Hookworm -etiology, pathogenesis, lifecycle, diagnosis, treatment, important points
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, multi-source data. Let me compile the complete answer.
Hookworm - Complete Overview
1. Etiology (Causative Agents)
Primary human hookworms:
| Species | Attachment Organ | Geographic Predominance | Eggs/day (female) |
|---|---|---|---|
| Necator americanus | Cutting plates | Tropics/subtropics worldwide; Americas, sub-Saharan Africa, Asia | 5,000-10,000 |
| Ancylostoma duodenale | Biting teeth (2 pairs) | Mediterranean, Middle East, North India, China, Japan | 10,000-30,000 |
| Ancylostoma ceylanicum | - | Southeast Asia (zoonotic - cats/dogs) | - |
Zoonotic species (do NOT complete life cycle in humans):
- A. caninum (dog hookworm) - causes eosinophilic enteritis (Australia) and cutaneous larva migrans
- A. braziliense (cat hookworm) - classic cause of cutaneous larva migrans
- Bunostomum phlebotomum, Uncinaria stenocephala - occasional CLM
Adults measure 7-13 mm, with a dorsally curved anterior end ("hook" shape). Adults reside in the proximal small intestine (mainly jejunum).
2. Lifecycle
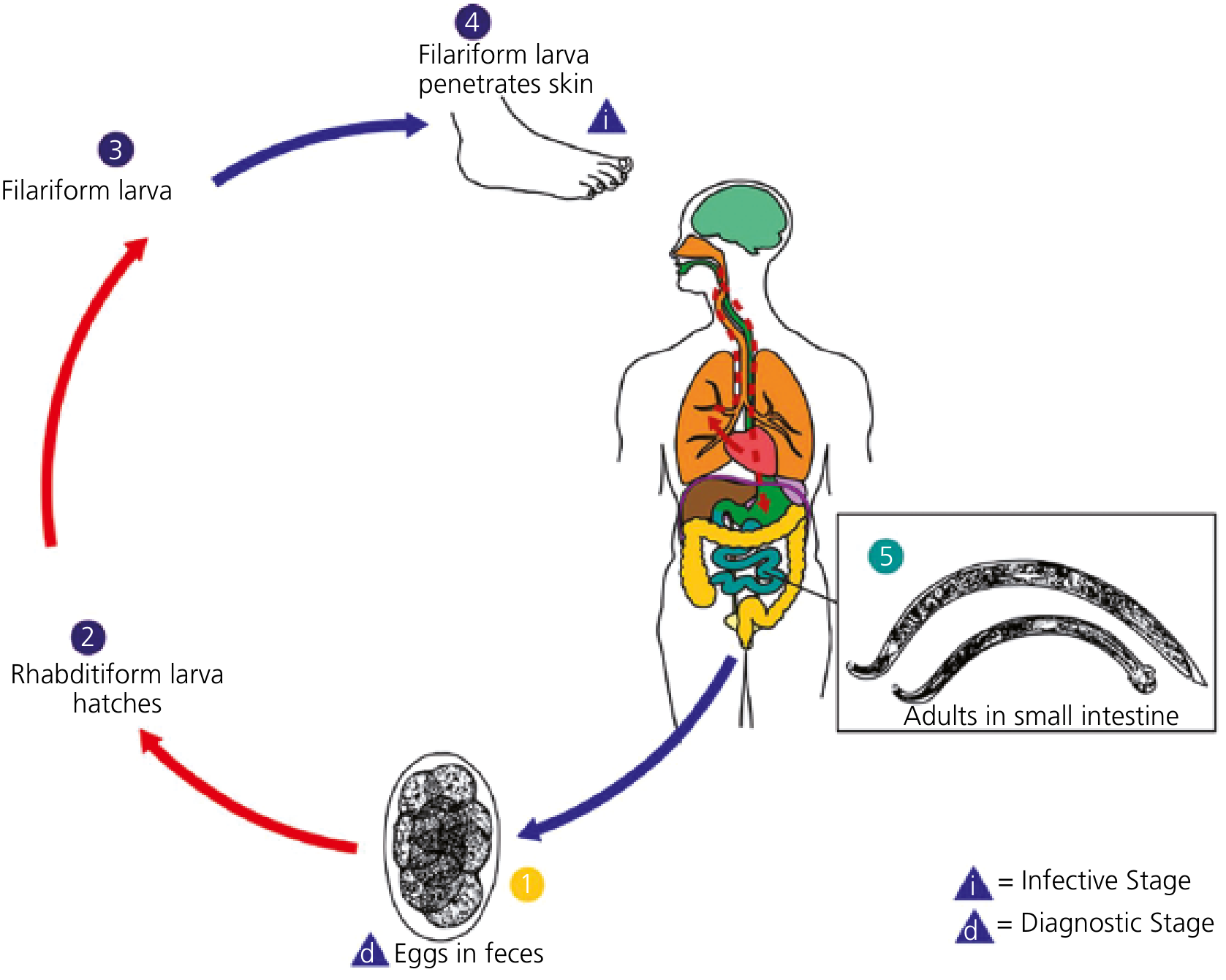
Step-by-step:
- Egg stage: Adult female worms in the small intestine produce eggs that are passed out in feces (diagnostic stage - eggs are 40x60 μm, oval, thin-shelled)
- Rhabditiform larva (L1/L2): In warm, moist soil (23-33°C), eggs hatch within 1-2 days into non-infective rhabditiform larvae, which undergo two molts over 5-10 days
- Filariform larva (L3 - infective stage): Third-stage filariform larvae develop, migrate upward on grass blades, can survive in soil for up to 1 month
- Skin penetration: Infective filariform larvae penetrate unprotected skin (usually feet/hands), triggering "ground itch"
- A. duodenale can also be transmitted orally (ingested larvae survive and develop)
- Migration: Larvae enter venous circulation → pulmonary vasculature → penetrate alveoli → ascend bronchial tree to larynx → swallowed
- Intestinal development: In the small intestine, larvae molt twice more and mature into sexually mature adults
- Prepatent period: 6-8 weeks from skin penetration to eggs in feces (can be longer with Ancylostoma spp.)
Adult worm survival: A. duodenale ~1-14 years; N. americanus ~2-5 years
3. Pathogenesis
3a. Blood Loss - The Core Mechanism
- Adult worms attach to intestinal villi, aspirate a plug of tissue, secrete anticoagulant and antiplatelet enzymes, and ingest blood
- A. duodenale extracts ~0.2 mL blood/worm/day
- N. americanus extracts ~0.03 mL blood/worm/day
- Worms move frequently, leaving bleeding points at old attachment sites
- Accumulated blood loss in heavy/prolonged infection leads to iron-deficiency anemia and hypoalbuminemia
3b. Three Phases of Disease
Phase 1 - Skin Entry ("Ground Itch"):
- Pruritic erythematous maculopapular rash at site of larval penetration
- More common with N. americanus; typically between toes or on ankles
- Resolves spontaneously within days
Phase 2 - Pulmonary Migration (Larval Phase):
- Dry cough, sore throat, wheezing, low-grade fever
- Less frequent and less severe than in ascariasis
- Transient eosinophilia
- Loeffler-like syndrome is uncommon
Phase 3 - Intestinal/Chronic Phase:
- Epigastric pain, abdominal bloating, abnormal peristalsis
- Chronic iron-deficiency anemia (hypochromic microcytic) - severity depends on worm burden, dietary iron intake, concurrent blood loss
- Hypoalbuminemia (protein-losing enteropathy) in heavy infections
- Fatigue, weakness, exertional dyspnea
- In children: growth retardation, cardiac failure (with severe anemia), kwashiorkor-like picture
- In pregnant women: increased maternal/fetal morbidity (~44 million pregnant women infected globally)
3c. Immune Response
- Elicits humoral antibody response and immediate hypersensitivity
- Peripheral eosinophilia and gut eosinophilia
- Eosinophils may play a role in worm destruction; however, evidence that immune responses significantly limit infection is lacking
4. Epidemiology
- Global burden: Over 400-700 million people infected worldwide (figures vary by source)
- Estimated 50,000-60,000 deaths/year; collectively extract over 1 million liters of blood/day from infected individuals
- Distributed between 45°N and 30°S latitude; greatest burden in sub-Saharan Africa, Asia, and rural Americas
- Transmission requires: feces-contaminated shady/moist soil + adequate rainfall + high temperature (23-33°C) + direct skin contact
- Risk factors: poverty, no footwear, use of human excrement as fertilizer, poor sanitation
- Prevalence increases through childhood, plateauing by age ~10 years; intensity peaks by age ~20 and may rise again in elderly
- Male sex more commonly infected; women and children more vulnerable to anemia/sequelae
5. Diagnosis
| Method | Details |
|---|---|
| Stool microscopy (gold standard) | Characteristic 40 x 60 μm oval, thin-shelled eggs in feces; stool concentration techniques (e.g., formalin-ether) needed for light infections |
| Fresh vs. old stool | Old (not fresh) stool may show hatched rhabditiform larvae - must be differentiated from Strongyloides stercoralis larvae |
| Species differentiation | Eggs of all three species are indistinguishable by light microscopy |
| PCR | Species-specific; high sensitivity/specificity but remains a research tool, not commercially available |
| CBC | Hypochromic microcytic anemia; eosinophilia in larval migration phase |
| Biochemistry | Hypoalbuminemia in heavy infections |
| Stool egg count | Quantitative Kato-Katz technique - estimates worm burden (correlates with intensity of disease) |
6. Treatment
| Drug | Dose | Notes |
|---|---|---|
| Albendazole | 400 mg once (single dose) OR 400 mg/day x 3 days | 3-day course preferred for N. americanus (lower single-dose efficacy) |
| Mebendazole | 500 mg single dose OR 100 mg BD x 3 days | Effective for both species |
| Pyrantel pamoate | 11 mg/kg (max 1g) x 3 days | Second-line; less effective for N. americanus |
| Iron supplementation | Ferrous sulfate | Concurrent treatment of iron-deficiency anemia |
- For cutaneous larva migrans (zoonotic hookworm): albendazole 400 mg/day x 3-5 days or ivermectin 200 μg/kg x 1-2 days
- Albendazole single dose has lower cure rates for N. americanus than 3-day regimens
- Treat symptomatic disease even when worm burden is light in vulnerable populations (pregnant women, children)
7. Important Points (High-Yield Summary)
-
"Hook" shape of worm = dorsally curved anterior end; name derives from this
-
Two cutting mechanisms: A. duodenale uses biting teeth (2 pairs), N. americanus uses cutting plates - both enable mucosal attachment and blood ingestion
-
Infective stage = filariform (L3) larva - the diagnostic stage in stool = eggs
-
A. duodenale is unique: larvae can also infect orally (swallowed, survive, develop directly)
-
Ground itch = pruritic rash at skin entry site, typically between toes, more common with N. americanus
-
A. duodenale extracts ~7x more blood per worm than N. americanus (0.2 vs 0.03 mL/day) - more anemia-inducing
-
Eggs in old/stale stool may hatch - must distinguish rhabditiform larvae from Strongyloides (S. stercoralis has a longer buccal cavity)
-
Cutaneous larva migrans = serpiginous, creeping track in skin from dog/cat hookworm larvae; a self-limited condition

-
Most infections are asymptomatic - disease develops only with heavy worm burden + prolonged infection + poor dietary iron
-
Pulmonary symptoms less severe than ascariasis - remember this distinction for exams
-
PCR for species differentiation - eggs are morphologically identical between species
-
WHO mass drug administration (MDA) targets school-age children in endemic areas using albendazole or mebendazole
-
Prevention: wearing footwear, sanitary disposal of feces, avoiding use of human feces as fertilizer
-
Hyperinfection does NOT occur with hookworm (unlike Strongyloides stercoralis) - key distinguishing feature in immunocompromised patients
-
Wakana disease (A. duodenale oral ingestion): nausea, vomiting, pharyngeal irritation, cough - follows oral ingestion of larvae
Sources: Harrison's Principles of Internal Medicine 22E (2025) - Goldman-Cecil Medicine - Sherris & Ryan's Medical Microbiology 8E - Yamada's Textbook of Gastroenterology 7E - Park's Textbook of Preventive and Social Medicine - Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.