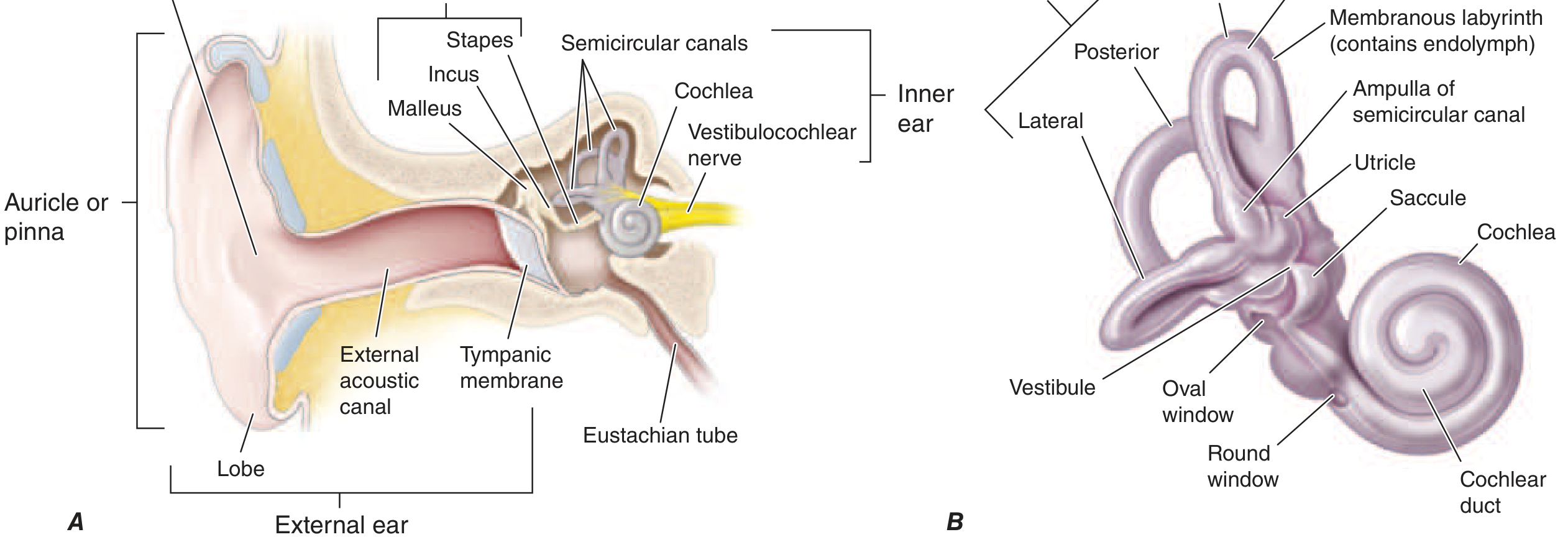
I. The External Ear
Components
- Pinna (auricle) - the cartilaginous, funnel-shaped outer structure
- External auditory canal (EAC) - approximately 2.5 cm long, ~2 cm³ in volume in adults
- Outer surface of the tympanic membrane
Functions
1. Sound Collection and Directional Funneling
The pinna collects sound waves and directs them through the ear canal, creating vibratory patterns on the eardrum. Its funnel shape is well-suited to capturing sound from the environment and channeling it inward.
2. Sound Localization
The pinna aids specifically in vertical localization of sound - i.e., determining whether a sound is above or below the listener. Its irregular contours create direction-dependent spectral cues (pinna-related transfer functions). It also preferentially amplifies high-frequency sounds over low-frequency ones.
3. Resonance Amplification
The external auditory canal functions as a closed-tube resonance chamber, amplifying frequencies in the range of 2000-5500 Hz (average resonant frequency approximately 2700 Hz, though this varies by individual). This resonance region importantly overlaps with the frequency range most critical for understanding speech. In effect, the external canal provides passive amplification precisely where the auditory system needs it most.
- K.J. Lee's Essential Otolaryngology, p. 289
II. The Tympanic Membrane
The tympanic membrane (eardrum) is the interface between the external and middle ear. It separates the air-filled external ear from the air-filled middle ear cavity. When sound waves impinge on it, it vibrates in response - and these vibrations are mechanically coupled to the ossicular chain.
Key anatomical point: although the total area of the adult tympanic membrane is 85-90 mm², only approximately 55 mm² (the lower two-thirds) vibrates effectively. This effective vibrating area is critical to understanding impedance matching (see below).
- K.J. Lee's Essential Otolaryngology, p. 290
III. The Middle Ear - Impedance Matching
The Core Problem
The inner ear (cochlea) is filled with fluid (perilymph). Sound travels through air in the external canal. The acoustic impedance of fluid is far greater than that of air. Without a mechanism to bridge this impedance mismatch, approximately 99.9% of sound energy would be reflected at the air-fluid interface - analogous to sound barely penetrating water when you shout into a pool.
The middle ear solves this with an impedance-matching mechanism that achieves approximately a 22:1 mechanical transformer ratio (~25 dB gain) through two distinct physical principles:
Mechanism 1: Area Effect of the Tympanic Membrane
The vibrating area of the tympanic membrane (~55 mm²) is much larger than the stapes footplate (~3.2 mm²). This concentrates the same total force applied to the large membrane onto the much smaller oval window, resulting in a 17:1 increase in pressure (force per unit area). This is the dominant contributor to impedance matching.
Mechanism 2: Lever Action of the Ossicular Chain
The three ossicles - malleus, incus, and stapes - form a lever system that rotates about an axis running from the anterior process of the malleus through the short process of the incus. The handle of the malleus is approximately 1.3 times longer than the long process of the incus. By the law of levers, this amplifies force at the stapes footplate by a factor of 1.3:1.
Combined transformer ratio: 17 × 1.3 = ~22:1 (approximately 25 dB of amplification).
Mechanism 3: Natural Resonance of the Outer and Middle Ears
The resonant properties of the outer and middle ears enhance sound transmission most efficiently in the range of 500-3000 Hz - exactly the frequency range most important for understanding speech.
Mechanism 4: Phase Difference Between Oval and Round Windows
The oval window (where the stapes footplate inserts) and round window lie at opposite ends of the cochlear fluid pathway. When sound impinges on the oval window, the resulting traveling wave reaches the round window out of phase. This phase difference contributes a small (~4 dB) boost in the normal ear.
- K.J. Lee's Essential Otolaryngology, p. 289-290
- Costanzo Physiology, 7th Ed., p. 98-99
IV. The Ossicular Chain in Detail
The ossicular chain - malleus, incus, and stapes - is the mechanical transmission line of the middle ear. Sound travels from the tympanic membrane → malleus (handle/manubrium) → incus (long process) → stapes → oval window → cochlear fluid.
Key mechanical notes:
-
The malleus and incus weigh approximately the same, but the stapes is about one-fourth the mass of the other two ossicles. This lower mass of the stapes facilitates transmission of higher frequencies.
-
The ossicular chain most efficiently transmits sound between 500 and 3000 Hz - the range of normal speech.
-
The stapes footplate rests in the oval window, sealed by the annular ligament. Its piston-like in-and-out movement generates pressure waves in the perilymph of the scala vestibuli.
-
K.J. Lee's Essential Otolaryngology, p. 289
-
Neuroscience: Exploring the Brain, 5th Ed., p. 1035
V. The Middle Ear Muscles and the Acoustic Reflex
Two muscles attach to the ossicles and modify sound transmission:
| Muscle | Nerve Supply | Attachment | Dominant Function |
|---|---|---|---|
| Tensor tympani | CN V (Trigeminal) | Malleus manubrium | Protects against self-generated sounds (vocalization, swallowing) |
| Stapedius | CN VII (Facial) | Stapes neck / annular ligament | Dominant reflex response to loud sounds |
The Acoustic (Attenuation) Reflex
When a loud sound is detected, both muscles contract reflexively, stiffening the ossicular chain and reducing sound conduction to the inner ear. This is called the acoustic reflex or attenuation reflex.
Key physiological roles:
- Protection - reduces cochlear exposure to potentially damaging loud sounds
- Frequency selectivity - attenuates low frequencies far more effectively than high frequencies, improving the ability to hear speech against background low-frequency noise
- Pre-vocalization reflex - the reflex activates a moment before speaking, preventing the speaker's own voice from sounding as loud as it would otherwise
- Dynamic range extension - by reducing saturation of inner ear receptors, the reflex extends the range of intensities the ear can process
Important limitation: The acoustic reflex has a latency of 30-100 msec. This means it cannot protect the cochlea from very sudden impulse sounds (e.g., a gunshot), where damage occurs before the muscles have time to contract.
In humans, unlike most other mammals, only the stapedius contracts reflexively in response to sound; the tensor tympani is not reliably activated by acoustic stimuli.
- Neuroscience: Exploring the Brain, 5th Ed., p. 1035-1036
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2, p. 623
VI. The Eustachian Tube - Pressure Regulation
The Eustachian tube connects the middle ear cavity to the nasopharynx. Its physiological roles in the middle ear include:
- Pressure equalization - it opens periodically (mainly during swallowing and yawning) to equalize air pressure in the middle ear cavity with ambient atmospheric pressure. Failure of this function leads to middle ear barotrauma (as occurs during rapid altitude changes).
- Ventilation - maintains aeration of the middle ear space, which is necessary for normal tympanic membrane and ossicular function.
- Drainage - allows secretions from the middle ear to drain into the nasopharynx via mucociliary clearance.
Without adequate Eustachian tube function, negative middle ear pressure builds up, the tympanic membrane retracts, and conductive hearing loss results.
VII. Summary of the Functional Sequence
Sound waves (air)
↓
Pinna - collects and focuses sound
↓
External auditory canal - resonant amplification (2-5.5 kHz)
↓
Tympanic membrane - vibrates in response to sound pressure
↓
Ossicular chain (malleus → incus → stapes)
- Impedance matching (area ratio 17:1 + lever ratio 1.3:1 = 22:1, ~25 dB gain)
↓
Stapes footplate → Oval window
↓
Fluid pressure wave in cochlea (perilymph)
↓
Basilar membrane traveling wave → Hair cell mechanotransduction (inner ear)
Clinical Relevance
Any disruption to the external or middle ear pathway produces conductive hearing loss - characterized by normal bone conduction with impaired air conduction (positive Rinne test, Weber lateralizes to the affected ear). Common causes include:
- Cerumen impaction (EAC blockage)
- Tympanic membrane perforation
- Ossicular chain disruption (trauma, cholesteatoma)
- Eustachian tube dysfunction / otitis media with effusion
Harrison's Principles of Internal Medicine, 22E, p. 288
Key Sources:
- Harrison's Principles of Internal Medicine, 22E (2025), Chapter 36: Physiology of Hearing
- Costanzo Physiology, 7th Ed. - Auditory Transduction
- K.J. Lee's Essential Otolaryngology, 11th Ed. - Outer Ear, Middle Ear
- Neuroscience: Exploring the Brain, 5th Ed. - The Acoustic Reflex
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 - Middle Ear Muscles
This is a shared conversation. Sign in to Orris to start your own chat.