
IMG_20260605_011950.jpg
Here is a 68 year old female patient came to emergency department with the complain of shortness of breath and palpitation with bp 12186 mmhg with pulse rate being 184 bits per minute and non case of right lower lim elephantiasis kindly diagnose this patient with the help of ECG and give me differential diagnosis
Reading File
Searching the Web
atrial flutter atrial fibrillation rapid ventricular response ECG 184 bpm narrow complex tachycardia elderly female dyspnea
Finding Sources
Finding Sources
Searching PubMed
atrial flutter rapid ventricular response management elderly
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information to give a full, authoritative answer. Here is the complete clinical analysis:
ECG Analysis & Clinical Diagnosis
Patient Summary
- Age/Sex: 68-year-old female
- Complaints: Shortness of breath, palpitations
- Vitals: BP 121/86 mmHg, HR 184 bpm
- Relevant finding: Right lower limb elephantiasis (lymphedema)
- Current medications (visible on pill box): Tab. Carvedilol 3.125 mg, Tab. Nikardia Retard (Nifedipine) 10 mg
ECG Interpretation
The machine has flagged this as a "Markedly Abnormal ECG" with a note about possible axis error due to low voltage.
Systematic ECG Analysis:
| Parameter | Finding |
|---|---|
| Rate | ~184 bpm |
| Rhythm | Appears regular (consistent R-R intervals across all leads) |
| P waves | Not clearly identifiable as discrete, upright P waves - baseline shows a continuous undulating/sawtooth-like pattern |
| QRS morphology | Narrow complex (normal duration, no bundle branch block) |
| QRS axis | Indeterminate/abnormal (machine flagged axis issue) |
| ST/T changes | Non-specific, difficult to assess at this rate |
Primary ECG Diagnosis:
Atrial Flutter with Rapid Ventricular Response (likely 1:1 or near-1:1 conduction)
Reasoning:
- Rate of 184 bpm is very characteristic. Classic atrial flutter has an atrial rate of ~300 bpm. With a 2:1 conduction ratio, the ventricular rate is typically ~150 bpm. With near 1:1 conduction (possible in this patient given she is on Carvedilol at a very low dose of 3.125 mg - a beta-blocker that may not be sufficiently rate-controlling), rates of 180-200 bpm are seen.
- The regular narrow-complex tachycardia is the hallmark of atrial flutter. Compare the textbook example below:
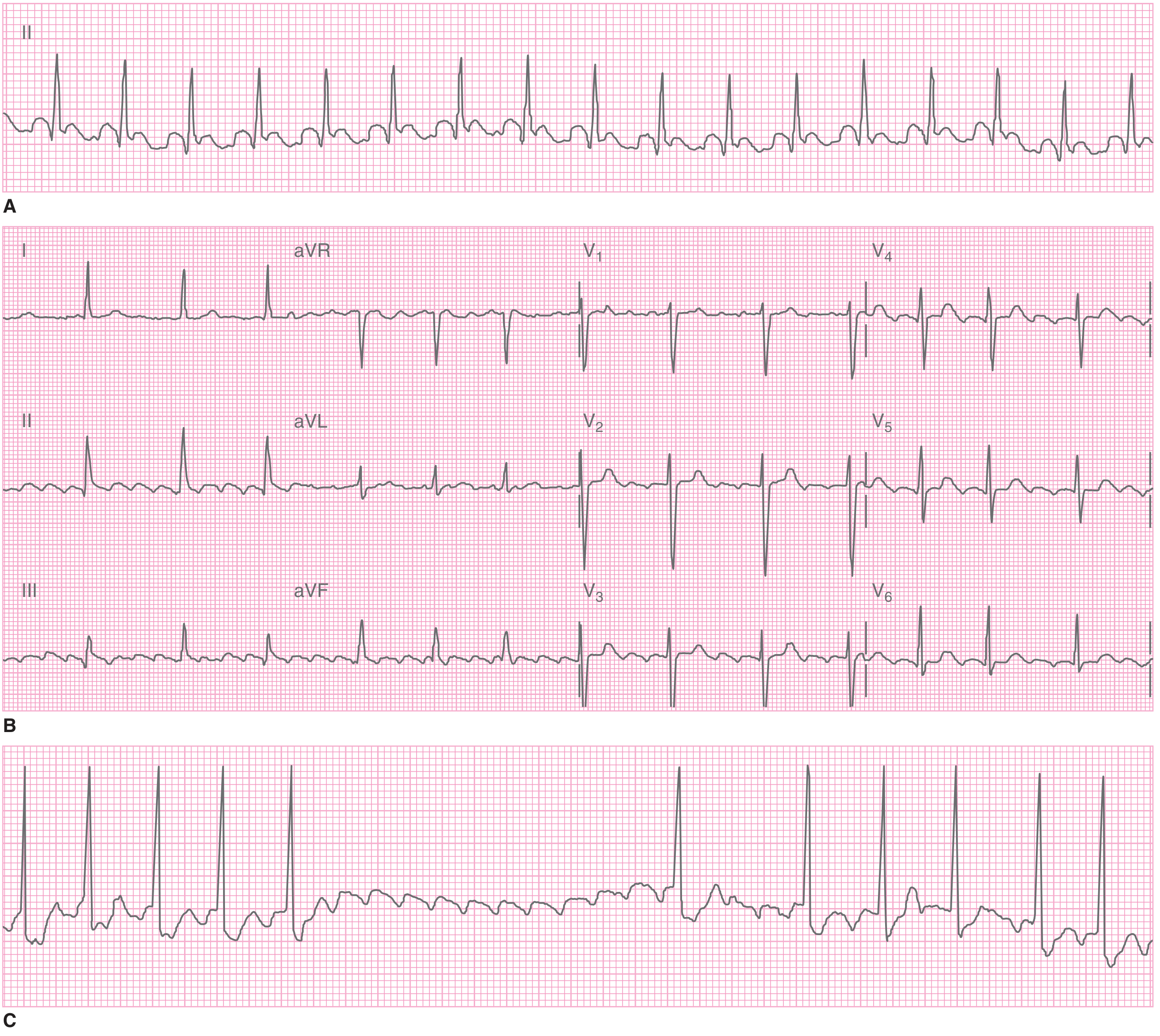
The pattern in the submitted ECG - particularly the undulating baseline between QRS complexes visible in the inferior leads (II, III, aVF) and V1 - is consistent with flutter waves (sawtooth pattern).
An alternative but closely related diagnosis is Atrial Fibrillation with Rapid Ventricular Response (AF with RVR). The key distinction:
- AF → irregularly irregular rhythm, no distinct P waves, chaotic baseline
- Atrial Flutter → regular rhythm, saw-tooth flutter waves, predictable AV conduction ratio
The regularity of the rhythm in this ECG favors atrial flutter over AF, though AF cannot be fully excluded without a cleaner tracing.
Differential Diagnosis
Listed in order of likelihood:
1. Atrial Flutter with Rapid Ventricular Response (Most Likely)
- Regular narrow-complex tachycardia at ~184 bpm
- Sawtooth flutter waves (best seen in II, III, aVF, V1)
- Atrial rate ~300-370 bpm with variable conduction
- Supported by: regular rhythm, rate in typical flutter range
- Tintinalli's EM: "A regular narrow-complex tachycardia at an approximate rate of 150 beats/min (+/- 5 beats/min) strongly suggests atrial flutter with 2:1 conduction." At 184 bpm, this may represent atrial flutter with near-1:1 or between 1:1 and 2:1 conduction.
2. Atrial Fibrillation with Rapid Ventricular Response (AF with RVR)
- Most common supraventricular tachycardia in the ED (after sinus tachycardia)
- No distinct P waves, irregularly irregular rhythm
- Ventricular rate typically 120-170 bpm in uncontrolled AF; rates >200 bpm may suggest an accessory pathway
- Rate of 184 bpm is slightly high for typical AF with RVR but possible
- The distinction is clinically important: both require similar acute management but long-term management differs
3. AV Nodal Reentrant Tachycardia (AVNRT)
- Most common regular narrow-complex tachycardia in adults
- Rates typically 150-250 bpm
- P waves are either absent or retrograde (buried in or just after QRS complex)
- Usually paroxysmal; less commonly sustained at 184 bpm in elderly
- Often triggered by a premature atrial beat
4. Atrioventricular Reentrant Tachycardia (AVRT) / WPW Syndrome
- Uses an accessory pathway (Bundle of Kent)
- Can present as orthodromic AVRT (narrow complex) at 150-250 bpm
- Less likely at age 68 without prior history, but must be considered
- Important: Do NOT give AV nodal blockers (adenosine, diltiazem, digoxin) if pre-excitation is suspected - can precipitate VF
5. Focal Atrial Tachycardia
- Abnormal automaticity from a single atrial focus
- Rates 100-250 bpm, narrow complex
- P wave morphology differs from sinus P waves
- Less common than flutter/AF
6. Sinus Tachycardia with Underlying Cause
- Less likely at 184 bpm - sinus tachycardia rarely exceeds 160-170 bpm even with severe physiological stress
- Would require an underlying cause: PE, sepsis, severe anemia, thyrotoxicosis
7. Pulmonary Embolism-Induced Tachycardia (Important to Exclude)
- The right lower limb elephantiasis/lymphedema is a key clinical clue
- Chronic lymphedema causes venous stasis, which is a major risk factor for DVT/PE
- PE can precipitate both AF and sinus tachycardia
- Classic ECG findings of PE: sinus tachycardia, S1Q3T3, right heart strain, RBBB
- This patient's ECG does not clearly show S1Q3T3, but PE should remain on the differential given the clinical history
Clinical Significance of Right Lower Limb Elephantiasis
The right lower limb elephantiasis is not incidental:
- Chronic lymphedema causes venous stasis - a core component of Virchow's triad for DVT
- DVT + tachycardia + shortness of breath = must rule out Pulmonary Embolism
- PE can itself trigger atrial flutter/AF and cause right heart strain
- Also, lymphedema may indicate underlying lymphatic obstruction from a pelvic/abdominal malignancy, which increases thrombotic risk further
Immediate Management
Step 1 - Hemodynamic Assessment
- BP of 121/86 mmHg is borderline - not severely hypotensive but HR of 184 is concerning
- Assess for signs of hemodynamic instability: altered consciousness, chest pain, severe dyspnea, hypotension
- If hemodynamically unstable → Urgent synchronized DC cardioversion (50-200 J)
Step 2 - Rate Control (if stable)
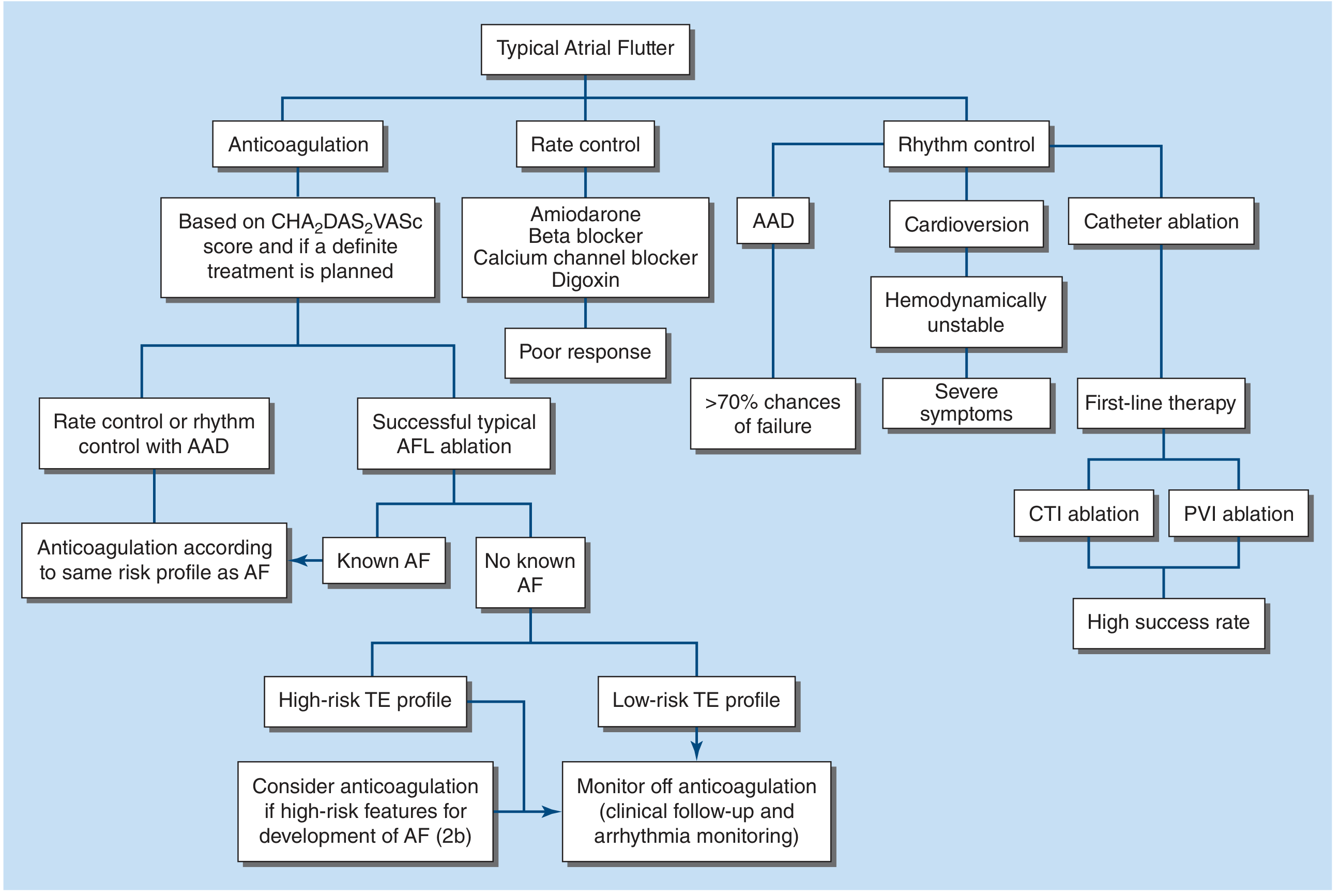
Per the treatment flowchart from Harrison's Principles of Internal Medicine (2025):
For rate control in atrial flutter/AF with RVR:
- IV Metoprolol or IV Diltiazem (first-line AV nodal blocking agents)
- IV Amiodarone (if LV dysfunction is suspected or beta-blockers contraindicated)
- Digoxin (slower onset, less preferred acutely)
- Note: She is already on Carvedilol 3.125 mg - a very low dose, clearly not providing adequate rate control
Step 3 - Anticoagulation
- CHA2DS2-VASc score for this patient:
- Congestive Heart Failure: unknown (possibly 1)
- Hypertension: unknown (possibly 1 - she's on Nifedipine)
- Age 65-74: +1 (she is 68)
- Female sex: +1
- Minimum score = 2 → anticoagulation indicated
- Start DOAC (e.g., Rivaroxaban, Apixaban) or LMWH pending evaluation
Step 4 - Workup to Perform
| Investigation | Reason |
|---|---|
| 12-lead ECG + rhythm strip | Better delineate flutter waves |
| D-dimer / CT Pulmonary Angiography | Rule out PE (given lymphedema + DVT risk) |
| Doppler US of right lower limb | Rule out DVT |
| TFTs (TSH, free T4) | Thyrotoxicosis can cause AF/flutter |
| Echocardiogram | Assess LV function, valvular disease, LA size |
| BMP, CBC, Mg2+, K+ | Electrolyte disturbance triggers arrhythmia |
| Troponin | Rule out acute MI as a trigger |
| CXR | Pulmonary edema, cardiomegaly |
Step 5 - Long-Term Management (if Atrial Flutter confirmed)
- Rate and rhythm control as outlined in the Harrison's flowchart above
- Catheter ablation (CTI ablation) - first-line definitive therapy for atrial flutter, >95% success rate
- Anticoagulation guided by CHA2DS2-VASc score
- Address right leg lymphedema and its underlying cause
Key Diagnosis Summary
Primary diagnosis: Atrial Flutter with Rapid Ventricular Response
- Regular narrow-complex tachycardia at 184 bpm
- ECG labeled "Markedly Abnormal" by the machine
- Consistent with typical (CTI-dependent) atrial flutter
Must not miss: Pulmonary Embolism as a precipitating cause, given the right lower limb elephantiasis, which implies significant venous stasis risk.
Current medications require dose adjustment: Carvedilol 3.125 mg is not providing adequate rate control; dose escalation or substitution with IV rate-controlling agent is indicated acutely.
Sources: Tintinalli's Emergency Medicine (9th ed.), Harrison's Principles of Internal Medicine 22E (2025), Braunwald's Heart Disease (2 Vol. Set)
This is a shared conversation. Sign in to Orris to start your own chat.