Ca endometrium Everything In detail from Dutta
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Important note: DC Dutta's Textbook of Gynecology is not in the medical library. The comprehensive answer above is compiled from Berek & Novak's Gynecology (the most comparable standard gynecology textbook) and Robbins & Cotran Pathologic Basis of Disease - both at the same depth and scope that Dutta covers this topic.
Carcinoma of the Endometrium - Complete Notes
1. Introduction & Epidemiology
- Most common invasive cancer of the female genital tract (Western countries)
- Accounts for 7% of all invasive cancers in females (excluding skin)
- Has overtaken cervical cancer due to better cervical screening programs
- Peak incidence: 55-65 years (postmenopausal); uncommon before age 40
- Incidence in younger women is rising
- About 80% of cases are stage I at diagnosis
2. Risk Factors
All major risk factors share the common mechanism of prolonged unopposed estrogen stimulation:
| Risk Factor | Notes |
|---|---|
| Obesity | Most significant risk factor; peripheral conversion of androgens → estrone in adipose tissue |
| Nulliparity / Infertility | Chronic anovulation |
| Late menopause | Prolonged estrogen exposure |
| Diabetes mellitus | Co-exists; associated with obesity |
| Hypertension | The classic triad: obesity + DM + HTN |
| Unopposed exogenous estrogen | 4-8x increased risk; dose- and time-dependent; risk reduced by adding progestins |
| Tamoxifen | Partial estrogen agonist on endometrium |
| Estrogen-secreting tumors | Granulosa-theca cell tumors |
| PCOS | Chronic anovulation |
| Lynch II syndrome (HNPCC) | Lifetime risk 32-60%; autosomal dominant; MLH1, MSH2, PMS1, PMS2, MSH6 mutations |
Protective: Combined OCP, multiparity, smoking
3. Type I vs Type II Classification
| Feature | Type I | Type II |
|---|---|---|
| Estrogen-dependence | Yes | No |
| Histology | Endometrioid | Serous, clear cell |
| Grade | Low (1, 2) | High (3) |
| Background endometrium | Hyperplasia | Atrophic |
| Patient | Obese, perimenopausal | Thin, older |
| Mutations | PTEN, PIK3CA, KRAS, ARID1A, MSI | TP53 |
| Prognosis | Favorable | Poor |
4. Pathogenesis & Molecular Biology
Type I - Key mutations (all drive PI3K/AKT pathway):
- PTEN: Most common (30-80%); tumor suppressor; loss of function
- PIK3CA: ~40%; activating mutation (encodes PI3K catalytic subunit)
- KRAS: ~25%; activating mutation
- ARID1A: ~1/3; chromatin remodeling; also mutated in endometriosis-associated ovarian cancers
- MMR defects: ~20% sporadic; MLH1 epigenetically silenced; Lynch syndrome has germline MMR mutations
- POLE mutations: <10%; ultramutated; paradoxically excellent prognosis
Type II - Key mutation:
- TP53: >90% of serous carcinomas
TCGA Four Molecular Subtypes (in order of prognosis, best to worst):
- POLE ultramutated - best prognosis
- MSI hypermutated - intermediate
- Copy number low/nonspecific - intermediate
- Copy number high/TP53 mutated - worst (serous-like)
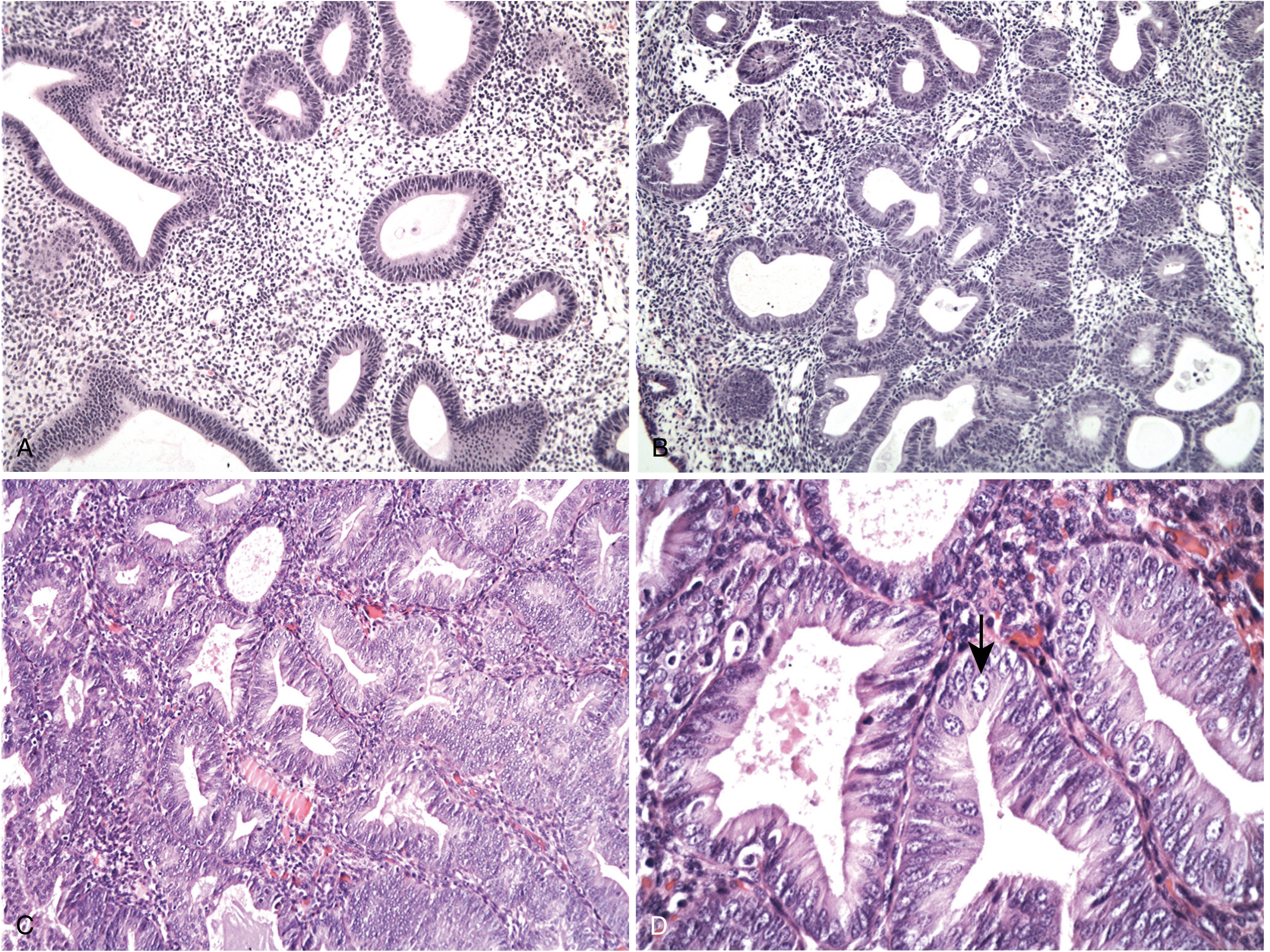
5. Precursor: Endometrial Hyperplasia
- Established precursor to Type I (endometrioid) carcinoma
- WHO classification: Hyperplasia without atypia vs. Atypical Hyperplasia/EIN (endometrial intraepithelial neoplasia)
- Atypical hyperplasia: 25-29% harbor concurrent carcinoma; high progression risk
6. Pathology
Classification of Endometrial Carcinomas:
- Endometrioid adenocarcinoma (+ variants: villoglandular/papillary, secretory, with squamous differentiation)
- Mucinous carcinoma
- Papillary serous carcinoma
- Clear cell carcinoma
- Squamous carcinoma
- Undifferentiated carcinoma
- Mixed carcinoma
Gross Morphology:
- Localized polypoid mass or diffuse involvement of endometrial lining
- Typically arises in fundus
- Spreads: myometrial invasion → adjacent structures → lymph nodes → distant (lungs, liver, bones)
Endometrioid Adenocarcinoma (80-85%):
- Glands resembling normal proliferative endometrium
- Columnar cells, basally oriented nuclei, little intracytoplasmic mucin
- Invasion criteria: desmoplastic stroma, back-to-back glands (no intervening stroma), extensive papillary pattern, squamous differentiation (area >4.2 mm)
- Up to 20% have squamous differentiation (graded by glandular component only)
FIGO Grading:
| Grade | Solid Component | Description |
|---|---|---|
| Grade 1 | ≤5% | Well-differentiated |
| Grade 2 | 6-50% | Moderately differentiated |
| Grade 3 | >50% | Poorly differentiated |
- Significant nuclear atypia upgrades tumor by 1 grade
- Serous and clear cell = always high-grade (grading not needed)
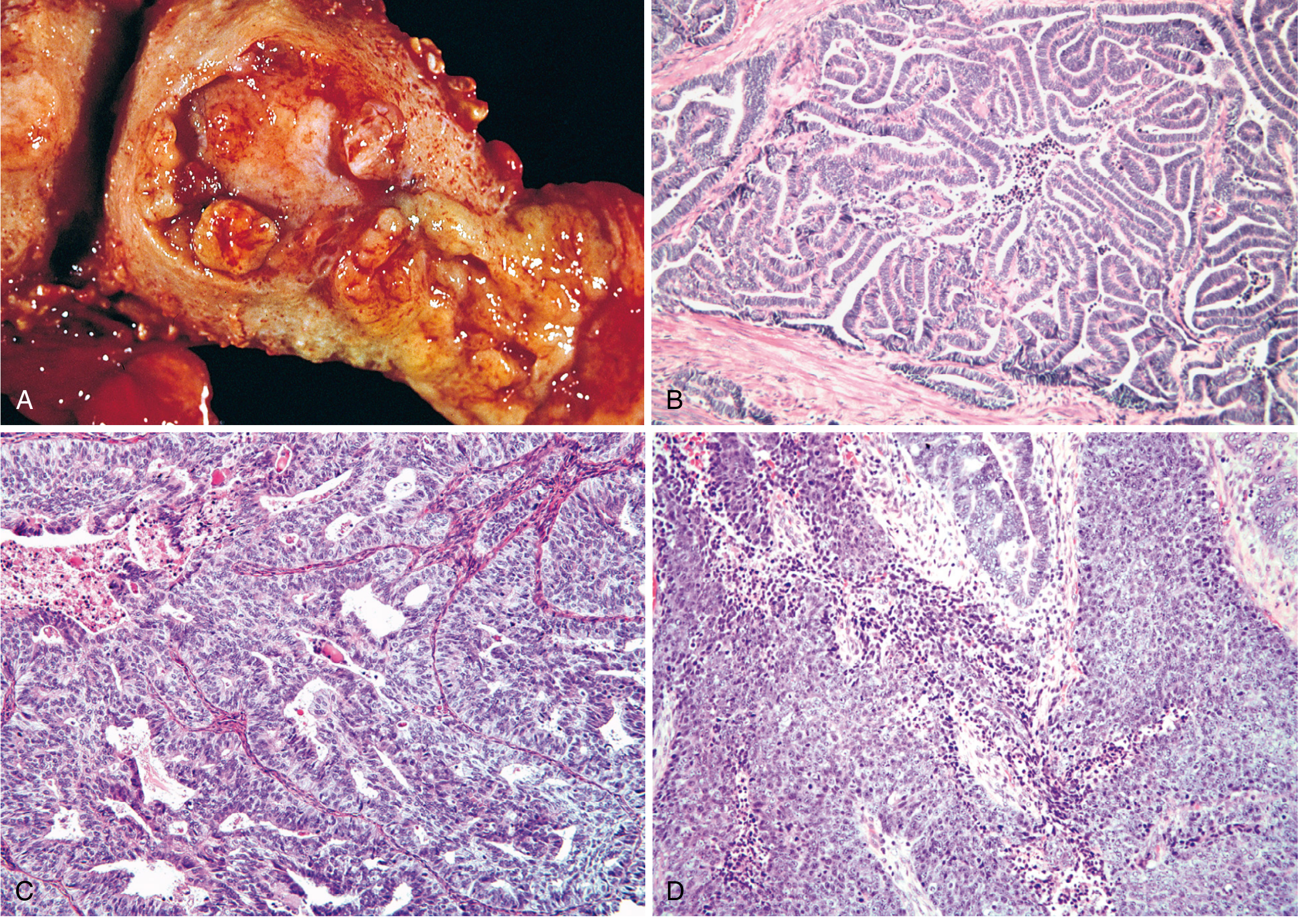
Serous Carcinoma (~10-15%):
- Arises in atrophic endometrium; occurs ~10 years later than endometrioid
- Precursor: Endometrial Intraepithelial Carcinoma (EIC) - malignant cells on surface epithelium only
- Papillary architecture; marked cytologic atypia; TP53 mutated (>90%)
- Spreads via transtubal route to peritoneum despite superficial uterine involvement
- 5-year survival 18-27%; recurrence rate up to 80% even when confined to uterus
- More common in women of African descent (2-fold higher mortality)
Clear Cell Carcinoma (~5%):
- High-grade; postmenopausal
- Clear (glycogen-rich) cytoplasm; distinct cell membranes; prominent nucleoli
- Back-to-back glandular pattern; binucleated and multinucleated forms
7. Clinical Features
Symptoms:
- Postmenopausal uterine bleeding (PMB) - cardinal symptom; present in >90%
- BUT remember: only ~10% of PMB is due to endometrial cancer; most is atrophy (60-80%)
- Perimenopausal: menometrorrhagia, oligomenorrhea, or cycles persisting past usual menopause age
- Watery/blood-stained vaginal discharge (early feature)
- Pyometra in elderly (malodorous discharge)
- Pelvic/lower abdominal pain - late feature
- Bladder/bowel symptoms in advanced disease
Signs:
- Obesity (common)
- Usually normal pelvic examination in early disease
- Uterus may be slightly enlarged or bulky
- Bimanual: assess uterine size and mobility, adnexal masses, parametrial induration, cul-de-sac nodularity
- Check inguinal and supraclavicular lymph nodes
- Assess for hepatomegaly, ascites, omental masses (advanced disease)
8. Diagnosis
1. Endometrial Aspiration Biopsy (First-line, office procedure)
- Sensitivity ~90%; adequate tissue in most cases
- Insufficient tissue or negative but high suspicion → D&C
2. Transvaginal Ultrasound (TVS)
- Endometrial thickness >4-5 mm in postmenopausal women requires biopsy
- Assesses myometrial invasion preoperatively
3. Fractional Curettage (D&C)
- Separate endocervical and endometrial curettings
- Endocervical involvement → Stage II
- Gold standard when office biopsy inconclusive
4. Hysteroscopy + Directed Biopsy
- Better visualization of focal lesions and polyps
5. MRI
- Best for preoperative assessment of myometrial invasion and cervical involvement
6. Papanicolaou Smear
- Inadequate for screening (positive in only ~50% of cases)
9. Pretreatment Evaluation
- History and physical examination - most important; assess comorbidities (DM, HTN, obesity)
- Chest X-ray: Exclude pulmonary metastasis; assess cardiorespiratory status
- ECG, CBC, platelet count, blood group and screen
- Serum CA-125: Elevated in advanced disease; useful for monitoring
- CT abdomen/pelvis: Consider for Type II tumors; assess extrauterine spread
- MRI: Preoperative myometrial invasion assessment
- Cystoscopy, colonoscopy, IVP, barium enema: only if symptoms indicate
- Stage IV disease usually clinically evident from symptoms + examination
10. FIGO Staging (Surgical)
| Stage | Description |
|---|---|
| I | Confined to corpus uteri |
| IA | No or <50% myometrial invasion |
| IB | ≥50% myometrial invasion |
| II | Cervical stromal invasion (not glandular) |
| III | Local/regional spread |
| IIIA | Uterine serosa and/or adnexa |
| IIIB | Vaginal/parametrial involvement |
| IIIC1 | Pelvic lymph node metastasis |
| IIIC2 | Para-aortic lymph node metastasis |
| IV | Beyond true pelvis or mucosal involvement |
| IVA | Bladder/bowel mucosa |
| IVB | Distant metastases (including inguinal LN) |
5-year survival:
- Stage I (grade 1/2): ~90%
- Stage I (grade 3): ~75%
- Stage II/III: ~50%
- Serous carcinoma overall: 18-27%
11. Prognostic Variables
| Factor | Detail |
|---|---|
| Age | Older = worse |
| Histologic type | Serous/clear cell >> endometrioid |
| Histologic grade | Grade 3 significantly worse |
| Myometrial invasion | ≥50% = high lymph node risk |
| LVSI | Independent predictor of recurrence |
| Cervical invasion | Stage II |
| Lymph node metastasis | Most important determinant |
| Tumor size | >2 cm: 15% LN mets; entire cavity: 35% |
| Hormone receptor status | PR+ > ER+ as predictor; receptor-positive = better |
| Peritoneal cytology | Positive = worse outcome |
| DNA ploidy | Aneuploid = worse |
| Molecular subtype | POLE = best; TP53-mutated = worst |
LN metastasis by myometrial invasion depth:
- No invasion: 1%
- Inner 1/3: 5%
- Middle 1/3: 6%
- Outer 1/3: 25%
12. Routes of Spread
- Direct extension - downward to cervix; outward through myometrium to serosa and adnexa
- Lymphatic - to pelvic nodes (obturator, external/internal iliac), then para-aortic nodes
- Hematogenous - lungs (most common), liver, bones, brain
- Transperitoneal - especially serous carcinoma; via tubal regurgitation
- Transcervical - to vagina
13. Treatment
Surgery (Primary Treatment)
Standard: TAH + BSO + peritoneal cytology ± lymph node assessment
Surgical staging includes:
- TAH + BSO
- Peritoneal cytology
- Inspection of all peritoneal surfaces
- Lymph node assessment (sentinel node biopsy or formal dissection)
- Omental biopsy if indicated
Laparoscopic approach (preferred): GOG trial (>2,500 patients) showed:
- Equivalent oncologic outcomes to laparotomy
- Shorter hospital stay (52% vs 94% >2 days)
- Less blood loss and fewer postoperative complications (14% vs 21%)
- Longer operative time; 24% conversion rate (improved to 2.4% with modern technique)
Vaginal hysterectomy: Acceptable for low-risk tumors (grade 1/2, <50% MI, tumor <2 cm) with high surgical risk. 94% survival in selected series.
Lymphadenectomy may be omitted when: grade 1/2 endometrioid + <50% MI + tumor ≤2 cm (negligible lymphatic spread risk)
Sentinel lymph node biopsy: Sensitivity 97.2%, NPV 99.6% - increasingly replacing formal lymphadenectomy
Radiation Therapy
- Vaginal vault brachytherapy: Intermediate-risk; reduces vaginal recurrence
- External pelvic RT (EBRT): Higher-risk; deep invasion or LN metastasis
- Extended-field RT: Para-aortic involvement
- Primary RT: Medically unfit patients
Chemotherapy
- Carboplatin + paclitaxel: Most widely used for advanced/recurrent disease
- Indicated for: Stage III/IV, Type II tumors, recurrence
Hormonal Therapy
- Megestrol acetate 40-160 mg/day - most reliable for reversing hyperplasia and treating receptor-positive recurrent disease
- Progesterone receptor status predicts response
- Fertility-preserving protocol: Continuous progestins + serial biopsy q3-6 months
- ~76% achieve complete response; ~24% never respond
- ~20 patients achieved pregnancy in reviewed series
- Must be counseled: temporary treatment; hysterectomy after childbearing
14. Screening
- No effective population screening exists
- Pap smear: inadequate (insensitive)
- TVS + biopsy: too expensive for routine use
- Lynch II syndrome: Annual pelvic exam + TVS + endometrial biopsy from age 35-40
- Prophylactic hysterectomy + BSO after childbearing = 100% prevention in Lynch II carriers
- Universal MMR IHC testing (MLH1, MSH2, MSH6, PMS2) now recommended for all newly diagnosed endometrial cancers to identify Lynch syndrome
15. Recurrent Disease
Most common site: Vaginal vault
Treatment:
- Vaginal recurrence (if not previously irradiated): radiation therapy
- Pelvic exenteration: selected patients with central pelvic recurrence
- Chemotherapy: carboplatin + paclitaxel for systemic recurrence
- Hormonal therapy: progestins for receptor-positive, slow-growing recurrences
Sources: Berek & Novak's Gynecology; Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.