In detail about liver diseasea
Reading File
Finding Sources
Finding Sources
Searching the Web
liver diseases overview classification pathophysiology 2024
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
"liver disease" AND "management" AND "cirrhosis"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the detailed answer.
Liver Disease: A Comprehensive Overview
The liver is the body's largest solid organ and performs over 500 functions - synthesis of clotting factors, albumin, and bile; metabolism of drugs, bilirubin, and toxins; gluconeogenesis; and immune defense. Liver disease refers to any condition impairing these functions, classified broadly as acute (onset and resolution within 6 months) or chronic (>6 months duration). Chronic disease is the more clinically significant category, as sustained injury inevitably leads to fibrosis, cirrhosis, and organ failure.
1. Anatomy & Functional Overview
The functional unit of the liver is the hepatic lobule (or acinus). Hepatocytes carry out most metabolic activity. The liver receives dual blood supply:
- Portal vein (~75%) - carries nutrient-rich blood from the gut
- Hepatic artery (~25%) - carries oxygenated blood
Blood drains via hepatic veins into the inferior vena cava. Bile is secreted by hepatocytes into bile canaliculi, which drain into the biliary tree.
2. Classification of Liver Diseases
| Category | Examples |
|---|---|
| Viral hepatitis | Hepatitis A, B, C, D, E |
| Alcohol-related | Steatosis, alcoholic hepatitis, cirrhosis |
| Metabolic/Fatty | NAFLD/NASH/MASLD, hemochromatosis, Wilson disease, α1-antitrypsin deficiency |
| Autoimmune | Autoimmune hepatitis, primary biliary cholangitis, PSC |
| Vascular | Budd-Chiari syndrome, cardiac cirrhosis, portal vein thrombosis |
| Drug-induced | DILI (acetaminophen, isoniazid, many others) |
| Infiltrative/Neoplastic | HCC, metastases, lymphoma, amyloidosis |
| Cholestatic | Biliary atresia, intrahepatic cholestasis |
(Schwartz's Principles of Surgery, 11e, p. 1391)
3. Viral Hepatitis
Hepatitis A (HAV)
- Fecal-oral transmission; self-limiting; no chronic form
- Vaccines available; supportive treatment
Hepatitis B (HBV)
- Bloodborne/sexual/vertical transmission
- Acute infection: 90-95% of adults clear spontaneously
- Chronic HBV: defined as HBsAg+ for >6 months; 5-10% of adults progress to chronic disease
- Major complication: cirrhosis and HCC
- Treatment: tenofovir, entecavir (nucleotide analogues)
Hepatitis C (HCV)
- Bloodborne transmission; most common cause of chronic liver disease
- ~75-85% of acute infections become chronic
- Can progress to cirrhosis over 20-30 years
- Curative with direct-acting antivirals (DAAs) - >95% SVR
- (Schwartz's Principles of Surgery, 11e)
Hepatitis D (HDV)
- Co-infection or superinfection with HBV only; worsens prognosis
Hepatitis E (HEV)
- Fecal-oral; self-limiting in immunocompetent; can be severe in pregnancy
4. Alcohol-Related Liver Disease (ALD)
ALD spans a spectrum from simple steatosis to steatohepatitis to cirrhosis.
Pathological progression:
- Steatosis (fatty liver): reversible with abstinence; mild elevation in ALP and bilirubin
- Alcoholic steatohepatitis (ASH): hepatocyte necrosis, Mallory bodies, neutrophilic infiltrate, perivenular inflammation
- Cirrhosis: irreversible; 15-20 years of excess drinking typically required; steatohepatitis can occur after weeks-months of heavy use
Key lab findings in ALD:
- AST:ALT ratio >2:1 (distinguishing feature from other liver diseases)
- Transaminases rarely exceed 500 U/mL
- Hyperbilirubinemia, elevated ALP, neutrophilic leukocytosis
Prognosis:
- Each bout of alcoholic hepatitis carries 10-20% risk of death
- With repeated bouts, cirrhosis develops in ~1/3 of patients within a few years
- 5-year survival ~90% with abstinence (free of jaundice/ascites/hematemesis) vs. 50-60% in those who continue drinking
- Causes of death: hepatic failure, massive GI hemorrhage, intercurrent infection, hepatorenal syndrome, HCC (3-6%)
(Robbins & Kumar Basic Pathology)
5. Nonalcoholic Fatty Liver Disease (NAFLD) / MASLD
NAFLD is now the most common chronic liver disease worldwide, driven by the global obesity epidemic.
Spectrum:
- Simple steatosis (NAFL): hepatic fat >5% without inflammation; largely benign
- NASH (nonalcoholic steatohepatitis): steatosis + hepatocyte injury + inflammation + fibrosis
- NASH cirrhosis + HCC risk
Associations: insulin resistance, metabolic syndrome, obesity, type 2 diabetes, dyslipidemia, hypertension
Nomenclature update: The term MASLD (metabolic dysfunction-associated steatotic liver disease) has replaced NAFLD in current guidelines to better reflect the underlying metabolic etiology.
Epidemiology:
- NAFLD prevalence: ~25% globally
- NASH affects 3-5% of the population
- ~1 in 10 NASH patients progress to cirrhosis
- NASH is increasingly the leading cause of HCC (surpassing HCV in many populations)
(Schwartz's Principles of Surgery, 11e, p. 1391; Robbins & Kumar Basic Pathology)
6. Cirrhosis
Cirrhosis is the final common pathway of chronic hepatic injury, characterized by widespread fibrous septa dividing the parenchyma into hepatocellular regenerative nodules.
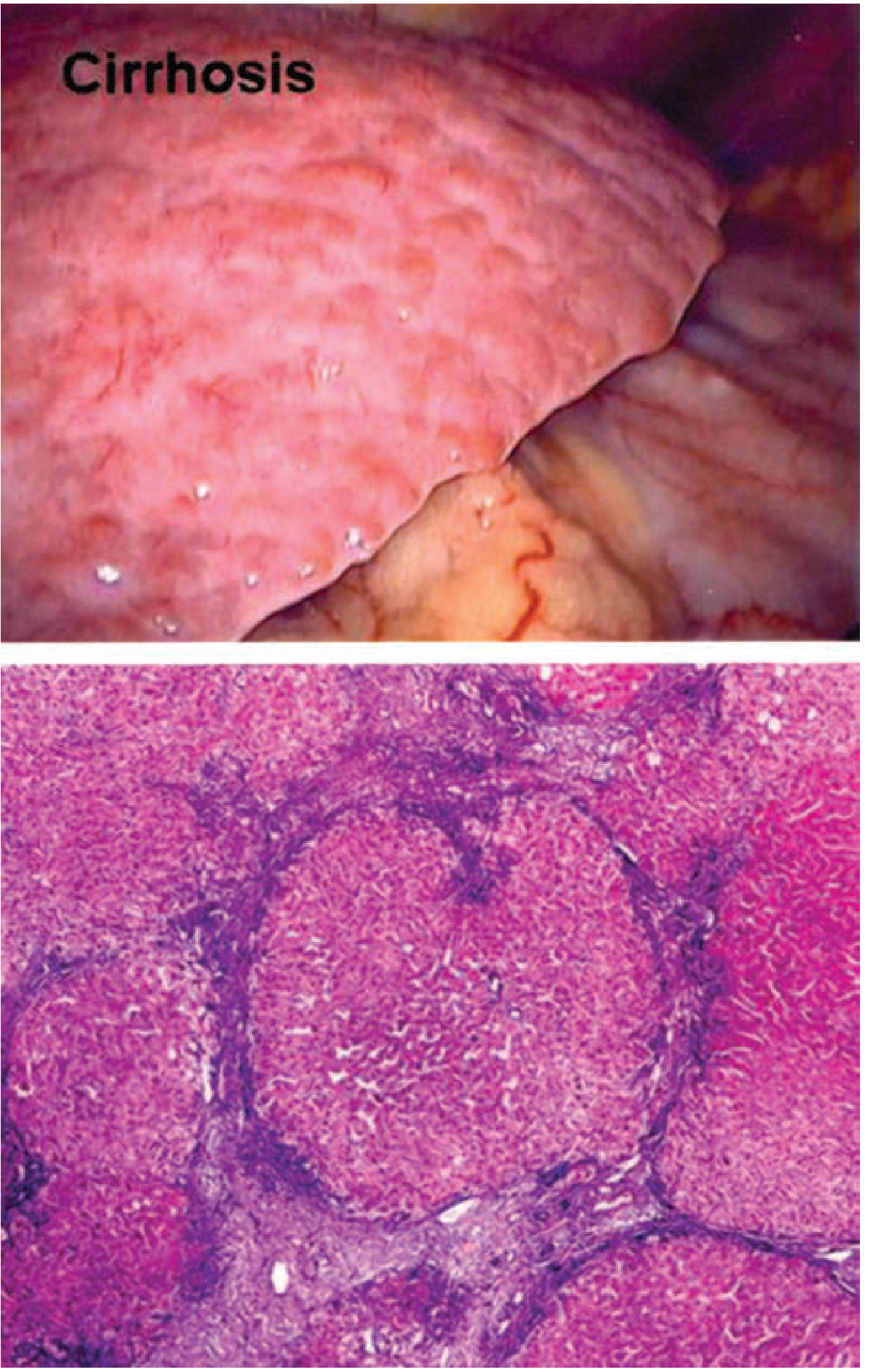
Figure: Grossly cirrhotic liver (top) and regenerative nodules with bridging fibrosis on H&E stain (bottom). - Schwartz's Principles of Surgery, 11e
Morphologic Classification
| Type | Features |
|---|---|
| Micronodular | Thick regular septa, small uniform nodules (<3mm); e.g., alcoholic |
| Macronodular | Varying nodule and septa sizes; e.g., viral hepatitis |
| Mixed | Transition from micro to macronodular (dynamic) |
Epidemiology
- Causes 30,000 deaths/year in the United States
- 5-year mortality of ESLD: 50% (70% from liver failure itself)
- 40% of cirrhotic patients are asymptomatic at presentation
Prognosis (Symptom to Diagnosis, 4e)
| Stage | 1-Year Mortality |
|---|---|
| No varices, no ascites | ~1% |
| Varices, no ascites | ~3.4% |
| Varices + ascites | ~20% |
| Variceal bleeding + ascites | ~57% |
- Median survival from diagnosis of compensated cirrhosis: 10-13 years
- Up to 60% progress to decompensated cirrhosis by 10 years
- After decompensation without transplant: 85% 5-year mortality
7. Complications of Cirrhosis / End-Stage Liver Disease (ESLD)
A. Portal Hypertension
Portal hypertension is defined as hepatic venous pressure gradient (HVPG) >10 mmHg (measured by wedged hepatic venous pressure - free hepatic venous pressure).
Classification by level of obstruction:
| Type | Examples |
|---|---|
| Presinusoidal | Portal/splenic vein thrombosis, schistosomiasis |
| Sinusoidal | Cirrhosis (most common in the US), hepatitis |
| Postsinusoidal | Budd-Chiari, cardiac failure, hepatic vein occlusion |
Consequences:
- Formation of portosystemic collaterals (varices)
- Splanchnic vasodilation
- Renal vasoconstriction - salt and water retention
- Increased cardiac output
- Decreased production of albumin and clotting factors
- Edema (low oncotic pressure + increased hydrostatic pressure)
(Symptom to Diagnosis, 4e, p. 326)
B. Variceal Bleeding
- Gastroesophageal varices form via the coronary (left gastric) vein
- HVPG >12 mmHg is threshold for variceal bleeding
- Management:
- Acute: IV octreotide (splanchnic vasoconstriction) + endoscopic band ligation
- Prevention: non-selective beta-blockers (propranolol, nadolol) or band ligation
- Refractory: TIPS (transjugular intrahepatic portosystemic shunt) - controls bleeding in >90% of cases
- TIPS complications: hepatic encephalopathy (25-30%), stent thrombosis, decreased hepatic function
C. Ascites
- Combination of portal hypertension + hypoalbuminemia + sodium retention
- Diagnosed by paracentesis; SAAG ≥1.1 g/dL indicates portal hypertension
- Treatment: sodium restriction, diuretics (spironolactone ± furosemide), large-volume paracentesis for refractory cases
D. Hepatic Encephalopathy (HE)
- Neuropsychiatric dysfunction from portosystemic shunting of ammonia and other toxins
- Grading scale (West Haven):
- Grade 1: subtle change in consciousness
- Grade 2: disoriented, inappropriate behavior
- Grade 3: somnolent but arousable
- Grade 4: comatose
- Treatment: lactulose (reduces ammonia), rifaximin (antibiotic to alter gut flora)
E. Hepatorenal Syndrome (HRS)
- Functional renal failure in advanced cirrhosis; diagnosis of exclusion
- Type 1 (acute): rapid GFR decline; often precipitated by SBP, hemorrhage; poor prognosis
- Type 2 (chronic): slower decline; associated with refractory ascites
- Treatment: terlipressin + albumin; bridge to liver transplant
F. Spontaneous Bacterial Peritonitis (SBP)
- Infection of ascitic fluid (PMNs >250/mm³); most common organism: E. coli
- Prophylaxis: norfloxacin in high-risk patients
- Treatment: IV cefotaxime + IV albumin (prevents HRS)
G. Hepatopulmonary Syndrome & Portopulmonary Hypertension
- Hepatopulmonary: intrapulmonary vascular dilation → hypoxemia
- Portopulmonary: pulmonary arterial hypertension from portal hypertension
H. Coagulopathy
- Decreased synthesis of coagulation factors (I, II, V, VII, VIII, IX, X, XI)
- Factor V (shortest half-life) is the most sensitive marker for acute deterioration
- INR elevation reflects synthetic dysfunction
8. Acute Liver Failure (ALF)
Definition: Rapid development of severe liver injury with encephalopathy and coagulopathy (INR ≥1.5) in a patient without pre-existing liver disease, within <6 months of symptom onset.
Subtypes:
| Type | Onset to Encephalopathy | Common Cause | Prognosis |
|---|---|---|---|
| Hyperacute | <7 days | Acetaminophen, HAV, HEV | Best |
| Acute | 8-28 days | HBV, drug-induced | Intermediate |
| Subacute | 5-12 weeks | Idiopathic, drugs | Worst |
Common causes: acetaminophen toxicity (#1 in Western countries), viral hepatitis, idiosyncratic DILI, autoimmune hepatitis, Wilson's disease, Budd-Chiari, AFLP (in pregnancy)
Management:
- ICU admission; address neurologic, respiratory, hemodynamic, infectious, and renal complications
- N-acetylcysteine (NAC): 140 mg/kg loading dose → 70 mg/kg q4h for acetaminophen toxicity; also used in non-acetaminophen ALF (especially grade 1-2 encephalopathy)
- Cause-specific: nucleoside analogues for HBV, acyclovir for HSV, copper chelation for Wilson's
- King's College Criteria or MELD score to determine transplant listing priority
(Goldman-Cecil Medicine, International Edition; Yamada's Textbook of Gastroenterology, 7e)
9. Other Important Liver Diseases
Autoimmune Hepatitis (AIH)
- Predominantly affects women; associated with HLA-DR3 and DR4
- Labs: elevated IgG, ANA and/or anti-smooth muscle antibodies (Type 1); anti-LKM1 (Type 2)
- Treatment: prednisolone ± azathioprine
Primary Biliary Cholangitis (PBC)
- Chronic cholestatic disease; autoimmune destruction of intrahepatic bile ducts
- Anti-mitochondrial antibodies (AMA-M2) in >90% of cases
- Treatment: ursodeoxycholic acid (UDCA)
Primary Sclerosing Cholangitis (PSC)
- Fibro-inflammatory stricturing of bile ducts; strongly associated with IBD (especially UC)
- Elevated ALP, characteristic "beading" on MRCP/ERCP
- No effective medical therapy; liver transplant for end-stage disease
Hereditary Hemochromatosis
- Autosomal recessive (HFE gene mutations C282Y, H63D)
- Iron deposition in liver, heart, pancreas, joints, pituitary
- Complications: cirrhosis, HCC, diabetes, cardiomyopathy
- Treatment: therapeutic phlebotomy
Wilson's Disease
- Autosomal recessive (ATP7B mutations); copper accumulation
- Manifestations: liver disease, neuropsychiatric symptoms, Kayser-Fleischer rings
- Labs: low ceruloplasmin, elevated 24-hr urine copper
- Treatment: D-penicillamine, trientine, or zinc
α1-Antitrypsin Deficiency
- PiZZ phenotype most common; abnormal protein accumulates in hepatocytes
- Causes cirrhosis and emphysema
- Treatment: liver transplant for end-stage disease
10. Assessment of Liver Disease Severity
Child-Pugh Score
Scores bilirubin, albumin, PT/INR, ascites, encephalopathy:
- Class A (5-6): compensated; good prognosis
- Class B (7-9): moderate compromise
- Class C (10-15): decompensated; poor prognosis
MELD Score (Model for End-Stage Liver Disease)
- Formula: 3.78(ln serum bilirubin mg/dL) + 11.2(ln INR) + 9.57(ln serum creatinine mg/dL) + 6.43
- Predicts 90-day mortality; used for transplant organ allocation
- MELD ≤6 or UKELD ≤42 - low risk of liver-related complications during pregnancy
Laboratory Tests
| Test | Significance |
|---|---|
| AST, ALT (transaminases) | Hepatocellular injury |
| ALP, GGT | Cholestatic disease |
| Bilirubin | Synthetic/excretory function |
| Albumin, PT/INR | Synthetic function |
| Platelet count | Low (<110 x10³/mcL) strongly suggests cirrhosis (LR+ = 9.8) |
11. Hepatocellular Carcinoma (HCC)
- Most common primary liver malignancy
- Risk factors: HBV, HCV, cirrhosis (of any cause), NAFLD/NASH, aflatoxin, alcohol, metabolic syndrome
- HCC is the most rapidly increasing neoplasm in the United States (10,000-12,000 deaths/year)
- Surveillance: ultrasound ± AFP every 6 months in high-risk patients
- Diagnosis confirmed by multiphasic CT or MRI (arterial enhancement + portal washout = LI-RADS 5)
- Treatment: curative resection, ablation, TACE, sorafenib/lenvatinib, liver transplant (Milan criteria)
12. Liver Transplantation
The only definitive treatment for end-stage liver disease. Key indications:
- Decompensated cirrhosis (MELD ≥15-18)
- HCC within Milan criteria (single tumor ≤5cm or ≤3 tumors all ≤3cm)
- Acute liver failure
- Metabolic liver diseases (Wilson's, α1-AT deficiency, etc.)
Contraindications include active alcohol/substance use, extrahepatic malignancy, severe cardiopulmonary disease, and sepsis.
Recent Evidence (2024-2025)
- A 2025 meta-analysis on alcohol-associated hepatitis confirmed high short-term mortality and identified key risk factors
- AI/machine learning in MASLD risk stratification is an active area per a 2026 systematic review (PMID 40850679)
- MASLD (metabolic dysfunction-associated steatotic liver disease) is the new preferred terminology replacing NAFLD in 2023 guidelines
Summary
Liver disease is a broad spectrum with multiple etiologies converging on the same endpoint - cirrhosis, portal hypertension, hepatic failure, and HCC. The key principles are:
- Identify and remove the cause (abstinence, antivirals, immunosuppression, chelation)
- Manage complications of portal hypertension and synthetic dysfunction
- Monitor for HCC with regular surveillance
- Transplant in appropriately selected patients with end-stage disease
Sources:
- Schwartz's Principles of Surgery, 11e
- Robbins & Kumar Basic Pathology
- Goldman-Cecil Medicine, International Edition
- Yamada's Textbook of Gastroenterology, 7e
- Symptom to Diagnosis: An Evidence-Based Guide, 4e
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.