A 47 year old young female presented with multiple petechial lesions over bilateral lower limbs with no joint pain gum bleeding fever with dengue ns1 igm negative nil comorbidities presented with hemogram 12.4/13.38/10000 ,peripheral smear suggestive of normocytic normochromic rbcs,wbc count raised on smear with neutrophillia .occasional neutrophil shows toxic granulations.platelet count markedly reduced on smear.occasional large platelets seen with mpv-10.9 N/L/E -82/10/01. No drug history no herbal medicine or ayurvedic medicine history
Reading File
Finding Sources
Finding Sources
Searching PubMed
immune thrombocytopenia diagnosis management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive information to provide a thorough clinical analysis. Let me compile a detailed response.
Clinical Analysis: 47-Year-Old Female with Petechiae and Isolated Thrombocytopenia
Interpreting the Hemogram
| Parameter | Value | Interpretation |
|---|---|---|
| Hb | 12.4 g/dL | Low-normal (mild anaemia) |
| MCV/MCH | Normocytic normochromic | No nutritional deficiency, no haemolysis |
| WBC | 10,000/μL (raised on smear) | Leukocytosis |
| Neutrophils | 82% | Neutrophilia |
| Toxic granulations | Occasional | Suggests active systemic response/sepsis/stress |
| Platelets | Markedly reduced | Thrombocytopenia (severe) |
| MPV | 10.9 fL (elevated) | Large platelets → increased platelet turnover |
| Occasional large platelets | Present | Consistent with peripheral destruction |
| Eosinophils | 1% | Normal |
| Lymphocytes | 10% | Relatively reduced (stress pattern) |
Key observation: The peripheral smear shows isolated thrombocytopenia with normocytic normochromic RBCs (no fragmented red cells/schistocytes), ruling out microangiopathic processes (TTP/HUS/DIC). The elevated MPV with large platelets signals increased platelet turnover — the bone marrow is producing platelets rapidly to compensate, pointing to peripheral destruction rather than decreased production.
Most Likely Diagnosis: Primary Immune Thrombocytopenia (ITP)
This is a diagnosis of exclusion — the characteristic scenario being isolated thrombocytopenia in the absence of an identifiable underlying cause or medication.
Supporting features in this patient:
- 47-year-old female (ITP has a female predominance in adults)
- Isolated thrombocytopenia — Hb and WBC in normal-to-mild range, no bicytopenia/pancytopenia
- Mucocutaneous bleeding (petechiae over bilateral lower limbs — gravity-dependent, classic)
- No joint pain, no fever → rules out vasculitis, dengue, septic etiology
- No drug/herbal medicine history → drug-induced thrombocytopenia excluded
- Dengue NS1 and IgM negative → dengue excluded
- Nil comorbidities
- Large platelets + elevated MPV → peripheral destruction pattern
- No schistocytes → TTP/HUS/DIC excluded
- Normocytic normochromic RBCs → no hemolysis, no megaloblastic change
"ITP typically presents as mild mucocutaneous bleeding and petechiae or incidental thrombocytopenia... Risk of bleeding is highest with platelet counts <30 × 10⁹/L." — Washington Manual of Medical Therapeutics
Diagnostic Algorithm
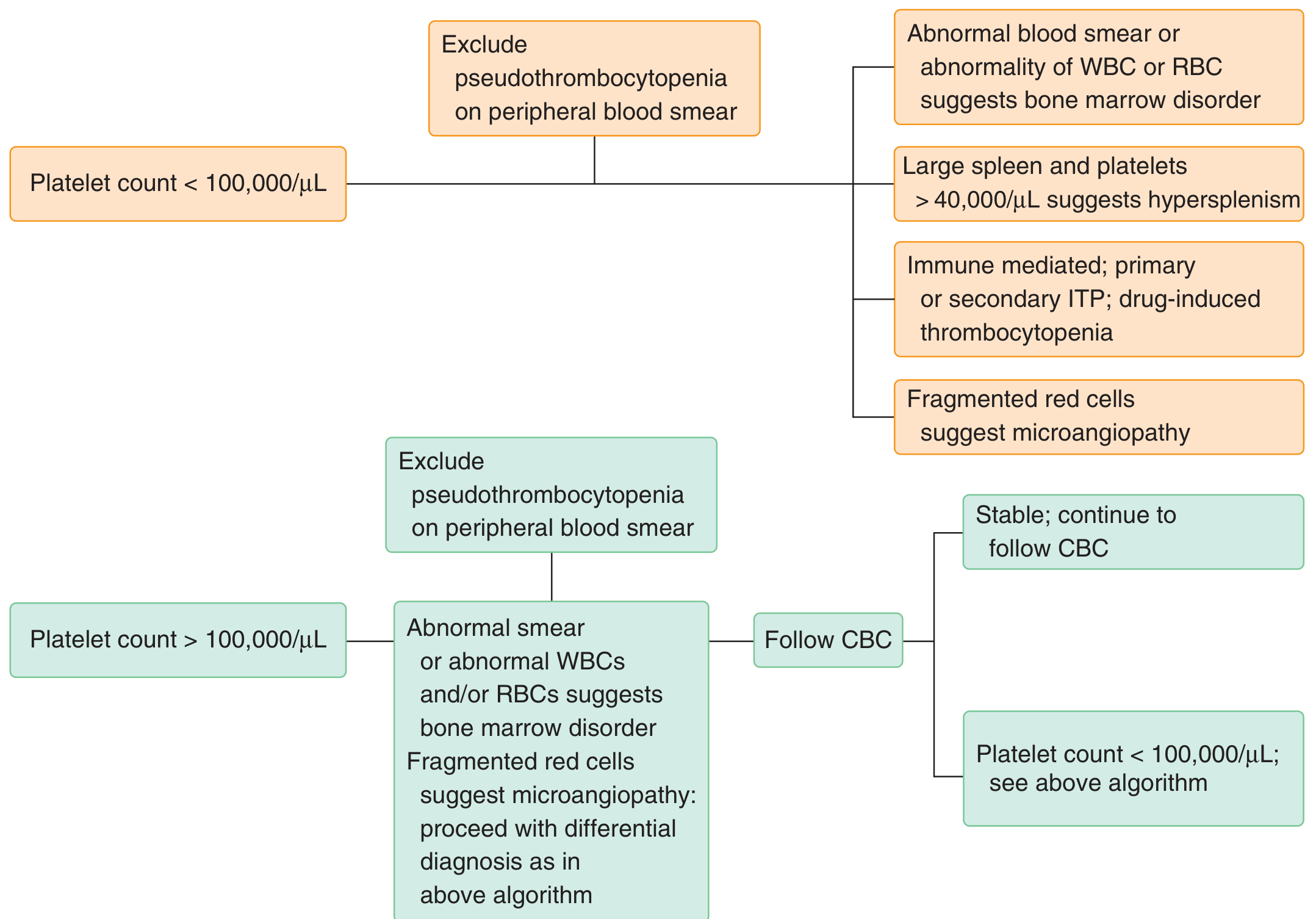
Goldman-Cecil Medicine — Systematic approach to evaluation of thrombocytopenia
Differential Diagnoses to Exclude
| Condition | Against It in This Case |
|---|---|
| Dengue | NS1 and IgM negative |
| TTP/HUS | No schistocytes, no renal failure, no fever/neurological signs |
| DIC | No coagulopathy history, no sepsis picture, no schistocytes |
| Drug-induced thrombocytopenia | No drug/herbal history |
| SLE | No joint pain, no rash (need ANA to formally exclude) |
| Antiphospholipid syndrome | Possible secondary ITP cause — needs APLA screen |
| HIV/HCV | Need serology to exclude as cause of secondary ITP |
| Hematological malignancy | Normocytic normochromic smear, no blasts, no lymphadenopathy mentioned |
| Hypersplenism | Usually platelet count >40,000; no splenomegaly mentioned |
| Pseudothrombocytopenia | Platelet clumping on smear absent — confirmed true thrombocytopenia |
The neutrophilia with toxic granulations is notable. In the context of ITP, this may represent a stress leukocytosis or a concurrent/triggering infection. However, no fever is reported. This warrants attention — consider checking CRP/ESR and blood culture to exclude an underlying infection that could be driving secondary ITP (e.g., H. pylori, viral).
Recommended Workup
To exclude secondary ITP causes (mandatory before labelling as primary ITP):
- HIV ELISA — secondary ITP is a common early presentation of HIV
- HCV antibody / HBsAg — hepatitis-related ITP
- ANA, anti-dsDNA — exclude SLE
- APLA panel (lupus anticoagulant, anticardiolipin, anti-β2GPI) — exclude antiphospholipid syndrome
- H. pylori (stool antigen or urea breath test) — eradication can resolve thrombocytopenia in up to 50% of H. pylori-associated ITP
- TSH — thyroid disorders can cause thrombocytopenia
- Coagulation profile (PT/aPTT) — to exclude DIC/coagulopathy
- LFT + renal function — baseline; assess for chronic liver disease/portal hypertension
- Peripheral smear review — confirm no blasts, no schistocytes (already done ✓)
- Reticulocyte count — assess for haemolysis
- LDH, bilirubin, haptoglobin — to definitively exclude haemolytic process
- USG abdomen — assess spleen size (hypersplenism vs. ITP)
Bone marrow examination: Not routinely needed for straightforward ITP in adults. However, given the patient's age (47 years), elevated WBC with neutrophilia and toxic granulations (atypical features), a bone marrow aspiration and biopsy should be considered if:
- No response to initial ITP treatment within 4 weeks
- Other CBC abnormalities develop
- Atypical peripheral smear features emerge
Management
Per Washington Manual and Harrison's principles:
Step 1 — Assess bleeding severity:
The platelet count is "markedly reduced." Risk of spontaneous bleeding is high if count <30 × 10⁹/L. Petechiae without active mucosal bleeding or wet purpura = dry purpura (lower risk).
First-line therapy (if treatment indicated — platelet count likely <30,000 or symptomatic):
| Drug | Dose | Notes |
|---|---|---|
| Dexamethasone | 40 mg orally × 4 days (preferred) | Faster platelet response than prednisone |
| OR Prednisone | 1 mg/kg/day with prolonged taper | |
| IVIG | 1 g/kg × 1–2 doses | If rapid response needed (e.g., bleeding, surgery) |
- 30–40% of patients develop relapsed/refractory ITP after initial response.
Second-line therapy (if relapse/refractory):
- Rituximab (anti-CD20) — ~25% durable remission at 12 months
- TPO receptor agonists — Romiplostim (SC weekly), Eltrombopag (oral daily), Avatrombopag (oral daily) — >90% platelet improvement
- Splenectomy — ~2/3 achieve durable complete response; requires pre-op vaccination (pneumococcal, meningococcal, Hib)
- Fostamatinib (Syk inhibitor) — for multiply refractory cases
If H. pylori positive: Eradication therapy (PPI + amoxicillin + clarithromycin × 14 days) before immunosuppression — can normalize platelets without steroids.
Clinical Pearls for This Case
- The leukocytosis with neutrophilia and toxic granulations in the absence of fever is unusual for uncomplicated primary ITP. This raises the possibility of a triggering infection (even subclinical) — check H. pylori, blood culture if CRP elevated.
- MPV 10.9 fL (elevated) with large platelets = classic ITP pattern of peripheral destruction with compensatory megakaryocytic hyperplasia.
- Bilateral lower limb petechiae follow gravity-dependent venous pressure distribution — textbook presentation of platelet-type bleeding.
- No joint pain, no gum bleeding, no fever cleanly excludes dengue, vasculitis, and most secondary causes clinically — but serologic workup is still mandatory.
- Do not transfuse platelets empirically in ITP — transfused platelets are destroyed rapidly by the same mechanism and may worsen autoimmune response. Reserve for life-threatening bleeding.
— Goldman-Cecil Medicine, p. 809; Washington Manual of Medical Therapeutics, p. 757–758; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.