NSAID s
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Searching PubMed
NSAIDs cardiovascular risk gastrointestinal safety
I now have comprehensive information to write a thorough answer on NSAIDs. Let me compile everything.
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
Overview
NSAIDs are one of the most widely prescribed drug classes worldwide, used for their analgesic, anti-inflammatory, and antipyretic effects. They form Step 1/2 of multimodal analgesic regimens and are used in pain, fever, inflammation, and numerous chronic conditions.
Mechanism of Action
NSAIDs work by inhibiting cyclooxygenase (COX) enzymes, which convert arachidonic acid (released from membrane phospholipids by phospholipases) into PGH2 - the precursor of all prostanoids (prostaglandins, prostacyclins, thromboxanes).
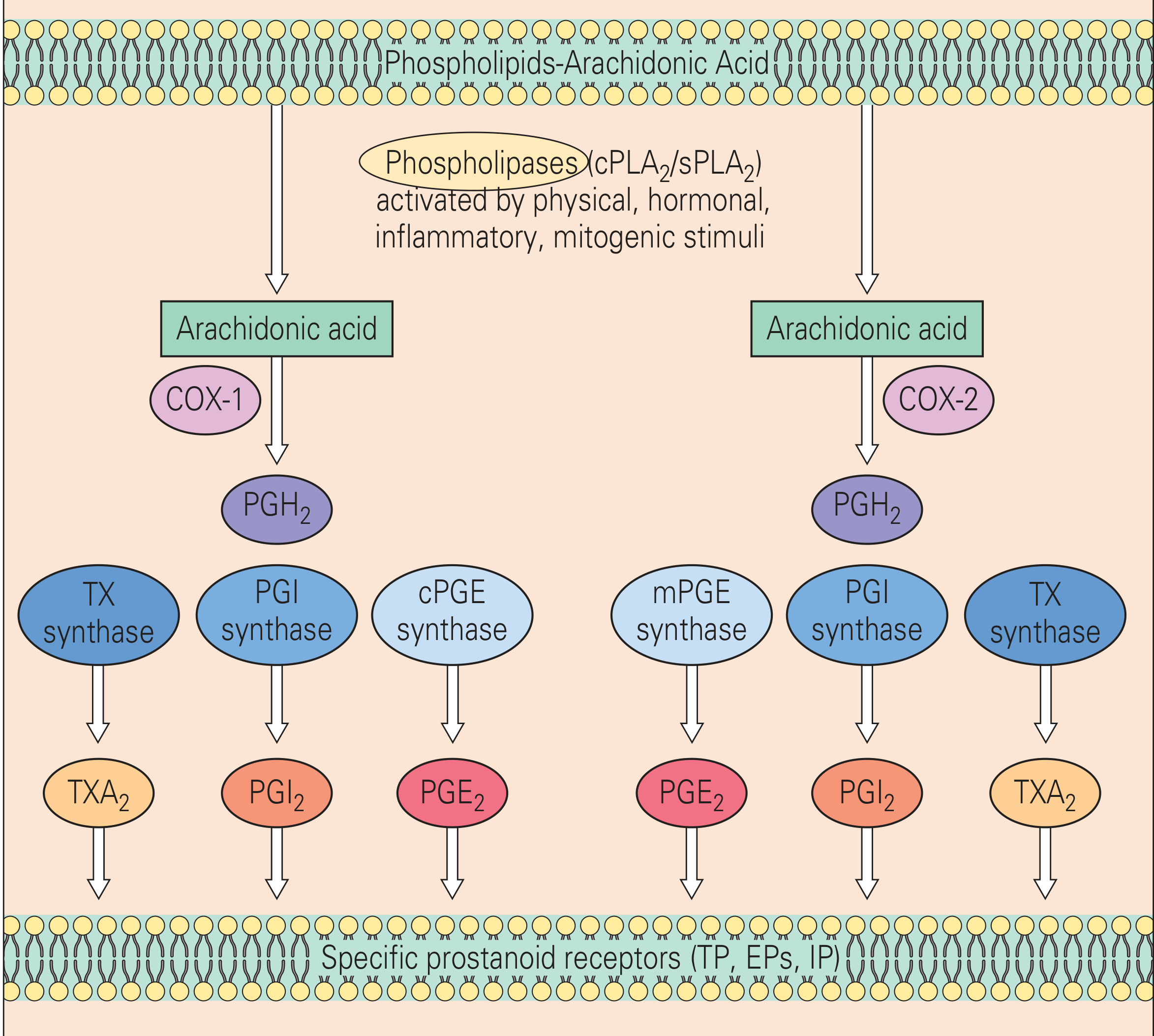
The figure above shows how both COX-1 and COX-2 convert arachidonic acid to PGH2, which is then converted by tissue-specific isomerases to TXA2, PGI2 (prostacyclin), and PGE2.
There are two main COX isoforms:
| Feature | COX-1 | COX-2 |
|---|---|---|
| Expression | Constitutive (always present) | Inducible (upregulated by inflammation, cytokines) |
| Location | Platelets, gastric mucosa, kidney, endothelium | Sites of inflammation, kidney, brain, endothelium |
| Products | TXA2 (platelet aggregation), PGI2, PGE2 (gastric protection) | PGE2 (inflammation, pain, fever), PGI2 |
| Role | Housekeeping functions | Inflammation, pain, fever |
By inhibiting COX, NSAIDs block:
- Prostaglandin synthesis → less pain sensitization and inflammation
- Thromboxane A2 (via COX-1) → reduced platelet aggregation
- Prostacyclin (PGI2) (via COX-2) → vasodilation lost → potential pro-thrombotic state with selective COX-2 inhibitors
Classification
1. Non-selective COX-1 + COX-2 Inhibitors (tNSAIDs)
These inhibit both isoforms to varying degrees:
- Propionic acids: Ibuprofen, Naproxen, Ketoprofen, Flurbiprofen
- Acetic acids: Indomethacin, Diclofenac, Ketorolac, Sulindac, Etodolac
- Oxicams: Piroxicam, Meloxicam (mild COX-2 preference)
- Fenamates: Mefenamic acid
- Pyrazolones: Phenylbutazone (largely withdrawn)
- Salicylates: Aspirin (special - see below)
2. Selective COX-2 Inhibitors (Coxibs)
- Celecoxib, Etoricoxib, Parecoxib (parenteral)
- Former members (withdrawn due to CV risk): Rofecoxib (Vioxx), Valdecoxib, Lumiracoxib
3. Aspirin - Unique NSAID
Aspirin irreversibly acetylates a serine residue in the COX active site, permanently inactivating both COX-1 and COX-2. Because platelets lack a nucleus (cannot synthesize new enzyme), the antiplatelet effect lasts for the entire platelet lifespan (7-10 days). All other NSAIDs are reversible inhibitors. - Quick Compendium of Clinical Pathology, 5th ed.
COX-2 Selectivity Spectrum
The plot below shows the COX-2 selectivity of various drugs based on their IC50 ratios. Drugs to the right of the diagonal line have greater COX-2 than COX-1 selectivity:
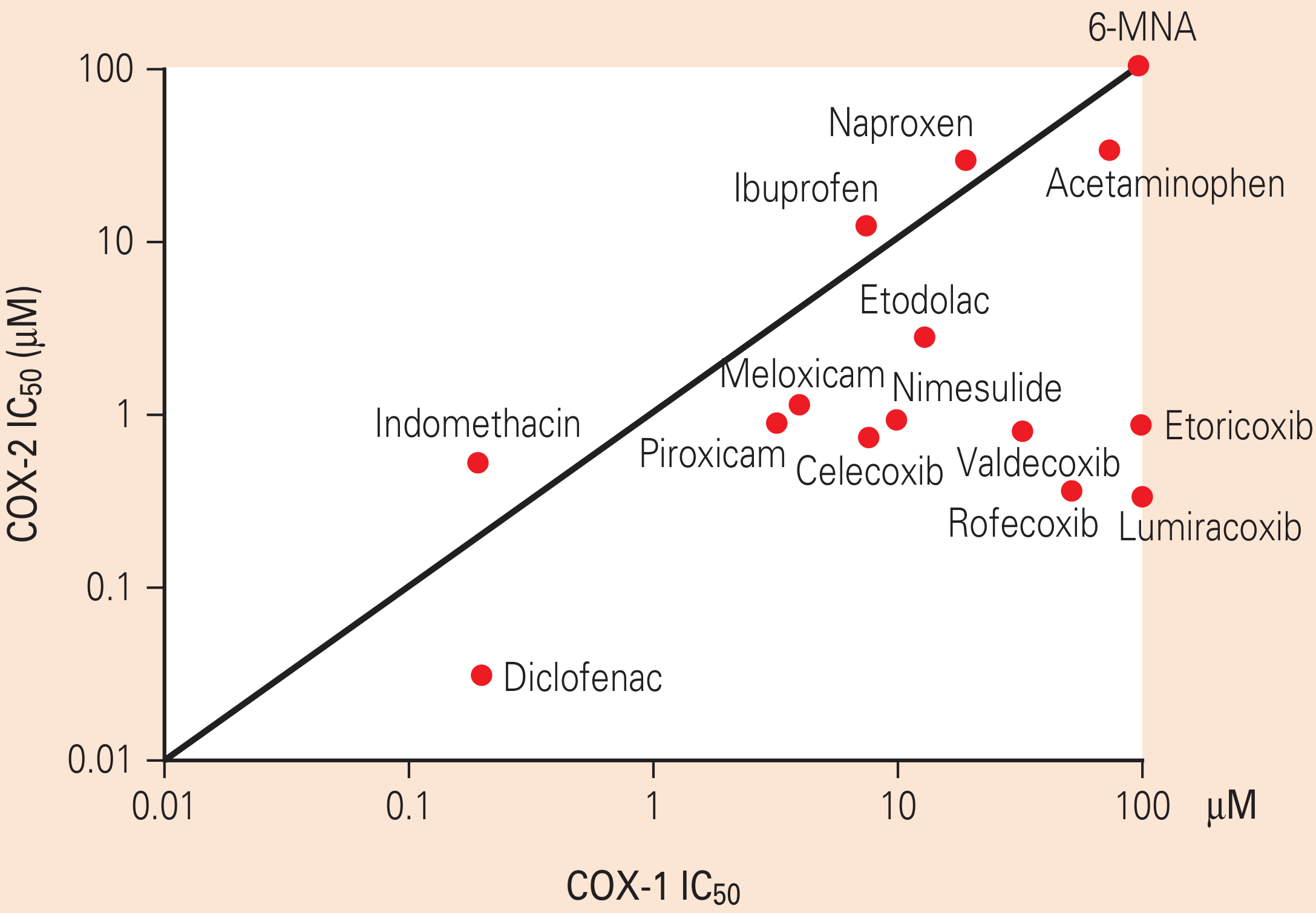
Key insight: Indomethacin is strongly COX-1 preferring; Diclofenac shows marked COX-2 preference despite being a "non-selective" NSAID; Celecoxib, Rofecoxib, Etoricoxib are the true coxibs with strong COX-2 selectivity.
Pharmacological Effects
| Effect | Mechanism |
|---|---|
| Analgesia | Block PGE2/PGI2 sensitization of nociceptors; also central action at spinal cord |
| Anti-inflammation | Reduce PGE2 and PGI2 at inflammatory sites; decreased vasodilation, edema |
| Antipyresis | Block PGE2 synthesis in hypothalamus (resets the thermostat) |
| Antiplatelet | COX-1 inhibition reduces TXA2-driven platelet aggregation |
| Uricosuric | Some (e.g., sulindac) have mild uricosuric effects |
Clinical Uses
- Acute pain: Post-operative, dental, musculoskeletal, headache
- Chronic inflammation: Rheumatoid arthritis, osteoarthritis, ankylosing spondylitis, psoriatic arthritis
- Acute gout attack: High-dose naproxen or indomethacin
- Dysmenorrhea: First-line (ibuprofen, naproxen)
- Fever: Second line after paracetamol in adults
- Pericarditis: Aspirin or ibuprofen
- Patent ductus arteriosus: Indomethacin IV (closes PDA in neonates)
- Tocolysis: Indomethacin (inhibits uterine prostaglandin synthesis)
- Cardiovascular prophylaxis: Low-dose aspirin (antiplatelet)
- Actinic keratoses: Topical diclofenac 3% gel
Adverse Effects
Gastrointestinal (most common)
- Mucosal damage from COX-1 inhibition: loss of protective PGE2/PGI2 → reduced mucus, bicarbonate, blood flow
- Ranges from dyspepsia to gastric/duodenal ulcers and upper GI bleeding
- COX-2-selective inhibitors significantly reduce GI risk
- Management: Add a proton pump inhibitor (PPI) for high-risk patients; consider misoprostol
- A 2026 meta-analysis (PMID: 40915652) confirmed all NSAIDs increase GI bleeding risk
Cardiovascular
- COX-2 inhibition reduces PGI2 (vasodilatory/anti-thrombotic) without reducing TXA2 → net prothrombotic state
- Risk of myocardial infarction and stroke, especially with selective COX-2 inhibitors
- Even ibuprofen and naproxen carry some CV risk at high doses
- Coxibs are contraindicated in perioperative CABG patients
- Reduced renal PGI2/PGE2 → sodium/water retention → elevated blood pressure regardless of antihypertensive being taken - Rheumatology 2-Volume Set (Elsevier, 2022)
Renal
- Prostaglandins dilate the afferent arteriole to maintain GFR, especially in states of reduced perfusion (heart failure, dehydration, cirrhosis)
- NSAID use → afferent arteriole constriction → decreased GFR → acute kidney injury
- Chronic use: analgesic nephropathy, interstitial nephritis, papillary necrosis
- Contraindicated in acute/chronic renal failure
Hematological
- Platelet dysfunction → prolonged bleeding time (all NSAIDs); irreversible with aspirin
- Risk of perioperative bleeding (avoid pre-surgery unless specifically indicated)
- NSAIDs displace warfarin from plasma proteins AND impair platelet function → amplify anticoagulation risk
Respiratory
- Aspirin-exacerbated respiratory disease (AERD): In ~10% of asthmatics, NSAIDs divert arachidonic acid to the 5-LOX pathway → leukotrienes → bronchoconstriction
- Can precipitate life-threatening asthma attacks
- Aspirin desensitization is a treatment option
Hepatic
- Rare hepatotoxicity (diclofenac has highest rate among NSAIDs)
- Avoid in severe hepatic impairment
Obstetric
- Contraindicated after 30 weeks gestation: Cause premature closure of the ductus arteriosus and oligohydramnios (reduced fetal renal blood flow)
- Indomethacin is used as a tocolytic before 32 weeks with caution
Drug Interactions
| Drug Affected | NSAID | Effect |
|---|---|---|
| Warfarin | All NSAIDs | Protein binding displacement + platelet inhibition → increased bleeding risk |
| Lithium | All NSAIDs | Inhibit renal excretion → lithium toxicity |
| Antihypertensives | All NSAIDs | Blunt antihypertensive effect (sodium retention, vasoconstriction) |
| Sulfonylureas | Phenylbutazone, azapropazone | Inhibit metabolism → prolonged hypoglycemia |
| Phenytoin | Phenylbutazone | Inhibit metabolism → phenytoin toxicity |
| ACE inhibitors | All NSAIDs | Reduce renal blood flow → hyperkalemia and AKI |
| Antiplatelet drugs | Non-selective NSAIDs (ibuprofen, naproxen) | Compete for COX-1 binding site → blunt aspirin's antiplatelet effect |
Source: Rheumatology, 2-Volume Set (Elsevier, 2022)
Contraindications
| Contraindication | Reason |
|---|---|
| Active peptic ulcer disease | Worsen GI mucosal damage |
| Acute/chronic renal failure | Loss of prostaglandin-dependent renal perfusion |
| Severe hepatic impairment | Impaired metabolism, hepatotoxicity risk |
| Asthma (aspirin-sensitive) | Precipitate bronchospasm via 5-LOX shunting |
| Pregnancy (>30 weeks) | Premature ductus arteriosus closure, oligohydramnios |
| Perioperative CABG | Thrombotic CV events (especially coxibs) |
| Platelet dysfunction / active GI bleed | Worsened hemostasis |
| Hypersensitivity | Cross-reactivity between NSAIDs |
Key Individual Agents
| Drug | Notes |
|---|---|
| Aspirin | Irreversible COX-1/2 inhibitor; low dose = antiplatelet; high dose = anti-inflammatory |
| Ibuprofen | Most commonly used OTC; moderate COX-1 preference; avoid with aspirin |
| Naproxen | Longer half-life (twice daily); may have lowest CV risk among tNSAIDs |
| Indomethacin | Most potent; used for gout, pericarditis, PDA closure; high GI/CNS toxicity |
| Diclofenac | Despite being non-selective, shows marked COX-2 preference in vitro; highest hepatotoxicity among NSAIDs |
| Ketorolac | Parenteral/IM for acute pain; limited to 5 days due to GI toxicity |
| Celecoxib | Selective COX-2; lower GI risk; still carries CV and renal risks |
| Etoricoxib | Highly selective COX-2; not available in all countries |
| Meloxicam | Mild COX-2 preference; lower GI risk than indomethacin |
GI Protection Strategies
For patients requiring NSAIDs who are at high GI risk (age >65, prior ulcer/bleed, concomitant steroids, anticoagulants):
- Prefer a selective COX-2 inhibitor (celecoxib)
- Add a PPI (omeprazole, lansoprazole)
- Add misoprostol (PGE1 analogue) - less used due to GI side effects of misoprostol itself
- Use the lowest effective dose for the shortest duration
Sources: Fischer's Mastery of Surgery 8e; Rheumatology 2-Volume Set (Elsevier 2022); Bailey & Love's Short Practice of Surgery 28e; Ganong's Review of Medical Physiology 26e; Quick Compendium of Clinical Pathology 5e; Goldman-Cecil Medicine
Recent evidence note: A 2026 systematic review and meta-analysis (PMID: 40915652) confirmed that all NSAIDs increase GI bleeding risk, reinforcing the need for gastroprotection in high-risk patients. A 2025 systematic review on celecoxib safety (PMID: 40911151) supports celecoxib's improved GI profile, though cardiovascular and renal monitoring remains necessary.
This is a shared conversation. Sign in to Orris to start your own chat.