Factors affecting myocardial oxygen supply demand and factors affecting myocardial oxygen supply demand during anesthesia.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
I have exhausted my database queries. I now have sufficient information from Miller's Anesthesia, Harrison's, and Goodman & Gilman's to construct a thorough, well-structured answer. Let me compile the complete response.
Myocardial Oxygen Supply-Demand Balance
The myocardium extracts oxygen near-maximally at rest (~70-75% extraction), leaving almost no reserve. Unlike skeletal muscle, the heart cannot significantly increase extraction during stress - it must increase delivery. Any mismatch between supply and demand results in ischemia.
Part 1: Determinants of Myocardial Oxygen Demand (MVO₂)
The three principal determinants of MVO₂ are heart rate, myocardial contractility, and myocardial wall tension (stress).
1. Heart Rate
- The most important determinant. Increased heart rate increases oxygen consumption per unit time AND shortens diastole (the phase during which 70-80% of coronary blood flow occurs), simultaneously increasing demand and reducing supply.
- The relationship between heart rate and diastolic duration is nonlinear - small increases in rate disproportionately shorten diastole.
- This dual effect makes tachycardia the most dangerous hemodynamic perturbation for myocardial oxygen balance.
2. Myocardial Contractility (Inotropy)
- Greater contractile force requires more ATP and therefore more oxygen.
- Increased catecholamine stimulation (pain, anxiety, light anesthesia, laryngoscopy) raises contractility and MVO₂.
3. Myocardial Wall Tension (Wall Stress / Afterload & Preload)
Governed by the Law of Laplace: Wall tension = (Pressure × Radius) / (2 × Wall thickness)
Two components increase wall tension:
| Component | Hemodynamic correlate |
|---|---|
| Preload (ventricular volume/filling pressure) | Increases radius → increases wall tension |
| Afterload (systolic pressure against which the heart ejects) | Directly increases wall tension |
- Hypertension dramatically increases afterload and MVO₂.
- Ventricular dilatation (e.g., heart failure) increases radius and thus wall tension even at normal pressures.
- Myocardial hypertrophy reduces wall thickness → further increase in wall tension per unit.
Minor Determinants
- Basal metabolic rate - constant, obligatory oxygen consumption for cell integrity (~20-25% of total MVO₂)
- Activation energy - electrical depolarization accounts for a small fraction
- External work - primarily stroke volume × pressure (pressure-volume area)
Part 2: Determinants of Myocardial Oxygen Supply
Supply = Coronary blood flow × Arterial oxygen content
A. Coronary Blood Flow
1. Coronary Perfusion Pressure (CPP)
- Left ventricle (LV): CPP = Aortic diastolic pressure - Left ventricular end-diastolic pressure (LVEDP)
- Elevated LVEDP (e.g., heart failure, volume overload) critically impairs subendocardial perfusion
- Hypotension directly reduces CPP
- Right ventricle (RV): Perfused during both systole and diastole (lower intramural pressures)
2. Duration of Diastole
- 70-80% of LV coronary flow occurs in diastole
- During systole, intramyocardial pressure from contraction compresses vessels, especially the subendocardium
- Tachycardia reduces diastolic time per minute → impairs perfusion
- The subendocardium is most vulnerable (highest wall tension, compressed first)
3. Coronary Vascular Resistance
Three anatomical segments contribute to resistance:
- R1 - Large epicardial arteries (trivial in normal vessels; major site of atherosclerosis)
- R2 - Pre-arteriolar vessels (autoregulatory)
- R3 - Arteriolar and intramyocardial capillaries (metabolic regulation)
Normal coronary circulation: Resistance autoregulates to maintain flow over a MAP range of ~60-130 mmHg. Distal to a significant stenosis, vessels maximally dilate - autoregulatory reserve is exhausted.
4. Coronary Autoregulation
- Vessels dilate with increased demand (metabolic: adenosine, CO₂, O₂) and with decreased perfusion pressure
- In significant CAD, vessels are already maximally dilated distal to stenoses; manipulating perfusion pressure is then the only effective intervention
B. Arterial Oxygen Content
CaO₂ = (Hb × 1.34 × SaO₂) + (0.003 × PaO₂)
Three contributors:
- Hemoglobin concentration - anemia directly reduces oxygen-carrying capacity
- Hemoglobin saturation (SaO₂) - hypoxemia reduces supply
- Dissolved oxygen (PaO₂) - minor contribution at normal PaO₂
The minimum safe hemoglobin in CAD is not firmly established but is influenced by heart rate, perfusion pressure, and myocardial wall thickness.
Part 3: Factors Affecting Myocardial O₂ Supply-Demand Balance During Anesthesia
Anesthesia introduces a unique set of physiological perturbations, often simultaneously affecting both supply and demand. The goal of anesthetic management in cardiac patients is to maintain balance by avoiding tachycardia, hypotension, hypertension, and anemia.
Factors That Increase Demand (and thus Risk of Ischemia)
| Trigger | Mechanism | Hemodynamic consequence |
|---|---|---|
| Laryngoscopy/intubation | Intense sympathetic stimulation | Tachycardia + hypertension → ↑↑ MVO₂ |
| Light anesthesia / painful stimuli | Catecholamine surge | Tachycardia, hypertension, ↑ contractility |
| Emergence/extubation | Sympathoadrenal activation | Tachycardia, hypertension |
| Shivering | Massive ↑ metabolic rate | ↑ cardiac output demand |
| Hypercarbia | Sympathomimetic → tachycardia | ↑ MVO₂ |
| Fluid overload | ↑ LVEDV → ↑ wall tension | ↑ demand + ↑ LVEDP impairs supply |
Factors That Reduce Supply (and thus Risk of Ischemia)
| Trigger | Mechanism | Consequence |
|---|---|---|
| Hypotension (induction, hemorrhage, neuraxial) | ↓ Aortic diastolic pressure → ↓ CPP | ↓ Coronary blood flow |
| Tachycardia | ↓ Diastolic duration | ↓ LV perfusion time |
| Anemia (dilution, hemorrhage) | ↓ CaO₂ | ↓ O₂ delivery |
| Hypoxemia | ↓ SaO₂ | ↓ CaO₂ |
| Elevated LVEDP | Raised filling pressures compressing subendocardium | ↓ Subendocardial perfusion |
| Coronary vasospasm | Triggered by surgical stress, catecholamines, hypothermia | ↓ Regional flow |
| Volatile anesthetics (high concentration) | Myocardial depression + vasodilation | ↓ CPP from hypotension |
Volatile Anesthetic-Specific Effects
- At controlled concentrations, volatile agents (sevoflurane, desflurane, isoflurane) provide ischemic preconditioning (cardioprotective) and reduce MVO₂ by reducing contractility and heart rate
- At excessive concentrations: myocardial depression + systemic vasodilation → hypotension → ↓ CPP
- Isoflurane raised early concern for "coronary steal" (vasodilation of non-stenotic vessels diverting flow away from stenotic territories), though clinical significance remains debated
- Desflurane can cause reflex tachycardia during rapid increase in concentration - directly harmful in CAD
Neuraxial Anesthesia Effects
- High thoracic epidural/spinal: sympathectomy → bradycardia + hypotension → ↓ CPP
- However, in CAD patients, the anti-sympathetic effect can be beneficial by reducing MVO₂ (lower heart rate, lower afterload)
- Risk: abrupt hypotension with single-shot spinal is poorly tolerated; gradual epidural titration is safer
Positive-Pressure Ventilation
- Increases intrathoracic pressure → reduces venous return → ↓ preload → may ↓ cardiac output
- Can reduce LVEDP (beneficial for subendocardial perfusion) or cause hypotension (harmful to CPP)
- PEEP elevates right heart pressures, may reduce coronary perfusion pressure
Summary Diagram
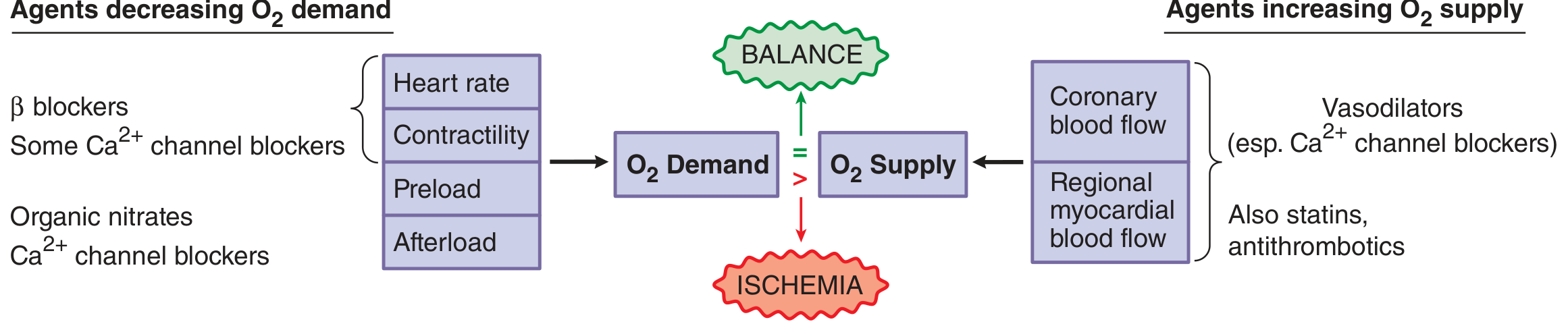
From Goodman & Gilman's - Agents modifying myocardial O₂ supply-demand balance
Key Perioperative Targets to Prevent Ischemia
| Parameter | Target |
|---|---|
| Heart rate | 60-80 bpm (avoid tachycardia above all else) |
| Blood pressure | Maintain SBP within 20% of baseline; adequate diastolic for CPP |
| Hemoglobin | Typically >8-10 g/dL in CAD; threshold individualized |
| LVEDP | Avoid volume overload; maintain adequate but not excessive preload |
| Anesthetic depth | Sufficient to blunt sympathetic responses (laryngoscopy, incision) |
Sources:
- Miller's Anesthesia 10e, "Determinants of Myocardial Oxygen Supply and Demand," pp. 7585-7586
- Harrison's Principles of Internal Medicine 22e, "Pathophysiology of Ischemic Heart Disease," p. 2134
- Goodman & Gilman's Pharmacological Basis of Therapeutics, "Pathophysiology of Myocardial Ischemia," Fig. 31-1
- Morgan & Mikhail's Clinical Anesthesiology 7e, "Anesthetic Management in Valvular Disease," p. 770
This is a shared conversation. Sign in to Orris to start your own chat.