CARCINOMA BREAST (PA31.2) Epidemiology, risk factors, molecular subtypes Gross and microscopic: IDC, ILC, special types Prognostic factors: ER/PR/HER2, lymph nodes Staging (TNM) From ramdas
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the content and images needed. Let me compile the comprehensive answer for PA31.2.
Carcinoma Breast (PA31.2)
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease
1. EPIDEMIOLOGY
Breast cancer is the most common malignancy globally and the leading cause of cancer death in females worldwide. Key facts:
- In 2020, it surpassed lung cancer as the most common cancer overall - ~2.3 million new cases (nearly 12% of all new cancer diagnoses worldwide)
- Lifetime risk: 1 in 8 females (living to age 90) in the United States
- Incidence is highest in North America, Northern/Western Europe, and Australia/New Zealand
- Rare below age 25; incidence rises steeply after age 30
- Incidence and mortality are increasing rapidly in low-resource countries (due to delayed childbearing, fewer pregnancies, reduced breastfeeding)
- Ethnicity: Highest incidence in females of European descent (avg. diagnosis age 63); females of African descent diagnosed earlier (avg. 59 years) with higher proportion of aggressive subtypes and higher mortality
- Overall risk of death once diagnosed: ~20% (declining ~1-2%/year due to earlier diagnosis and better adjuvant therapy)
2. RISK FACTORS
| Risk Factor | Relative Risk |
|---|---|
| Female sex | >4.0 |
| Increasing age | >4.0 |
| Germline mutations (high penetrance: BRCA1/2) | >4.0 |
| Strong family history (>1 first-degree relative, young age, multiple cancers) | >4.0 |
| Personal history of breast cancer | >4.0 |
| High breast density | >4.0 |
| Germline mutations (moderate penetrance: ATM, PALB2, CHEK2) | 2.1-4.0 |
| High-dose chest radiation at young age (<18 years) | 2.1-4.0 |
| Family history (1 first-degree relative) | 2.1-4.0 |
| Early menarche (<12 years) | 1.1-2.0 |
| Late menopause (>55 years) | 1.1-2.0 |
| Late first pregnancy (>35 years) | 1.1-2.0 |
| Nulliparity | 1.1-2.0 |
| Absence of breastfeeding | 1.1-2.0 |
| Exogenous hormone therapy | 1.1-2.0 |
| Postmenopausal obesity | 1.1-2.0 |
| Physical inactivity | 1.1-2.0 |
| High alcohol consumption | 1.1-2.0 |
Key points on risk:
- ~20% of breast cancers are attributable to modifiable factors (obesity, alcohol, inactivity)
- Estrogen exposure (endogenous and exogenous) is a major driver - estrogen promotes proliferation of luminal epithelial cells, increasing the chance of acquired mutations
- BRCA1 (chromosome 17q): lifetime risk up to 80%; associated with TNBC/basal-like subtype
- BRCA2 (chromosome 13q): lifetime risk up to 85%; associated with luminal/ER+ subtype; also increases male breast cancer risk
3. MOLECULAR SUBTYPES
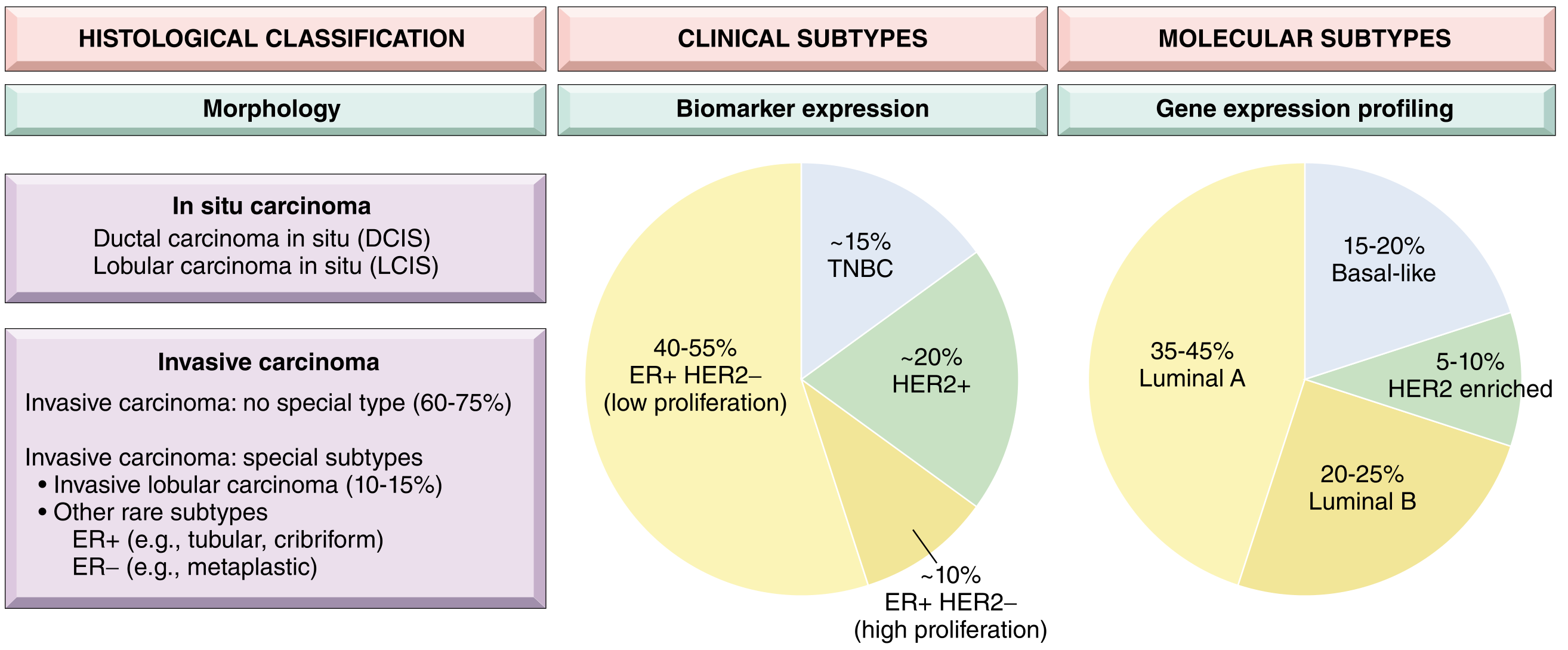
Fig. 23.15 - Breast cancer classification framework (Robbins PBD)
Three complementary classification systems exist:
A. Clinical Subtypes (Biomarker-based - routine practice)
| Clinical Subtype | Biomarker Profile | Frequency | Treatment |
|---|---|---|---|
| Luminal | ER+ / HER2- | ~65% | Endocrine therapy (tamoxifen/aromatase inhibitors) |
| HER2 | HER2 overexpressed (ER+ or ER-) | ~20% | Anti-HER2 (trastuzumab) |
| TNBC (Triple Negative) | ER-/PR-/HER2- | ~15% | Chemotherapy; immunotherapy |
B. Intrinsic Molecular Subtypes (Gene Expression Profiling)
| Molecular Subtype | % | Key Features | Prognosis |
|---|---|---|---|
| Luminal A | 35-45% | ER+/PR+/HER2-, low Ki67, low grade | Best; late recurrences continue |
| Luminal B | 20-25% | ER+, higher Ki67 (high proliferation), may be HER2+ | Intermediate |
| HER2 enriched | 5-10% | HER2 amplified, ER- | Poor without targeted therapy |
| Basal-like | 15-20% | ER-/PR-/HER2-, CK5/6+, EGFR+; overlaps TNBC | Poor; early recurrence |
| Normal-like | ~5% | Resembles normal breast tissue | Good |
| Claudin-low | ~5% | Low claudin expression, mesenchymal features | Poor |
Key clinical insight: Luminal cancers have the lowest early recurrence rate but continue to recur late (>10 years). TNBC recurrences peak early (within 3 years) and almost all occur within 8 years. HER2+ shows a bimodal pattern.
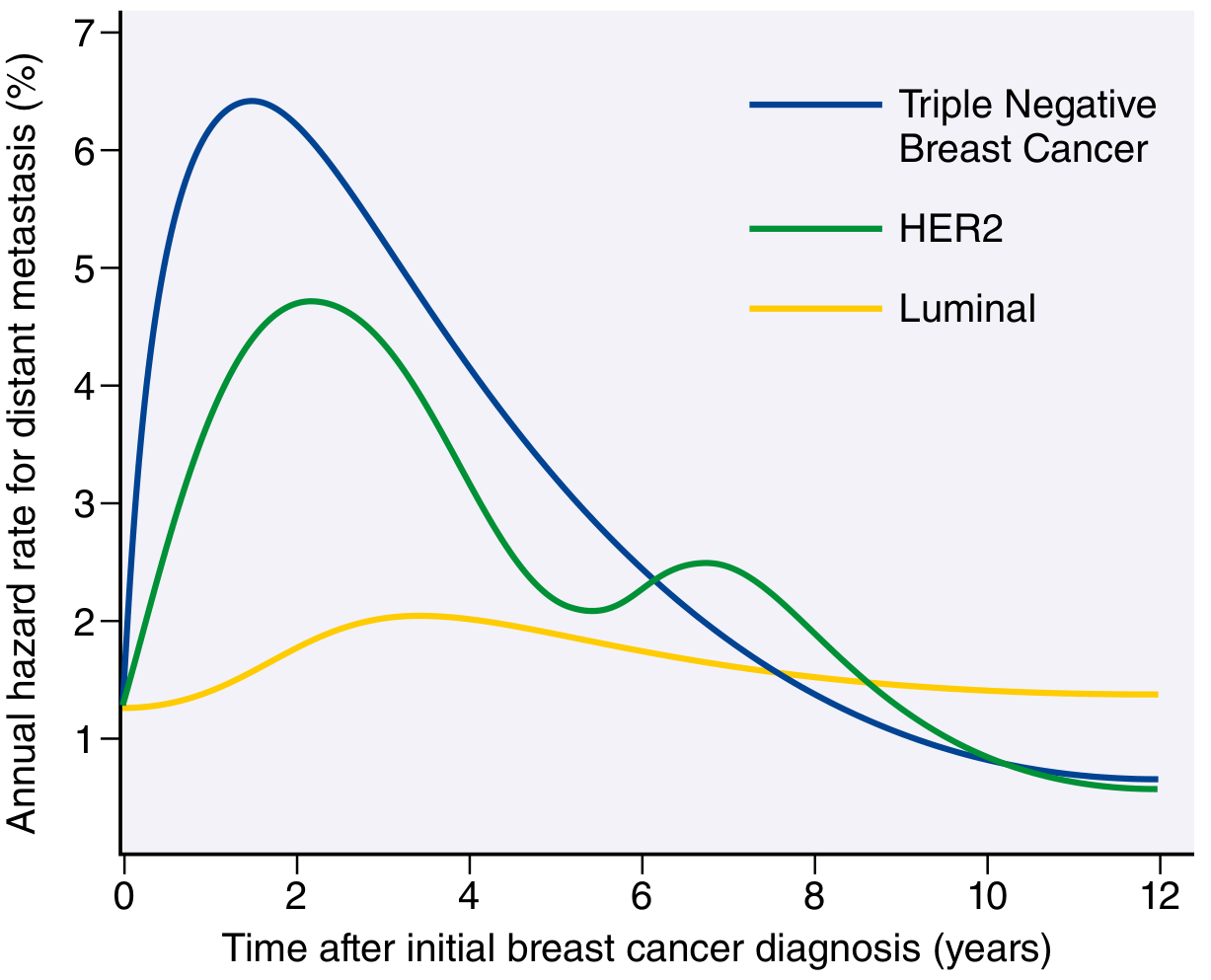
Fig. 23.23 - Recurrence hazard rates by molecular subtype (Robbins PBD)
4. GROSS AND MICROSCOPIC PATHOLOGY
A. Invasive Ductal Carcinoma (IDC) / Invasive Carcinoma of No Special Type (NST)
- Most common invasive breast malignancy - ~75% of cases
- Heterogeneous group; lacks the defining features of special subtypes
Gross:
- Hard, irregular, stellate/spiculated mass with irregular margins
- Associated desmoplastic stromal reaction (scirrhous carcinoma)
- On cutting: grating/chalky-white sound due to desmoplastic stroma and calcification foci
- Mammography: radiodense, spiculated mass ± calcifications
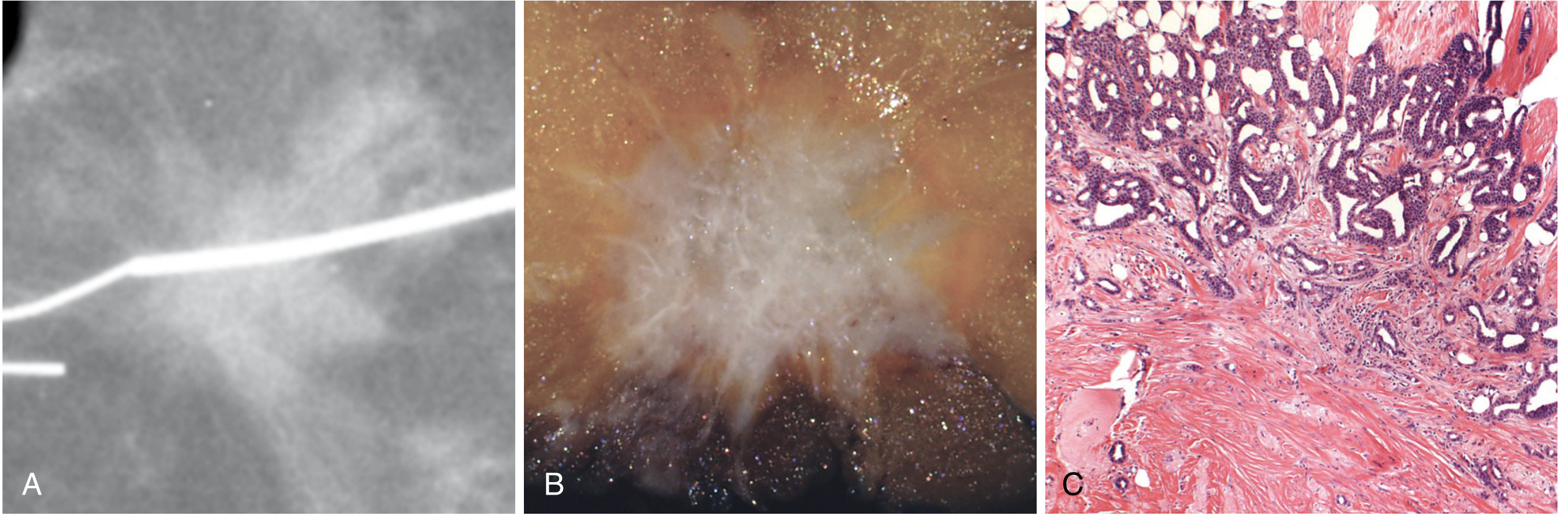
Fig. 23.20 - IDC (NST): (A) mammographic stellate density, (B) gross spiculated grey-white mass, (C) exuberant desmoplastic stromal response on microscopy
Microscopic (Nottingham Histologic Grading - 3 parameters):
| Grade | Tubule Formation | Nuclear Pleomorphism | Mitotic Rate | Score |
|---|---|---|---|---|
| Grade 1 (Well diff.) | >75% tubules | Small, uniform nuclei | Low | 3-5 |
| Grade 2 (Mod. diff.) | 10-75% tubules | Moderate pleomorphism | Moderate | 6-7 |
| Grade 3 (Poorly diff.) | <10% tubules | Marked pleomorphism, irregular nuclei | High | 8-9 |
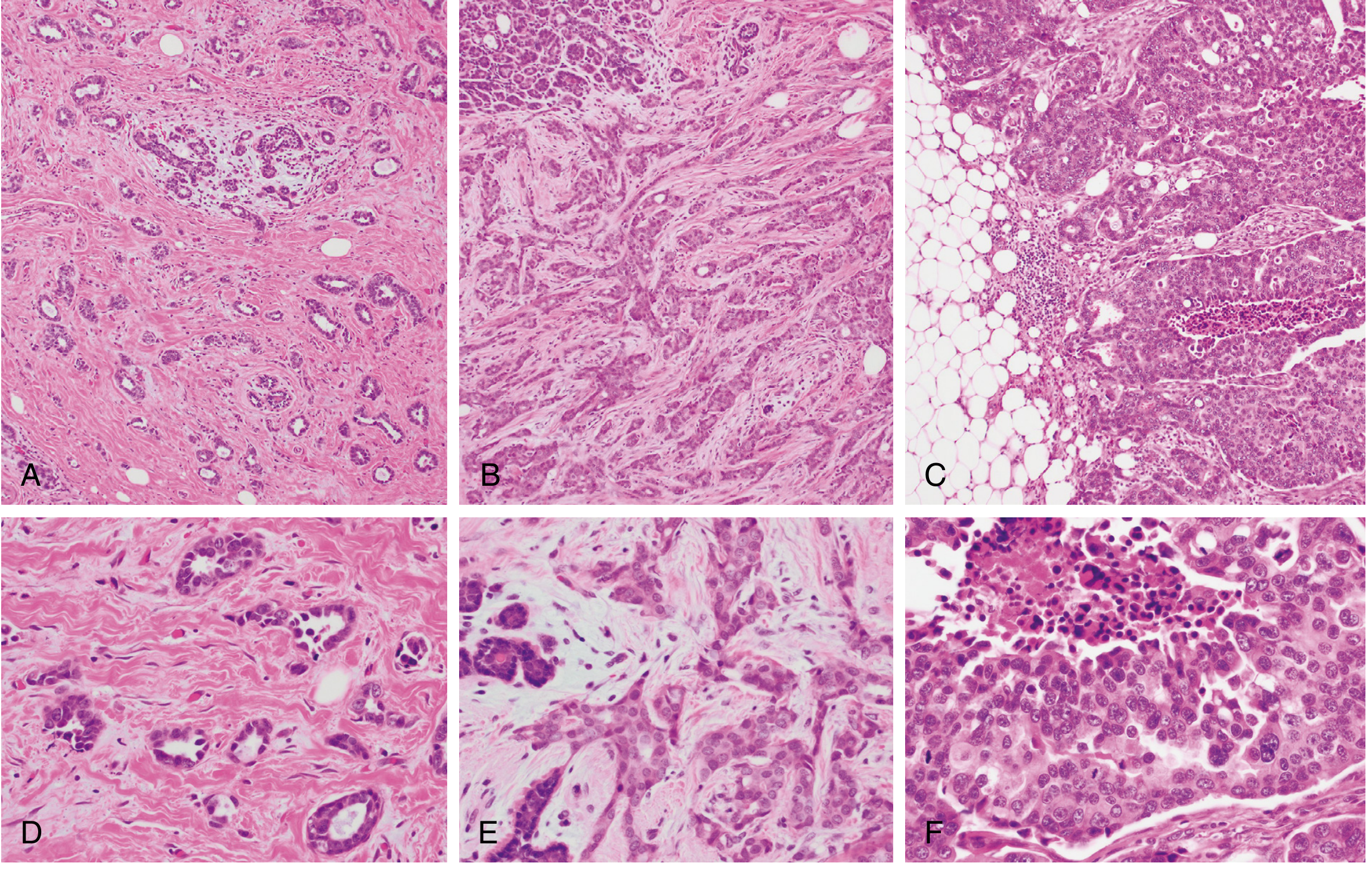
Fig. 23.21 - Histologic grading: A,D = Grade 1 (tubular pattern, small nuclei); B,E = Grade 2 (solid nests, moderate pleomorphism); C,F = Grade 3 (ragged sheets, large nuclei, necrosis)
"Medullary pattern" IDC: High-grade tumor with prominent tumor-infiltrating lymphocytes (TILs) - previously called medullary carcinoma; now classified as IDC with medullary pattern.
B. Invasive Lobular Carcinoma (ILC)
- Second most common invasive breast carcinoma - up to 15% of cases
- Defined by loss of E-cadherin (CDH1 gene mutation/loss - hallmark)
- Associated with germline CDH1 mutations (also signet ring carcinoma of stomach)
Gross:
- Often insidious - produces minimal desmoplasia
- Difficult to detect on imaging; often imperceptible on mammography
- No discrete mass; diffuse infiltration of breast tissue
Microscopic:
- Classic pattern: dyscohesive infiltrating tumor cells in single-file "Indian file" cords
- Cells are small, round, with intracytoplasmic mucin vacuoles - may look like signet ring cells
- Cells often target/wrap around pre-existing normal ducts (targetoid pattern)
- E-cadherin immunostain: negative (vs. positive in IDC)
Spread pattern: Characteristic metastatic sites - peritoneum, retroperitoneum, leptomeninges, GI tract, ovaries, uterus.
C. Special Histologic Subtypes
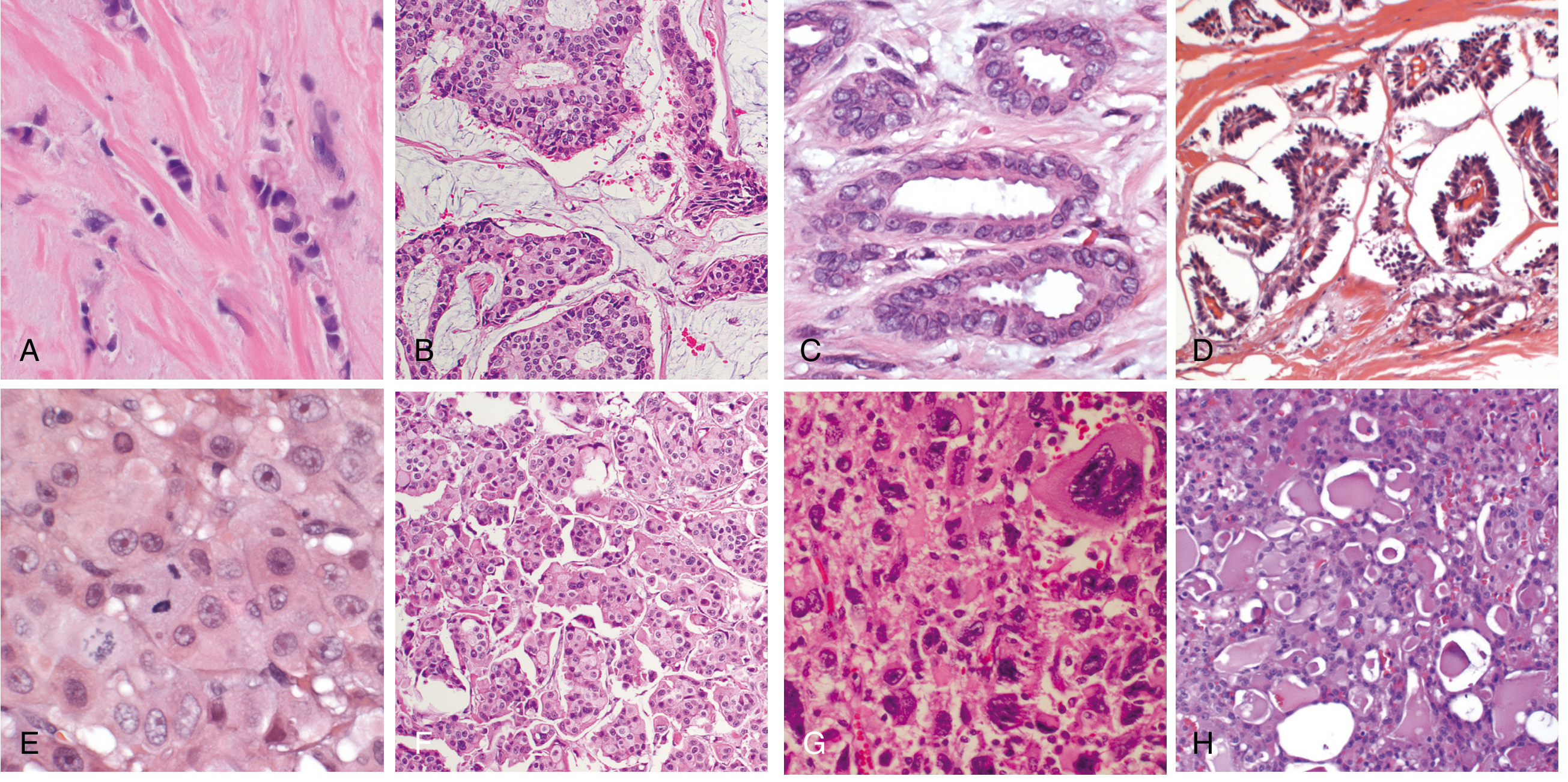
Fig. 23.22 - Special types: (A) ILC - single-file cords; (B) Mucinous - tumor cells in mucin lakes; (C) Tubular - well-formed tubules; (D) Papillary - true papillary fronds; (E) Apocrine - eosinophilic granular cytoplasm; (F) Micropapillary - hollow balls floating in fluid; (G) Metaplastic - squamous/mesenchymal differentiation; (H) Secretory/salivary-type
| Subtype | Molecular Class | Key Features | Prognosis |
|---|---|---|---|
| Mucinous (colloid) | Luminal (ER+) | Tumor cells in large lakes of extracellular mucin; soft, gelatinous, pushing borders | Favorable |
| Tubular | Luminal (ER+) | >90% well-formed tubules; single layer of cells; may mimic sclerosing adenosis | Excellent |
| Cribriform | Luminal (ER+) | Invasive nests with cribriform (sieve-like) morphology | Favorable |
| Papillary | Luminal (ER+) | True papillary fronds lined by tumor cells | Favorable |
| Apocrine | HER2 enriched | Enlarged nuclei + prominent nucleoli + eosinophilic granular cytoplasm | Variable |
| Micropapillary | HER2 enriched | Hollow balls of cells floating in fluid-filled spaces (NOT true papillae); high LVI | Poor (high LVI, lymph node mets) |
| Metaplastic | TNBC | Squamous or mesenchymal (spindle, chondroid, osseous) differentiation; myoepithelial gene profile | Generally poor |
| Adenoid cystic / Secretory / Mucoepidermoid | TNBC | "Salivary gland-like" carcinomas; rare, indolent | Relatively favorable |
Inflammatory Breast Carcinoma (not a histologic type but a clinical syndrome):
- Extensive plugging of dermal lymphovascular spaces by carcinoma cells
- Presents as diffuse breast erythema, swelling, skin thickening
- Peau d'orange: skin tethered by Cooper ligaments → orange-peel appearance
- No discrete palpable mass; usually high-grade, diffusely infiltrative
- Misnomer - NO actual inflammation present
- Very poor prognosis
5. PROGNOSTIC FACTORS
A. ER / PR (Estrogen Receptor / Progesterone Receptor)
- Assessed by immunohistochemistry (IHC) - nuclear staining
- ER+ tumors (Luminal):
- Better overall prognosis (lower early recurrence rates)
- Respond to endocrine therapy (tamoxifen in premenopausal; aromatase inhibitors in postmenopausal)
- But continue to recur late (10-20 years post-diagnosis)
- ER+/PR+ = best hormone response; ER+/PR- = less responsive
- ER-/PR- (TNBC):
- Aggressive; early recurrences; no endocrine therapy benefit
- Peak recurrence at ~18 months; most recurrences within 8 years
B. HER2 (Human Epidermal Growth Factor Receptor 2)
- Encoded by ERBB2 gene (chromosome 17q12)
- Assessed by IHC (score 0, 1+, 2+, 3+) ± FISH (for IHC 2+ equivocal cases)
- HER2 overexpression (IHC 3+ or FISH amplified) = ~20% of cancers
- HER2+ without targeted therapy: Poor prognosis
- HER2+ with trastuzumab (anti-HER2): Markedly improved outcomes
- Bimodal recurrence pattern (early and late peaks)
C. Lymph Node Status
- Most important anatomic/staging prognostic factor (for localized disease)
- Number of involved nodes correlates directly with prognosis:
| Lymph Node Status | 10-year DFS (approx.) |
|---|---|
| Node-negative | ~70-80% |
| 1-3 positive nodes | ~50-60% |
| 4-9 positive nodes | ~25-40% |
| ≥10 positive nodes | ~10-20% |
- Axillary lymph nodes (Level I, II, III) are the primary drainage; sentinel lymph node biopsy (SLNB) is the standard first step
D. Other Key Prognostic Factors
| Factor | Significance |
|---|---|
| Distant metastases | Most important overall; cure unlikely once present |
| Tumor size | Larger size = worse prognosis; strongly correlates with LN status |
| Histologic grade | Grade 3 > Grade 2 > Grade 1 (poorer outcome) |
| Histologic type | Tubular, mucinous, cribriform = better; metaplastic, micropapillary = worse |
| Proliferation (Ki67) | High Ki67 = high proliferation = poor prognosis (esp. in luminal B) |
| Lymphovascular invasion (LVI) | Positive LVI = higher risk of LN and distant metastases |
| Tumor-infiltrating lymphocytes (TILs) | High TILs = better response to therapy, better prognosis (esp. in TNBC, HER2+) |
| Gene expression signatures | Oncotype DX (21-gene), MammaPrint (70-gene): guide chemotherapy decisions in ER+/HER2- |
6. TNM STAGING (AJCC)
Primary Tumor (T)
| Stage | Description |
|---|---|
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis | Carcinoma in situ (DCIS; or Paget disease with no invasive tumor) |
| T1 | Tumor ≤20 mm in greatest dimension |
| - T1mi | Microinvasion ≤1 mm |
| - T1a | >1 mm to ≤5 mm |
| - T1b | >5 mm to ≤10 mm |
| - T1c | >10 mm to ≤20 mm |
| T2 | Tumor >20 mm to ≤50 mm |
| T3 | Tumor >50 mm |
| T4 | Any size with direct extension to: chest wall (T4a), skin (T4b), both (T4c), or inflammatory carcinoma (T4d) |
Regional Lymph Nodes (N)
| Stage | Description |
|---|---|
| N0 | No regional lymph node metastasis |
| N1 | Metastasis in movable ipsilateral Level I/II axillary lymph node(s) |
| N2 | Metastasis in ipsilateral Level I/II axillary nodes fixed/matted (N2a); or clinically detected internal mammary nodes without axillary involvement (N2b) |
| N3 | Metastasis in ipsilateral infraclavicular (Level III axillary) nodes (N3a); or clinically detected internal mammary + axillary (N3b); or ipsilateral supraclavicular nodes (N3c) |
Distant Metastases (M)
| Stage | Description |
|---|---|
| M0 | No distant metastasis |
| cM0(i+) | No distant metastasis but circulating tumor cells detected |
| M1 | Distant metastasis present (bone, lung, liver, brain most common) |
Anatomic Stage Groups
| Stage | T | N | M | 5-year OS (approx.) |
|---|---|---|---|---|
| Stage 0 | Tis | N0 | M0 | ~99% |
| Stage IA | T1 | N0 | M0 | ~99% |
| Stage IB | T0-T1 | N1mi | M0 | ~99% |
| Stage IIA | T0-T1/N1 or T2/N0 | M0 | ~93% | |
| Stage IIB | T2/N1 or T3/N0 | M0 | ~75% | |
| Stage IIIA | T0-T3/N2 or T3/N1 | M0 | ~66% | |
| Stage IIIB | T4/N0-N2 | M0 | ~40% | |
| Stage IIIC | Any T/N3 | M0 | ~40% | |
| Stage IV | Any T | Any N | M1 | ~28% |
Note: The AJCC 8th edition also incorporates biomarker-based prognostic stage (using ER, PR, HER2, grade, and Oncotype DX score) alongside anatomic stage, which can upgrade or downgrade the anatomic stage group.
Quick Summary Table
| Feature | IDC (NST) | ILC | TNBC |
|---|---|---|---|
| Frequency | 75% | 10-15% | 15% |
| E-cadherin | + | - (lost) | + |
| Gross | Stellate/hard, spiculated | No discrete mass, insidious | Circumscribed (sometimes) |
| Microscopy | Glands/nests + desmoplasia | Indian file cords, signet ring cells | Sheets, TILs, necrosis |
| ER/PR | Variable | Usually ER+ | Negative |
| HER2 | Variable | Usually negative | Negative |
| Special spread | Axillary LNs | Peritoneum, GI, meninges | Lung, brain |
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease (9780443264528)
Make into flowchart image based for mbbs university exam
Generating Image
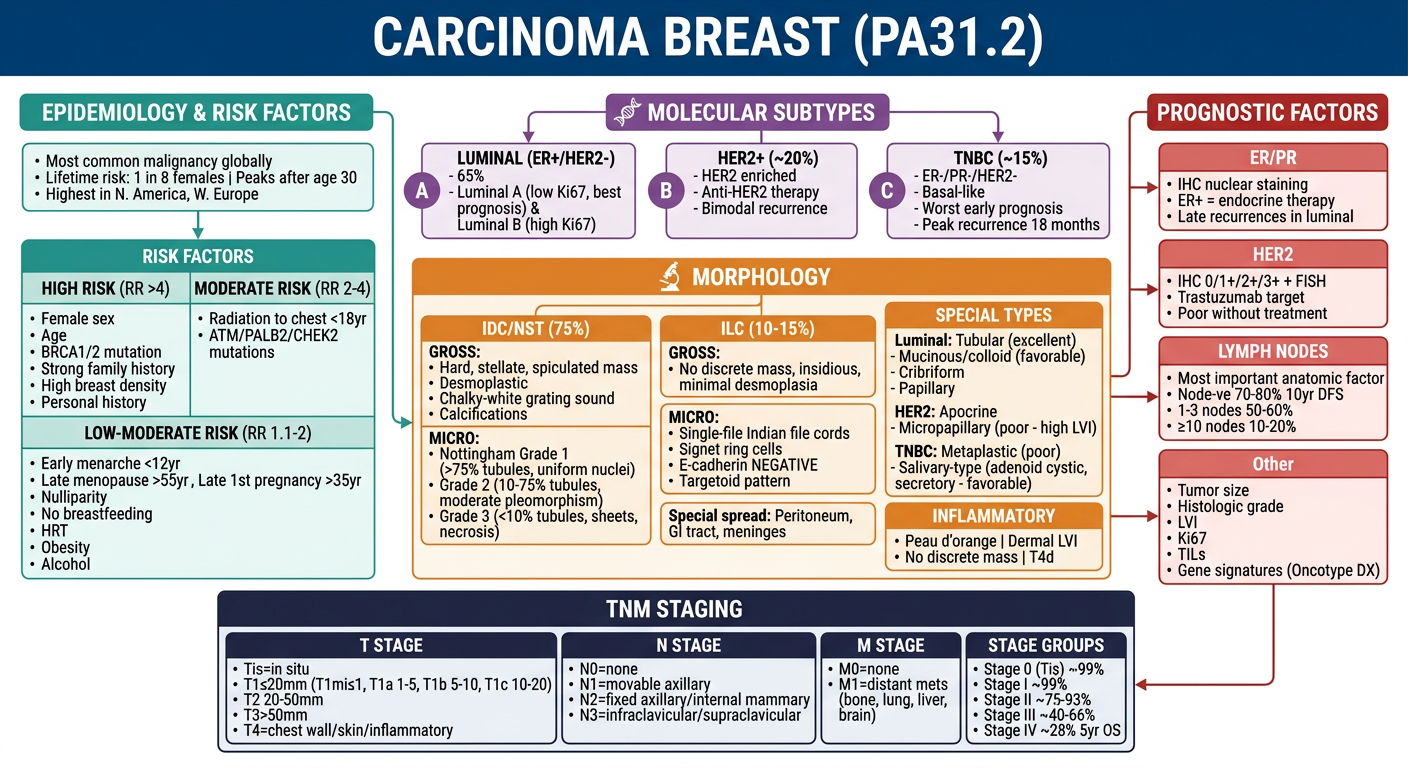
Here's your complete PA31.2 exam flowchart covering all four topics in one visual:
- Top-left - Epidemiology + Risk factors with relative risk groupings
- Top-center - Three molecular subtypes (Luminal / HER2 / TNBC) with frequencies
- Center - IDC morphology (gross + Nottingham grading), ILC hallmarks (Indian file, E-cadherin loss), and all special subtypes with their prognosis
- Right - Prognostic factors (ER/PR, HER2, lymph nodes, Ki67, TILs)
- Bottom - Full TNM staging with 5-year OS for each stage group
The color-coded sections make it easy to revise quickly before university exams. Each box is self-contained for short-answer or essay-type questions.
This is a shared conversation. Sign in to Orris to start your own chat.