Approach to dvt
Reading File
Finding Sources
Finding Sources
Searching PubMed
"deep vein thrombosis" AND "diagnosis" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have everything needed for a complete, well-structured answer. Let me compile it:
Approach to Deep Vein Thrombosis (DVT)
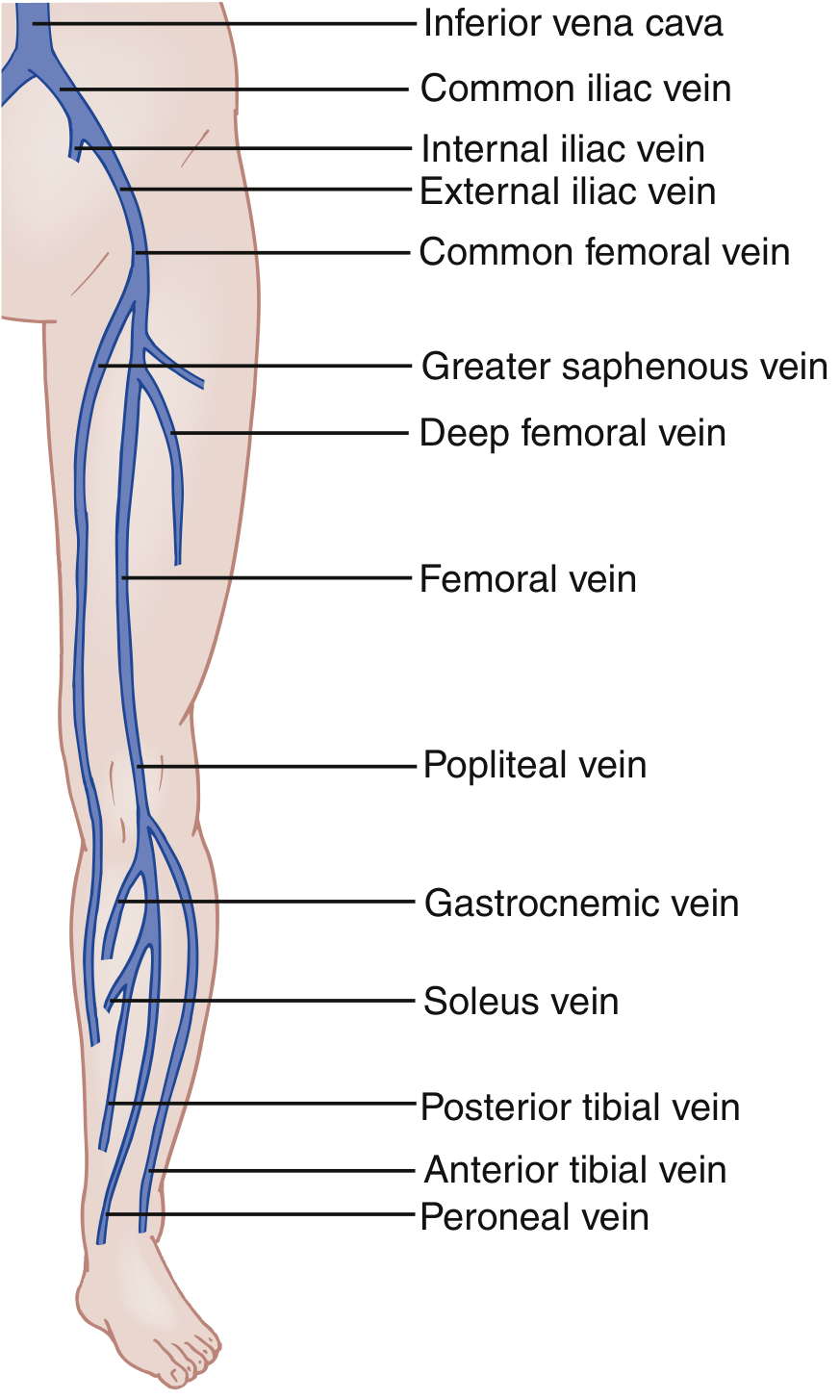
Anatomy
DVT can occur anywhere in the deep venous system. The proximal veins (popliteal, femoral, common femoral, iliac) carry the highest risk of pulmonary embolism. Distal (calf) veins include the posterior tibial, anterior tibial, and peroneal veins.
Pathophysiology - Virchow's Triad
Three factors predispose to thrombosis:
- Venous stasis - immobility, reduced calf pump, obstruction (e.g., gravid uterus compressing iliac veins)
- Endothelial injury - venous trauma, surgery, intravenous catheters
- Hypercoagulability - deficiencies of antithrombin III, protein C, protein S; malignancy; antiphospholipid syndrome; OCP use; pregnancy
Risk Factors
| Category | Examples |
|---|---|
| Provoked | Surgery, fracture, immobility, hospitalization, pregnancy/postpartum |
| Medical illness | Active cancer, heart failure, inflammatory bowel disease |
| Thrombophilia | Factor V Leiden, prothrombin mutation, antiphospholipid antibody |
| Patient factors | Prior VTE, age, obesity, OCP/HRT |
| Upper extremity | Indwelling catheters (>90% of cases), Paget-Schroetter syndrome in young athletes |
Note: May-Thurner syndrome (left iliac vein compressed by right iliac artery) explains why left leg DVT is slightly more common.
Clinical Features
Hallmarks are unilateral limb pain and swelling, though these can be subtle and nonspecific. Signs include:
- Pitting edema
- Erythema and warmth
- Tenderness along the deep venous distribution
- Dilation of superficial collateral veins
- Rarely, a palpable venous cord
Homans' sign (calf pain on dorsiflexion) is neither sensitive nor specific and should not be relied upon.
Fever suggests an alternative diagnosis such as cellulitis. Bilateral DVT occurs in fewer than 10% of cases.
Differential Diagnosis
-
Venous insufficiency / chronic venous congestion
-
Cellulitis (concurrent DVT is present in only ~3% of proven cellulitis)
-
Ruptured Baker cyst
-
Gastrocnemius muscle tear or Achilles tendon injury
-
Calf hematoma
-
Asymmetric edema from heart failure or liver disease
-
Arterial claudication
-
Rosen's Emergency Medicine, p. 1196-1197
Step 1: Pre-test Probability - Wells DVT Score
| Clinical Feature | Points |
|---|---|
| Active cancer (ongoing treatment, within 6 months, or palliative) | +1 |
| Paralysis, paresis, or recent plaster immobilization of lower extremity | +1 |
| Recently bedridden ≥3 days or major surgery within 12 weeks | +1 |
| Localized tenderness along the deep venous system | +1 |
| Entire leg swollen | +1 |
| Calf swelling ≥3 cm vs asymptomatic side | +1 |
| Pitting edema confined to symptomatic leg | +1 |
| Collateral (non-varicose) superficial veins | +1 |
| Alternative diagnosis at least as likely | -2 |
Interpretation:
- Score < 2: Low pre-test probability (PTP)
- Score ≥ 2: High PTP
In pregnant women, the LEFt score is used instead (1 point each for Left leg, Edema, and First trimester). Score 0-1 = low PTP.
Step 2: Diagnostic Workup
D-dimer
- A highly sensitive but non-specific fibrin degradation product assay
- Standard cutoff: >500 ng/mL (confirm local lab threshold)
- Age-adjusted cutoff for patients >50 years: age × 10 ng/mL (e.g., 80-year-old = 800 ng/mL cutoff) - maintains ~95% sensitivity while reducing unnecessary US
- False positives with: pregnancy, malignancy, recent surgery, renal failure, SLE, sickle cell disease, advanced age, Black race
- Warfarin use may cause false-negative D-dimer results
Venous Compression Ultrasound (Gold Standard)
- Three-point compression US (proximal): common femoral, femoral, and popliteal veins
- Whole-leg US: adds tibial, peroneal, and gastrocnemius veins; detects distal DVT but increases false-positive rate
- Diagnostic criterion: non-compressibility of the vein under probe pressure, absence of flow, no respiratory augmentation
Other Imaging
- MRI venography / CT venography: reserved for suspected pelvic vein DVT (e.g., gynecological malignancy with bilateral leg swelling); venous US is still first-line even when pelvic DVT is suspected
- Conventional contrast venography: historical gold standard, now rarely used
Step 3: Diagnostic Algorithm
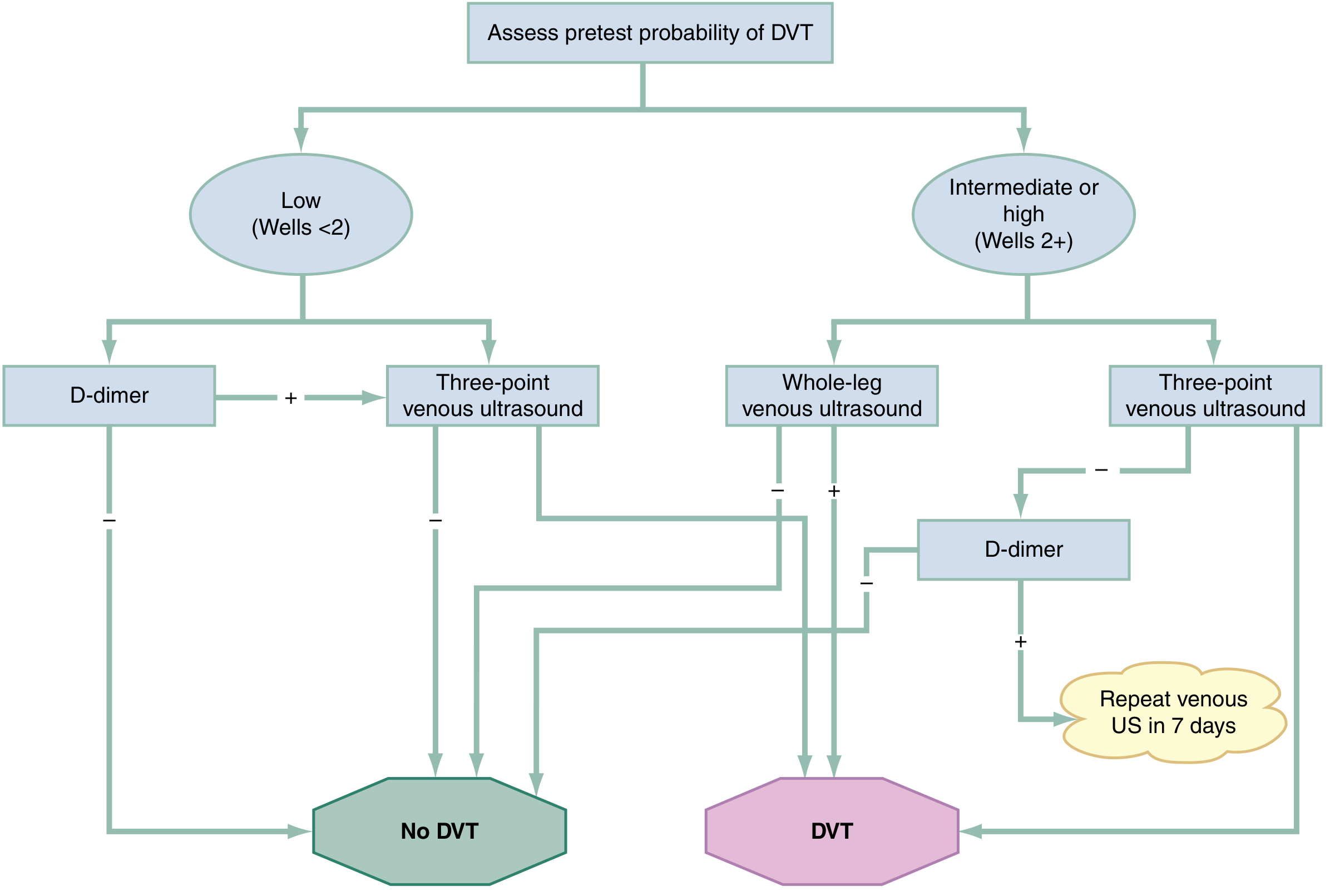
In practice:
-
Low PTP (Wells <2): Send D-dimer first. If negative - DVT excluded. If positive - perform 3-point or whole-leg venous US.
-
High PTP (Wells ≥2): Go straight to venous US (whole-leg preferred). If US negative + D-dimer negative - DVT excluded. If US negative but D-dimer positive - repeat venous US in 7 days to detect distal clot propagation.
-
High PTP + positive US: Diagnose and treat DVT.
-
Rosen's Emergency Medicine, p. 1199-1200
Step 4: Management
Anticoagulation (First-line)
Start anticoagulation immediately at time of confirmed diagnosis (or when high PTP and imaging is delayed).
| Agent | Initial Dose | Notes |
|---|---|---|
| Rivaroxaban (preferred DOAC) | 15 mg BD × 21 days, then 20 mg OD | With food; avoid if CrCl <30 |
| Apixaban (preferred DOAC) | 10 mg BD × 7 days, then 5 mg BD | With or without food; avoid if CrCl <30 |
| Enoxaparin (LMWH) | 1 mg/kg SC q12h or 1.5 mg/kg q24h | Avoid if CrCl <30 |
| Dalteparin | 200 unit/kg daily or 100 unit/kg q12h SC | Avoid if CrCl <30 |
| Fondaparinux | 5-10 mg SC once daily | For HIT; avoid if CrCl <30 |
| Unfractionated heparin (UFH) | 70-80 U/kg bolus, then 17-18 U/kg/h IV | Use in severe renal impairment, pregnancy, high-bleeding risk (reversible) |
| Warfarin | Overlap with parenteral agent; titrate to INR 2-3 | Requires monitoring; inferior to DOACs |
DOACs are first choice - equally effective as warfarin, fewer bleeding events (especially intracranial), no monitoring required.
DOAC contraindications/cautions:
- Pregnancy (use LMWH)
- Severe renal failure (use UFH)
- Liver failure
- Antiphospholipid antibody syndrome (use warfarin)
- High-risk PE
Duration of Anticoagulation
| Scenario | Duration |
|---|---|
| Provoked DVT (surgery, trauma, transient risk) | 3 months |
| Unprovoked DVT | At least 3 months; consider extended (reassess bleeding vs thrombosis risk) |
| Active cancer (cancer-associated VTE) | LMWH or DOAC; continue as long as cancer active |
| Recurrent unprovoked VTE | Long-term anticoagulation |
Special Situations
Calf (distal) DVT only:
- Anticoagulation may be withheld if no symptoms of propagation and low risk - but requires close surveillance with serial US
- If patient is symptomatic or has risk factors for propagation, treat
IVC Filter:
- Only if anticoagulation is absolutely contraindicated
- Use a retrievable filter; remove when anticoagulation becomes safe
Catheter-directed thrombolysis (CDT) / endovascular therapy:
- Considered in extensive iliofemoral DVT to reduce post-thrombotic syndrome (PTS) risk
- Does not improve mortality but may reduce long-term morbidity in selected cases
- Carries higher bleeding risk - not routine
Compression stockings:
- No longer routinely recommended to prevent PTS (trials showed no benefit)
- May offer symptom relief; encourage early ambulation post-anticoagulation
Step 5: Assess Bleeding Risk Before Anticoagulation
Absolute contraindications:
- Active bleeding into a critical organ or uncontrolled site
- Severe bleeding diathesis
- Recent/planned high-bleeding-risk surgery
- Recent major trauma
- Recent intracranial, spinal, or ocular hemorrhage
Relative contraindications:
- History of major GI bleeding
- Intracranial or spinal tumors
- Large AAA with severe hypertension
- Stable aortic dissection
Use the VTE-BLEED score to stratify: score <2 = 0.5% risk of major bleeding; score ≥2 = 2.0%.
Reversal Agents
| Anticoagulant | Reversal Agent |
|---|---|
| Heparin (UFH) | Protamine sulfate |
| Warfarin | FFP, 4-factor PCC, Vitamin K |
| Dabigatran | Idarucizumab |
| Rivaroxaban, Apixaban | Andexanet alfa |
Complications
- Pulmonary embolism - the most feared complication; small emboli cause pleuritic chest pain, large emboli cause hemodynamic collapse
- Post-thrombotic syndrome (PTS) - chronic pain, swelling, skin changes, and ulceration; affects up to 50% after proximal DVT. A 2026 systematic review (PMID: 41655785) estimated PTS incidence in Europe at significant levels, reinforcing the need for prompt treatment
- Phlegmasia cerulea dolens - massive venous occlusion causing limb ischemia; requires urgent intervention
Upper Extremity DVT - Special Note
-
90% occur with an indwelling catheter, pacemaker wire, or similar device
-
Without a device: think Paget-Schroetter syndrome (effort-induced thoracic outlet syndrome in young dominant-arm athletes)
-
Approach: same principles - US, anticoagulation, consider catheter removal
-
Rosen's Emergency Medicine, pp. 1196-1202; Bailey & Love's Surgery, 28th Ed., pp. 344-345; Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.