Intervensional cardiology all hard wares
Reading File
Finding Sources
Finding Sources
Searching the Web
interventional cardiology hardware devices equipment complete overview 2024
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Now I have everything I need for a comprehensive, well-illustrated answer. Here is the complete guide to all interventional cardiology hardware:
Interventional Cardiology: All Hardware
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 287
Historical Background
PTCA (percutaneous transluminal coronary angioplasty) was introduced by Andreas Gruentzig in 1977. Coronary stents arrived in 1994, reducing acute thrombosis and restenosis by half. Drug-eluting stents (DES) followed in 2003, further slashing restenosis rates. Today, PCI is performed on >900,000 patients/year in the US alone.
CATEGORY 1: Vascular Access Hardware
Arterial Sheath (Introducer Sheath)
- Inserted into the radial artery (preferred, less bleeding risk) or femoral artery
- Provides a hemostatic valve and port for catheter exchange
- French sizes: 5F-8F (coronary); 14F-20F+ (structural heart/TAVR)
- Radial access has become dominant due to reduced access-site bleeding
Arteriotomy Closure Devices
- Collagen-based (e.g., Angio-Seal): plug seals femoral arteriotomy
- Suture-based (e.g., Perclose ProGlide): pre-placed suture closes the arteriotomy
- Clip-based (e.g., StarClose): nitinol clip apposition
- Used after femoral access; radial access uses compression bands (e.g., TR Band)
CATEGORY 2: Catheters
Guiding Catheter
- The "workhorse" catheter - sits in the coronary ostium
- Provides coaxial support and delivers contrast + devices
- Multiple tip shapes: Judkins Left (JL), Judkins Right (JR), Amplatz, XB/EBU (extra backup), AL, AR
- Selection depends on aortic root size, coronary anatomy, and access site
Diagnostic Catheter
- Used for coronary angiography only (no intervention)
- Thinner walls, smaller lumen - not suitable for device delivery
- Examples: Judkins, Tiger, Ikari, Radifocus
Microcatheter
- Delivered over a guidewire to chronic total occlusions (CTOs) or complex anatomy
- Enables guidewire exchange, contrast injection distally, and increased torque transmission
- Examples: Finecross, Corsair Pro, Turnpike, Teleport
Balloon Catheter (see Category 4 below)
Aspiration Catheter
- Manual suction device (e.g., Export AP) to aspirate thrombus in STEMI
- Now less routinely used (TASTE and TOTAL trials showed no mortality benefit; risk of stroke with routine use)
CATEGORY 3: Guidewires
The guidewire is passed through the guiding catheter and navigated across the coronary stenosis under fluoroscopy. All other devices are then advanced over it ("monorail" or "over-the-wire" systems).
| Property | Types/Examples |
|---|---|
| Workhorse wires (low stenosis) | BMW Universal, Runthrough NS, Fielder XT-R |
| Support wires (tortuous anatomy) | Iron Man, Mailman, Grand Slam |
| CTO wires (crossing occlusions) | Gaia series, Confianza Pro, Fielder XT, Hornet |
| Polymer-tipped (atraumatic) | Pilot series, Whisper |
| Pressure wires (FFR/iFR measurement) | PressureWire X (Abbott), Verrata Plus (Philips/Volcano) |
Key specs: diameter (0.014" standard), stiffness, tip load, hydrophilic vs. hydrophobic coating, torquability.
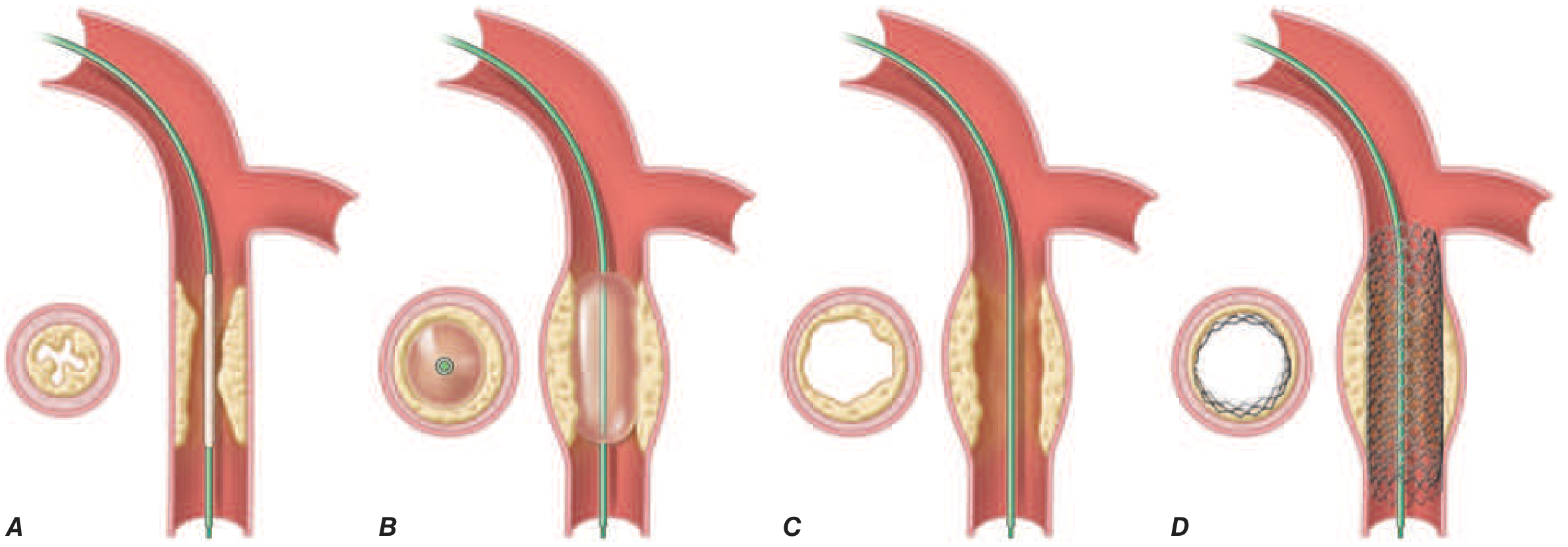
CATEGORY 4: Balloon Catheters
Balloon Angioplasty - Mechanism
The balloon is advanced over the guidewire, positioned across the stenosis, then inflated (typically 6-20 atm) to stretch and disrupt the plaque. This expands the lumen and creates small controlled dissections that are then scaffolded by stenting.
Types of Balloon Catheters
| Type | Purpose | Notes |
|---|---|---|
| Semi-compliant | Pre-dilation, post-dilation, general use | Expands beyond nominal size at higher pressures |
| Non-compliant (NC) | High-pressure stent expansion, resistant lesions | Minimal size change with pressure; avoids geographic miss |
| Drug-coated balloon (DCB) | In-stent restenosis, small vessels, bifurcations | Paclitaxel-coated; delivers drug without leaving a permanent implant |
| Scoring/Cutting balloon | Calcified, resistant, or ostial lesions | Atherotomes or scoring wire on surface fracture calcified plaque |
| Cryoplasty balloon | Peripheral use primarily | Delivers cold energy to induce apoptosis |
| Kissing balloon | Bifurcation lesions | Two balloons simultaneously inflate in main vessel + side branch |
CATEGORY 5: Coronary Stents
A. Bare Metal Stents (BMS)
- Metal scaffold only (cobalt-chromium or stainless steel)
- Introduced 1994; solved acute recoil and dissection after balloon angioplasty
- Major problem: ~20-30% restenosis (neointimal hyperplasia)
- Now largely replaced by DES except where prolonged DAPT is contraindicated
B. Drug-Eluting Stents (DES) - Current Standard of Care
- Metal platform + biodegradable or durable polymer + antiproliferative drug
- Restenosis reduced to <5%
- Drug examples: Everolimus, Zotarolimus, Sirolimus, Paclitaxel
- Common DES platforms:
| Device | Drug | Maker |
|---|---|---|
| XIENCE Sierra / Xpedition | Everolimus | Abbott |
| Resolute Onyx | Zotarolimus | Medtronic |
| SYNERGY | Everolimus (bioabsorbable polymer) | Boston Scientific |
| Orsiro | Sirolimus (bioabsorbable polymer) | Biotronik |
| Ultimaster Nagomi | Sirolimus | Terumo |
- Require dual antiplatelet therapy (DAPT) ideally for 12 months post-implant (aspirin + P2Y12 inhibitor) due to delayed endothelial healing
C. Bioresorbable Vascular Scaffolds (BVS)
- Fully dissolve over ~2-3 years, leaving no permanent metal
- Abbott ABSORB BVS (PLLA polymer + everolimus) - withdrawn from market after higher scaffold thrombosis rates
- Research continues with newer iteration designs (Magmaris - magnesium alloy)
D. Drug-Eluting Balloons (DEB) - Stentless Strategy
- Used for in-stent restenosis and small vessels (<2.5 mm) where stenting is avoided
- Paclitaxel coating transfers drug into vessel wall within 60 seconds of inflation
CATEGORY 6: Plaque Modification Devices
For heavily calcified or resistant lesions that balloons cannot adequately expand:
| Device | Mechanism | Example |
|---|---|---|
| Rotational atherectomy | High-speed diamond-coated burr (140,000-180,000 rpm) ablates calcified plaque into micro-particles (<10 microns) | Rotablator (Boston Scientific) |
| Orbital atherectomy | Eccentrically rotating crown sands calcium, wider treatment zone | Diamondback 360 (Cardiovascular Systems Inc.) |
| Intravascular lithotripsy (IVL) | Shockwave energy cracks both superficial and deep calcification, then balloon inflated | Shockwave S4 (Shockwave Medical) |
| Laser atherectomy (ELCA) | Excimer laser vaporizes plaque, useful in ISR and undilatable lesions | Spectranetics/Philips |
| Cutting/scoring balloon | Atherotome blades score calcified plaque | AngioSculpt, NSE Cutting Balloon |
CATEGORY 7: Imaging & Physiologic Assessment Hardware (Intracoronary)
Fractional Flow Reserve (FFR) / iFR
- Pressure wire placed beyond stenosis; measures ratio of distal to proximal pressure
- FFR <0.80 = hemodynamically significant; guides decision to stent vs. defer
- iFR (instantaneous wave-free ratio) - similar, no adenosine needed
- Devices: PressureWire X (Abbott), Verrata (Philips/Volcano), Coroventis CoroFlow
Intravascular Ultrasound (IVUS)
- 20-60 MHz ultrasound transducer on catheter tip
- Visualizes lumen dimensions, plaque burden, calcium location, stent apposition
- Used for stent sizing and optimization
- Devices: EAGLE Eye (Philips/Volcano), Revolution (Boston Scientific), AltaView (ACIST)
Optical Coherence Tomography (OCT)
- Near-infrared light; 10x higher resolution than IVUS
- Best for stent edge assessment, strut coverage, dissection identification
- Requires blood clearance (contrast flush)
- Devices: ILUMIEN OPTIS/ULUMIEN OPTA (Abbott), OPTIS Integrated (Abbott)
Near-Infrared Spectroscopy (NIRS) + IVUS
- Identifies lipid-rich plaques at risk of rupture
- TVC Insight (Infraredx / Nipro)
CATEGORY 8: Thrombectomy & Embolic Protection Devices
| Device | Type | Use |
|---|---|---|
| Aspiration catheters | Manual suction | STEMI with large thrombus (e.g., Export AP, Eliminate) |
| Distal embolic protection filters | Filter wire in distal vessel | Saphenous vein graft PCI (e.g., FilterWire EZ - Boston Scientific) |
| Proximal embolic protection | Occlusion balloon proximal to lesion | SVG PCI (e.g., Proxis - St. Jude/Abbott) |
| Mechanical thrombectomy | Aspiration + fragmentation | AngioJet (rheolytic), Penumbra CAT RX |
CATEGORY 9: Hemodynamic Support Devices
For high-risk PCI or cardiogenic shock:
| Device | Support Level | Mechanism |
|---|---|---|
| Intra-Aortic Balloon Pump (IABP) | ~0.5 L/min augmentation | Balloon in descending aorta; counterpulsation improves diastolic coronary filling |
| Impella CP / Impella 5.5 | 2.5-5.5 L/min | Axial flow pump across aortic valve (Abiomed/J&J) |
| TandemHeart | Up to 4 L/min | Transseptal left atrial to femoral artery bypass |
| VA-ECMO | Full cardiopulmonary bypass | Peripheral veno-arterial extracorporeal membrane oxygenation |
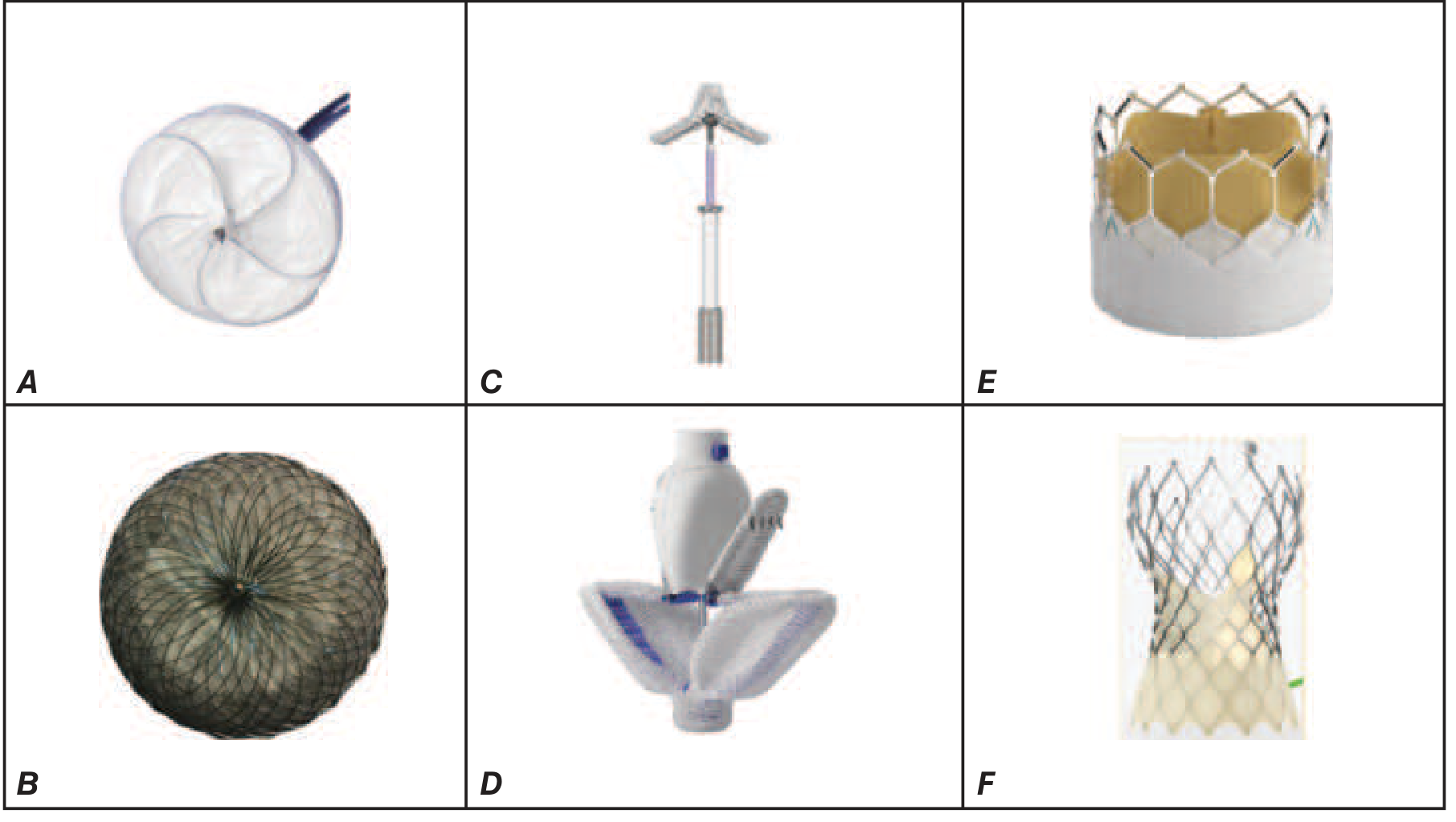
CATEGORY 10: Structural Heart Disease Hardware
A. Septal Closure Devices
- Atrial Septal Defect (ASD): Amplatzer Septal Occluder (Abbott), Gore ASD Occluder
- Patent Foramen Ovale (PFO): Amplatzer PFO Occluder, Gore Cardioform
- Ventricular Septal Defect (VSD): Amplatzer Muscular VSD Occluder
B. Transcatheter Aortic Valve Replacement (TAVR)
- Balloon-expandable: SAPIEN 3 Ultra RESILIA (Edwards Lifesciences) - FDA approved Sept 2022
- Self-expanding: Evolut FX (Medtronic) - nitinol frame, repositionable
- Delivered via transfemoral, transapical, or transaortic access
C. Transcatheter Mitral Valve Repair/Replacement (TMVR)
- MitraClip (Abbott): clips the leaflets together - edge-to-edge repair; for functional or degenerative MR
- PASCAL (Edwards): similar concept with larger paddles and clasps
- Tendyne (Abbott): fully implantable transcatheter mitral valve
D. Tricuspid Valve Devices
- TRILUMINATE Pivotal (Abbott TriClip): edge-to-edge TR repair
- CLASP TR (Edwards): PASCAL for tricuspid
- Transcatheter tricuspid replacement (TTVr) devices in trials
E. Left Atrial Appendage (LAA) Closure
- Prevents cardioembolic stroke in AF patients who cannot tolerate anticoagulation
- Watchman FLX (Boston Scientific): nitinol plug-in LAA
- Amulet (Abbott): dual-disc occluder
F. Valvuloplasty Balloons
- Mitral balloon valvuloplasty (Inoue balloon): for rheumatic mitral stenosis - preferred non-surgical option
- Aortic balloon valvuloplasty: palliative or bridge to TAVR
CATEGORY 11: Peripheral & Renal Interventional Hardware
The field has extended beyond coronary arteries to include:
- Carotid stenting - embolic protection mandatory (filter or flow reversal); nitinol self-expanding stents
- Renal artery stenting - for renovascular hypertension (balloon-expandable stents)
- Iliac/femoral/SFA intervention - self-expanding nitinol stents, drug-coated balloons, atherectomy
- Renal denervation - Symplicity Spyral catheter (Medtronic) for resistant hypertension - delivers RF energy to renal artery adventitia to ablate sympathetic nerves
CATEGORY 12: Ancillary Hardware
| Item | Role |
|---|---|
| Inflation device (indeflator) | Hand-held syringe with pressure gauge; inflates/deflates balloons to precise atmospheres |
| Y-connector | Hemostatic valve at catheter hub; allows wire + contrast injection |
| Torque device | Rotates guidewire tip to steer |
| Manifold | Connects contrast injector, pressure transducer, and saline flush |
| Introducer needle & dilator | Initial vessel puncture and tract dilation |
| Power injector | Automated contrast delivery for angiography |
Summary Table
| Category | Key Hardware |
|---|---|
| Vascular access | Sheaths, closure devices |
| Catheters | Guiding, diagnostic, microcatheter, aspiration |
| Guidewires | Workhorse, support, CTO, pressure wires |
| Balloons | Semi-compliant, NC, DCB, cutting/scoring |
| Stents | BMS, DES (everolimus/zotarolimus), BVS, DEB |
| Plaque modification | Rotablator, orbital atherectomy, IVL, laser |
| Imaging/physiology | FFR/iFR wire, IVUS, OCT, NIRS |
| Thrombectomy | Aspiration catheters, embolic filters, AngioJet |
| Hemodynamic support | IABP, Impella, TandemHeart, ECMO |
| Structural heart | TAVR, TMVR, LAA closure, septal occluders, valvuloplasty |
| Peripheral | Carotid/renal/peripheral stents, renal denervation |
| Ancillary | Inflators, Y-connectors, manifolds, torque devices |
Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 287 - Percutaneous Coronary Interventions and Other Interventional Procedures
This is a shared conversation. Sign in to Orris to start your own chat.