Short not on plasma proteins(its values) and their functions and write a short note on A/G ratio for 5 marks
Plasma Proteins - Values and Functions
Normal Values
| Protein Fraction | Normal Value |
|---|---|
| Total plasma protein | 6.0 - 8.0 g/dL |
| Albumin | 3.5 - 5.0 g/dL (~60% of total) |
| Globulins (total) | 2.0 - 3.5 g/dL |
| - α1-globulins | 0.2 - 0.4 g/dL |
| - α2-globulins | 0.5 - 0.9 g/dL |
| - β-globulins | 0.6 - 1.1 g/dL |
| - γ-globulins | 0.7 - 1.7 g/dL |
| Fibrinogen | 0.2 - 0.4 g/dL |
Functions of Plasma Proteins
1. Oncotic (Osmotic) Pressure Maintenance
2. Transport / Carrier Function
- Albumin: carries free fatty acids, bilirubin, calcium, zinc, copper, steroid hormones, and numerous drugs (e.g. penicillin, aspirin, warfarin)
- Transferrin: transports iron
- Ceruloplasmin: transports copper
- Haptoglobin: binds free hemoglobin
- Thyroxine-binding globulin (TBG): transports thyroid hormones
- Transcortin (CBG): transports cortisol and other corticosteroids
- Transthyretin: transports T4 and retinol-binding protein
3. Immune Defense
4. Blood Coagulation
5. Buffering Capacity
6. Acute Phase Response
7. Enzyme Activity
A/G Ratio (Albumin to Globulin Ratio)
Definition
Normal Value
Significance
| Condition | Effect on A/G Ratio |
|---|---|
| Liver disease (cirrhosis, hepatitis) | Decreased (albumin synthesis falls) |
| Nephrotic syndrome | Decreased (urinary albumin loss) |
| Malnutrition / Malabsorption | Decreased (albumin synthesis falls) |
| Multiple myeloma | Reversed (marked globulin rise) |
| Autoimmune hepatitis | Reversed (polyclonal IgG rises) |
| Primary biliary cirrhosis | Reversed (polyclonal IgM rises) |
| Kala-azar (visceral leishmaniasis) | Reversed (greatly increased IgG) |
| Normal / Well-nourished state | >1 |
Why is Reversal Significant?
Note: While the A/G ratio was widely used historically, serum protein electrophoresis (SPEP) is now more informative as it separates the five major fractions (albumin, α1, α2, β, γ) individually and can identify a monoclonal spike in conditions like myeloma.
For mbbs first year
Plasma Proteins - Values, Functions & A/G Ratio
Plasma Proteins - Normal Values
| Fraction | Normal Value |
|---|---|
| Total Plasma Protein | 6.0 - 8.0 g/dL |
| Albumin | 3.5 - 5.0 g/dL |
| Globulins | 2.0 - 3.5 g/dL |
| Fibrinogen | 0.2 - 0.4 g/dL |
- Albumin makes up ~60% of total plasma protein
- Site of synthesis: Liver (except immunoglobulins, which are made by plasma cells/B lymphocytes)
Functions of Plasma Proteins
1. Maintenance of Osmotic (Oncotic) Pressure
2. Transport Function
- Albumin - free fatty acids, bilirubin, Ca²⁺, drugs (aspirin, penicillin, warfarin)
- Transferrin - iron
- Ceruloplasmin - copper
- Haptoglobin - free hemoglobin
- TBG (Thyroxine Binding Globulin) - thyroid hormones
- Transcortin - cortisol
3. Role in Blood Coagulation
4. Immune Defense
5. Buffer Action
6. Acute Phase Proteins
A/G Ratio (Albumin : Globulin Ratio)
Globulin = Total protein - Albumin A/G ratio = Albumin ÷ Globulin
Clinical Significance
| Condition | Change in A/G ratio |
|---|---|
| Liver cirrhosis / hepatitis | Decreased |
| Nephrotic syndrome | Decreased (albumin lost in urine) |
| Protein malnutrition (Kwashiorkor) | Decreased |
| Multiple myeloma | Reversed (massive globulin rise) |
| Kala-azar | Reversed |
| Autoimmune hepatitis | Reversed |
Why is it useful?
Remember: Normal = A > G. Reversed = G > A (pathological).
- Total protein = 6-8 g/dL; Albumin = 3.5-5 g/dL
- Albumin = main osmotic protein + main transport protein
- A/G ratio normal = 1.2-1.8; reversed in liver disease, nephrotic syndrome, myeloma
- Fibrinogen is removed in serum (so serum has no fibrinogen; plasma does)
Immunoglobulins structure types and functions 5 marks mbbs
Immunoglobulins - Structure, Types and Functions
Definition
Basic Structure of Immunoglobulin (IgG as prototype)
Chains
- 2 Heavy (H) chains - larger (~50-70 kDa each)
- 2 Light (L) chains - smaller (~23 kDa each)
- Held together by inter-chain disulfide bonds (-S-S-) and non-covalent forces
Regions on each chain
- Variable (V) region - N-terminal end; differs between antibodies; forms the antigen-binding site
- Constant (C) region - C-terminal end; same within a class; determines effector functions
Light Chains
- A single Ig molecule always has either 2κ or 2λ, never mixed
- In humans, κ chains predominate
Heavy Chains
| Class | Heavy chain |
|---|---|
| IgG | γ (gamma) |
| IgA | α (alpha) |
| IgM | μ (mu) |
| IgD | δ (delta) |
| IgE | ε (epsilon) |
Functional Fragments (Proteolytic Cleavage)
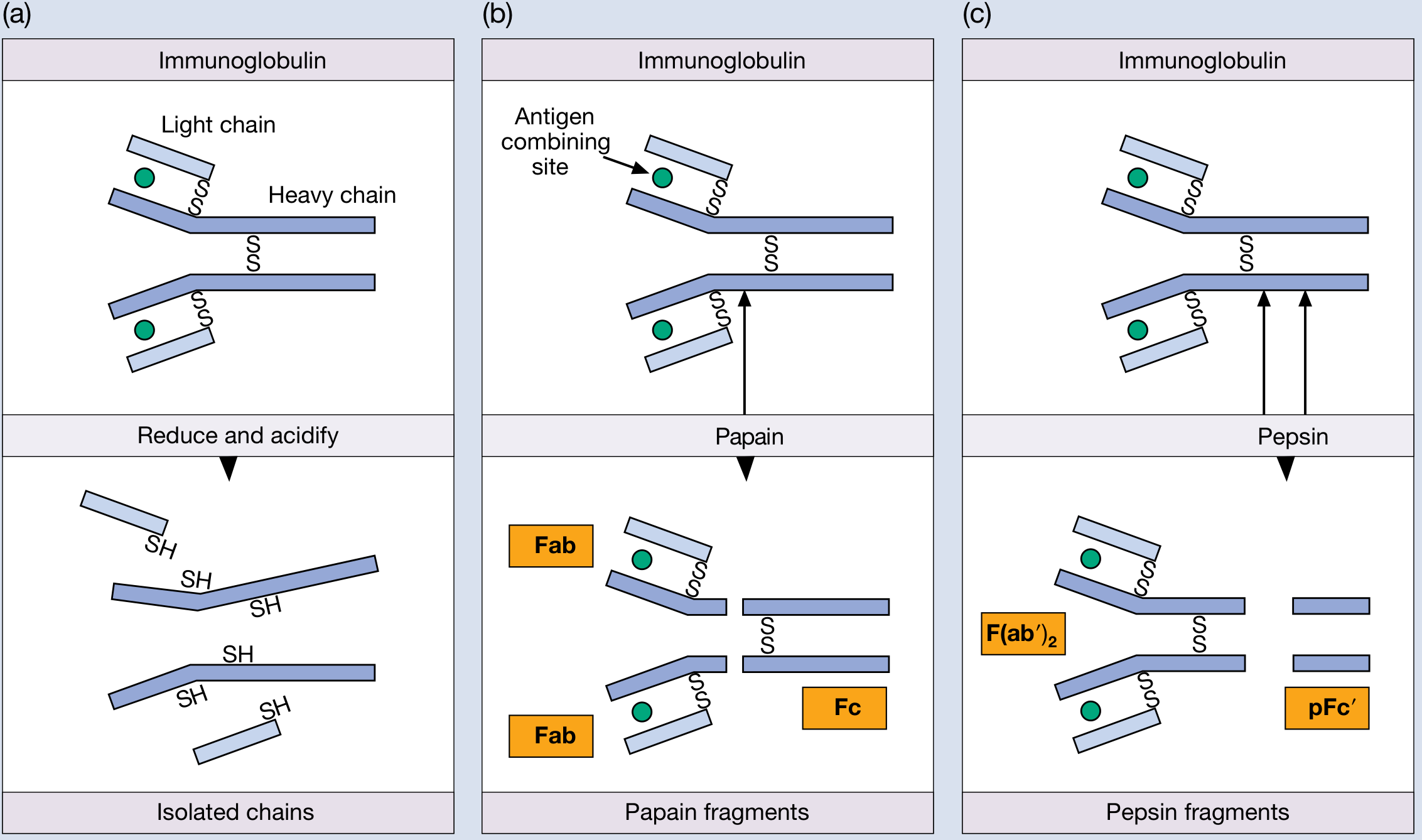
| Enzyme | Fragments Produced |
|---|---|
| Papain | 2 × Fab (Fragment Antigen Binding - each monovalent) + 1 × Fc (Fragment Crystallizable) |
| Pepsin | 1 × F(ab')₂ (bivalent, still precipitates antigen) + pFc' (degraded) |
- Fab - contains VH + VL + CH1 + CL; binds antigen
- Fc - contains CH2 + CH3; mediates effector functions (complement, opsonization, placental transfer)
- Hinge region - between CH1 and CH2; flexible; susceptible to proteases
Types of Immunoglobulins and Their Properties
| Property | IgG | IgA | IgM | IgD | IgE |
|---|---|---|---|---|---|
| % of total Ig | 75% | 15% | 9% | 0.2% | 0.004% |
| Serum conc. | ~1000 mg/dL | ~200 mg/dL | ~120 mg/dL | ~3 mg/dL | ~0.05 mg/dL |
| Structure | Monomer | Monomer/Dimer | Pentamer | Monomer | Monomer |
| Mol. weight | 150 kDa | 170/400 kDa | 900 kDa | 180 kDa | 190 kDa |
| Sedimentation | 7S | 7S or 11S | 19S | 7S | 8S |
Functions of Each Class
IgG (most abundant)
- Main antibody of secondary immune response
- Crosses the placenta - provides passive immunity to the newborn
- Opsonization - coats bacteria to enhance phagocytosis
- Complement activation (classical pathway) - IgG1 and IgG3 most effective
- Neutralization of toxins and viruses
- Has 4 subclasses: IgG1, IgG2, IgG3, IgG4
IgA
- Found in secretions (saliva, tears, breast milk, gut, respiratory mucosa) as secretory IgA (sIgA)
- Dimer in secretions, joined by J chain + secretory component (SC)
- First line of mucosal defense against pathogens
- Protects mucosal surfaces (GIT, respiratory tract)
IgM
- First antibody produced in primary immune response (earliest response)
- Pentameric structure - 10 antigen binding sites (highest avidity)
- Most efficient at complement activation
- Antigen receptor on naive B cells (as surface monomer)
- Responsible for ABO blood group agglutination (isohemagglutinins)
- Contains J chain linking the 5 monomers
IgD
- Found mainly on the surface of B lymphocytes as antigen receptor (along with IgM)
- Very low serum levels
- Role in lymphocyte activation and regulation
- May protect against upper respiratory tract microbes
IgE
- Present in extremely low concentrations in serum
- Most IgE is bound to mast cells and basophils via high-affinity Fc receptors (FcεRI)
- When antigen (allergen) cross-links IgE on mast cells → degranulation → histamine release
- Mediates Type I hypersensitivity (allergic reactions) - anaphylaxis, asthma, urticaria
- Plays a role in defense against helminth (worm) infections
Key Points to Remember
| Feature | Remember |
|---|---|
| Most abundant | IgG (75%) |
| First in infection | IgM |
| Crosses placenta | IgG only |
| Found in secretions | IgA |
| Allergy/anaphylaxis | IgE |
| B cell receptor | IgM and IgD |
| Pentamer | IgM |
| Highest avidity | IgM (10 binding sites) |
Mention functions and types
Immunoglobulins - Types and Functions
Types of Immunoglobulins (5 Classes)
| Class | Heavy Chain | Structure | % in Serum |
|---|---|---|---|
| IgG | γ (gamma) | Monomer | 75% |
| IgA | α (alpha) | Monomer / Dimer | 15% |
| IgM | μ (mu) | Pentamer | 9% |
| IgD | δ (delta) | Monomer | 0.2% |
| IgE | ε (epsilon) | Monomer | 0.004% |
Light chains are of 2 types: Kappa (κ) and Lambda (λ) - same in all classes.
Functions of Each Type
IgG
- Main antibody of secondary (anamnestic) immune response
- Only Ig that crosses the placenta - provides passive immunity to newborn
- Opsonization - coats bacteria, enhances phagocytosis
- Complement activation (classical pathway)
- Neutralizes toxins and viruses
- Has 4 subclasses: IgG1, IgG2, IgG3, IgG4
IgA
- Mucosal/secretory immunity - main Ig in saliva, tears, breast milk, colostrum, respiratory and GI secretions
- In secretions, exists as dimer joined by J chain + secretory component (SC)
- First line of defense at mucosal surfaces
- Protects gut and respiratory tract from pathogen entry
IgM
- First antibody produced in primary immune response (earliest to appear)
- Pentameric - has 10 antigen binding sites (highest avidity of all Ig)
- Most potent activator of complement (classical pathway)
- Acts as antigen receptor on naive B cells (as surface monomer)
- Responsible for ABO blood group agglutination (natural isohemagglutinins)
IgD
- Found mainly on surface of mature B lymphocytes as antigen receptor (co-expressed with IgM)
- Involved in B cell activation and regulation
- Very low serum levels - exact serum function not fully clear
- May have a role in defense against upper respiratory infections
IgE
- Mediates Type I (immediate) hypersensitivity reactions - allergy, asthma, anaphylaxis, urticaria
- Binds to mast cells and basophils via high-affinity Fc receptors (FcεRI)
- When allergen cross-links IgE → mast cell degranulation → histamine, leukotrienes released
- Plays a protective role in helminth (parasitic worm) infections
- Lowest serum concentration but most potent in allergic reactions
Quick Memory Table
| Ig | Key Function - One Line |
|---|---|
| IgG | Most abundant; crosses placenta; opsonization |
| IgA | Secretory; mucosal protection |
| IgM | First responder; strongest complement activator; pentamer |
| IgD | B cell surface receptor; lymphocyte regulation |
| IgE | Allergy and anaphylaxis; anti-helminth |
G A M D E → "Go And Meet Doctor Edelman"
Structure of insulin and its maturation
Structure of Insulin and Its Maturation
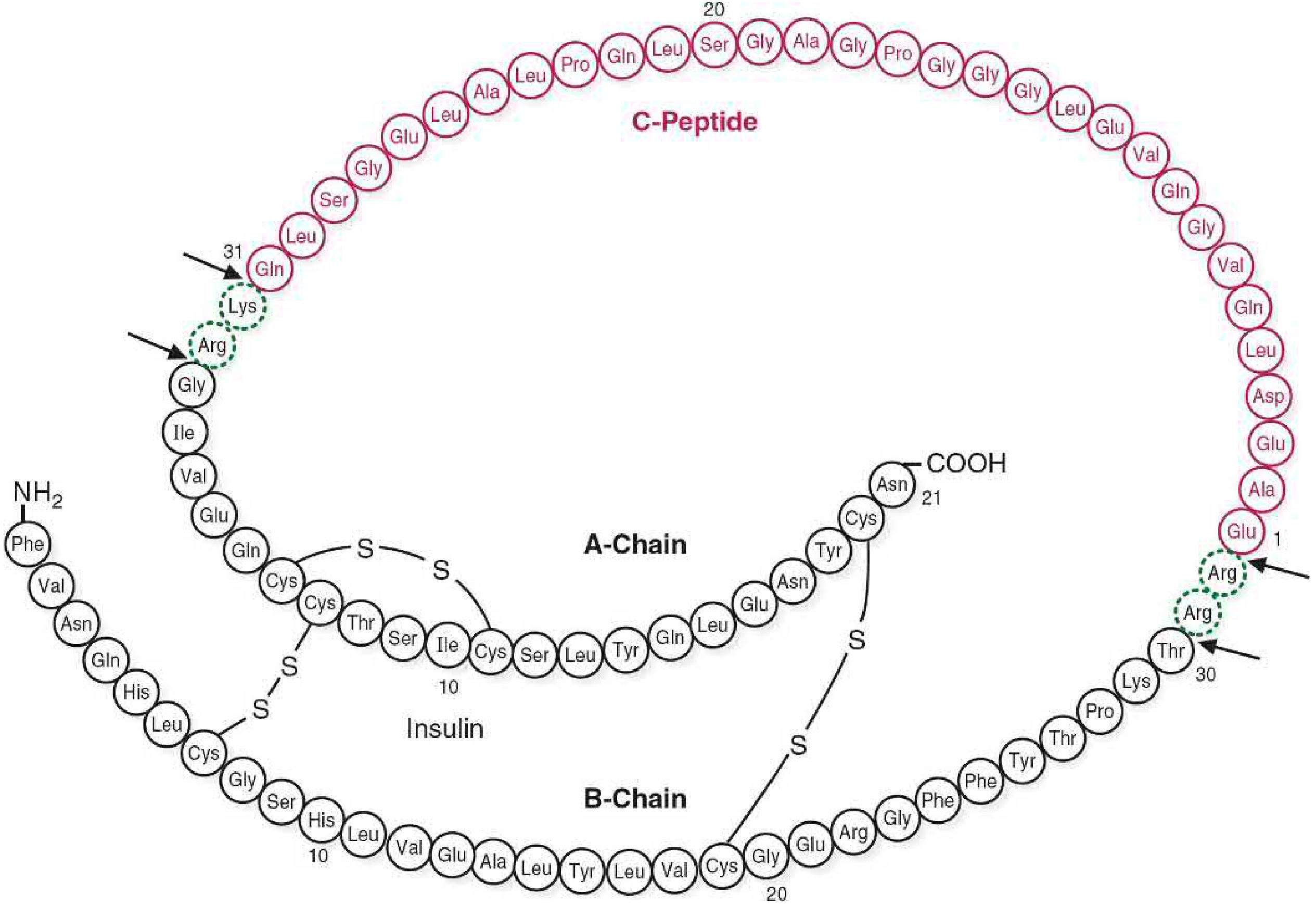
Structure of Insulin
Chains
| Feature | Detail |
|---|---|
| A chain | 21 amino acids |
| B chain | 30 amino acids |
| Total | 51 amino acids, mol. wt ~5808 Da |
| Gene location | Short arm of chromosome 11 |
Disulfide Bonds (3 total)
- 2 interchain disulfide bonds - link A chain to B chain (at A7-B7 and A20-B19)
- 1 intrachain disulfide bond - within the A chain itself (at A6-A11)
These disulfide bonds are essential for the correct 3D shape and biological activity of insulin.
Maturation (Biosynthesis) of Insulin
Step-by-Step Maturation
Gene (Chromosome 11)
↓ Transcription + Translation on ribosomes of RER
PREPROINSULIN (110 amino acids)
↓ Signal peptide cleaved in RER lumen
PROINSULIN (86 amino acids)
↓ Disulfide bonds form → correct folding
↓ Transferred to Golgi → packaged into secretory granules
↓ Proteases cleave C-peptide (+ 2 dipeptides)
ACTIVE INSULIN (51 amino acids) + C-PEPTIDE
↓ Exocytosis (triggered by ↑ blood glucose)
BLOODSTREAM
1. Preproinsulin
- First product of translation on RER ribosomes
- Contains: Signal peptide (24 aa) + B chain + C peptide + A chain
- The hydrophobic signal peptide directs the polypeptide into the lumen of the RER and is immediately cleaved off
2. Proinsulin
- Formed after signal peptide removal (86 amino acids)
- Folds into correct conformation in the RER
- 3 disulfide bonds form between cysteine residues
- Transferred to Golgi apparatus → packaged into secretory granules
- Biologically inactive
3. Active Insulin + C-Peptide
- Inside secretory granules, two proteases (Prohormone convertase 1 and 2) cleave the C-peptide (connecting peptide, 31 amino acids) + 2 small dipeptides
- Result: Active insulin (A + B chains held by disulfide bonds) + C-peptide
- Released in equimolar amounts by exocytosis
- Zinc ions co-precipitate with insulin in granules → form hexameric zinc-insulin crystals for storage
Clinical Significance of C-Peptide
| Point | Detail |
|---|---|
| Released equimolar with insulin | Yes - 1:1 ratio |
| Present in exogenous (injected) insulin? | No - commercial insulin has no C-peptide |
| Use | Measures endogenous β-cell function in diabetics receiving insulin injections |
| Half-life | Longer than insulin (~30 min vs ~5 min) |
C-peptide measurement is used to distinguish Type 1 DM (low/absent C-peptide) from Type 2 DM (normal/high C-peptide) and to detect insulinoma.
Summary Table
| Precursor | Location | What happens |
|---|---|---|
| Preproinsulin | RER (ribosomes) | Signal peptide cleaved |
| Proinsulin | RER → Golgi | Disulfide bonds form; folding |
| Active Insulin | Secretory granules | C-peptide removed by proteases |
| Secretion | Plasma membrane | Exocytosis triggered by ↑ glucose |
- A chain = 21 aa; B chain = 30 aa; Total = 51 aa
- 3 disulfide bonds (2 interchain, 1 intrachain)
- Order: Preproinsulin → Proinsulin → Insulin
- C-peptide is released equimolar with insulin
- Gene on chromosome 11
- Half-life of insulin in circulation = ~5 minutes
Describe the biosynthesis of heme and regulation of heme synthesis 15 marks
Biosynthesis of Heme and Its Regulation
Introduction
- Bone marrow (erythroid cells) - ~85% of total heme synthesis (for hemoglobin)
- Liver - ~15% (for cytochrome P450 enzymes)
- Succinyl-CoA (from TCA cycle)
- Glycine (non-essential amino acid)
- Iron (Fe²⁺)
- Pyridoxal phosphate (Vitamin B₆) - coenzyme
Steps of Heme Biosynthesis
MITOCHONDRIA - Step 1
Succinyl-CoA + Glycine → δ-ALA + CO₂ + CoA
- Enzyme: ALA synthase (ALAS) - two isoforms:
- ALAS1 - ubiquitous (all tissues, especially liver)
- ALAS2 - erythroid specific
- Coenzyme: Pyridoxal phosphate (PLP/Vitamin B₆)
- Location: Mitochondria
- This is the committed, rate-limiting step of heme synthesis
- Two molecules of ALA are produced per cycle
CYTOSOL - Steps 2 to 5
2 ALA → Porphobilinogen (PBG) + 2 H₂O
- Enzyme: ALA dehydratase (ALAD) / PBG synthase
- Cofactor: Zinc (Zn²⁺) at active site
- Inhibited by lead (Pb²⁺) - basis of lead poisoning anemia
- Location: Cytosol
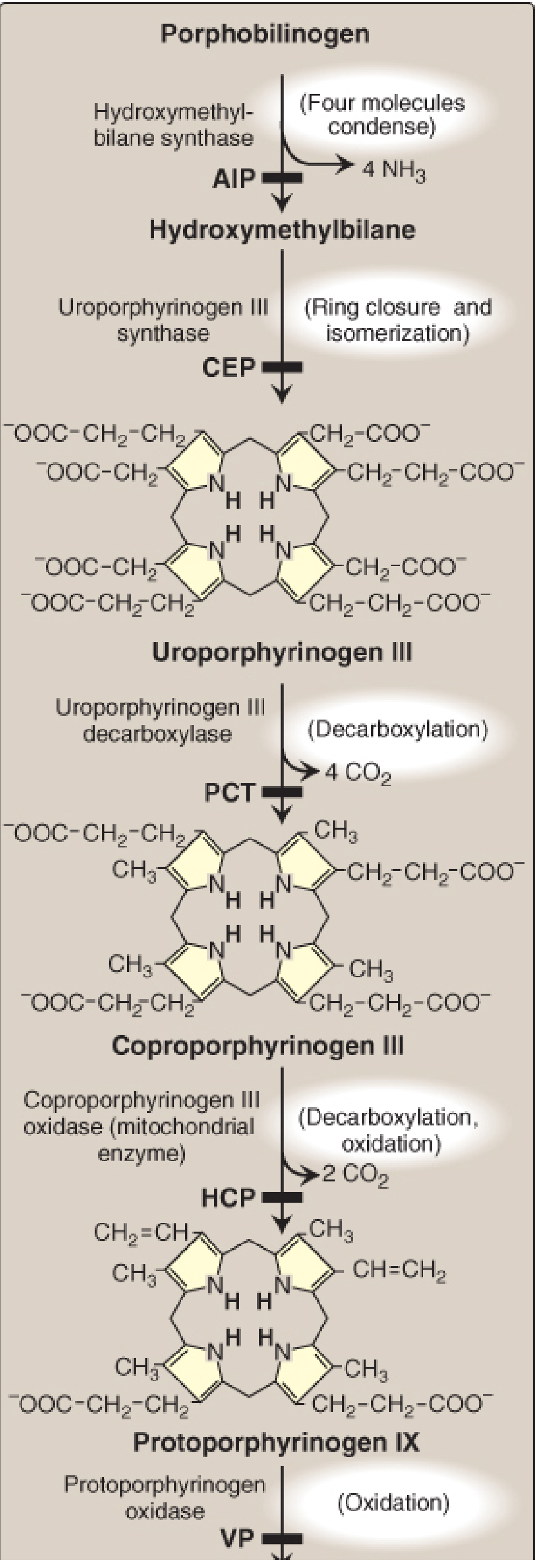
4 PBG → Hydroxymethylbilane + 4 NH₃
- Enzyme: Hydroxymethylbilane synthase (HMBS) / PBG deaminase
- 4 PBG units condense to form a linear tetrapyrrole
- Deficiency → Acute Intermittent Porphyria (AIP)
- Location: Cytosol
Hydroxymethylbilane → Uroporphyrinogen III
- Enzyme: Uroporphyrinogen III synthase (UROS)
- Ring closure and isomerization occurs
- Deficiency → Congenital Erythropoietic Porphyria (CEP)
- Location: Cytosol
Uroporphyrinogen III → Coproporphyrinogen III + 4 CO₂
- Enzyme: Uroporphyrinogen III decarboxylase (UROD)
- Four acetate side chains are decarboxylated to methyl groups
- Deficiency → Porphyria Cutanea Tarda (PCT) - most common porphyria
- Location: Cytosol
Back to MITOCHONDRIA - Steps 6 to 8
Coproporphyrinogen III → Protoporphyrinogen IX + 2 CO₂
- Enzyme: Coproporphyrinogen III oxidase (CPOX)
- Two propionate side chains are decarboxylated and oxidized to vinyl groups
- Deficiency → Hereditary Coproporphyria (HCP)
- Location: Mitochondria
Protoporphyrinogen IX → Protoporphyrin IX
- Enzyme: Protoporphyrinogen oxidase (PPOX)
- Oxidation (removes 6 hydrogen atoms)
- Deficiency → Variegate Porphyria (VP)
- Location: Inner mitochondrial membrane
Protoporphyrin IX + Fe²⁺ → HEME + 2H⁺
- Enzyme: Ferrochelatase (FECH) / Heme synthase
- Ferrous iron (Fe²⁺) is inserted into protoporphyrin IX
- Also inhibited by lead (Pb²⁺)
- Deficiency → Erythropoietic Protoporphyria (EPP)
- Location: Inner mitochondrial membrane
Summary Pathway Diagram
Summary Table of All 8 Steps
| Step | Substrate | Product | Enzyme | Location | Deficiency/Porphyria |
|---|---|---|---|---|---|
| 1 | Succinyl-CoA + Glycine | δ-ALA | ALA synthase (ALAS) | Mitochondria | - (rate-limiting step) |
| 2 | 2 × ALA | PBG | ALA dehydratase | Cytosol | Lead poisoning |
| 3 | 4 × PBG | Hydroxymethylbilane | HMB synthase | Cytosol | AIP |
| 4 | Hydroxymethylbilane | Uroporphyrinogen III | UPG III synthase | Cytosol | CEP |
| 5 | Uroporphyrinogen III | Coproporphyrinogen III | UPG decarboxylase | Cytosol | PCT |
| 6 | Coproporphyrinogen III | Protoporphyrinogen IX | CPG oxidase | Mitochondria | HCP |
| 7 | Protoporphyrinogen IX | Protoporphyrin IX | PPG oxidase | Mitochondria | VP |
| 8 | Protoporphyrin IX + Fe²⁺ | HEME | Ferrochelatase | Mitochondria | EPP |
Memory aid for location: Steps 1, 6, 7, 8 in Mitochondria; Steps 2, 3, 4, 5 in Cytosol "Mito-Cyto-Cyto-Cyto-Cyto-Mito-Mito-Mito" → 1 M, 4 C, 3 M
Regulation of Heme Synthesis
1. Negative Feedback by Heme (Hemin)
| Mechanism | Effect |
|---|---|
| Represses transcription of ALAS1 gene | Less enzyme made |
| Destabilizes ALAS1 mRNA | Less translation |
| Blocks import of pre-ALAS1 into mitochondria | Less enzyme at site of action |
| Increases proteolytic degradation of ALAS1 | More enzyme destroyed |
Net result: ↑ Heme → ↓ ALAS1 → ↓ ALA synthesis → ↓ Heme production
2. Induction by Drugs (in Liver)
Drugs → ↑ CYP synthesis → ↑ Heme consumption → ↓ Free heme → ↑ ALAS1 → ↑ ALA → ↑ Heme synthesis
3. Nutritional Regulation (PGC-1α)
- ALAS1 activity is regulated by the transcriptional co-activator PGC-1α
- This links the rate of hepatic heme synthesis to nutritional and energy status
- Fasting increases PGC-1α → increases ALAS1
4. Erythroid Regulation (ALAS2 - Iron Dependent)
- Iron regulatory proteins (IRP) bind to an iron-responsive element (IRE) in the 5' UTR of ALAS2 mRNA
- When iron is deficient → IRP binds IRE → blocks translation of ALAS2 → ↓ ALA synthesis
- When iron is abundant → IRP does not bind → ALAS2 is freely translated → ↑ Heme synthesis
This ensures heme is only made in erythroid cells when sufficient iron is available for insertion into protoporphyrin IX.
5. Regulation by Heme of Globin Synthesis
Clinically Important Inhibitors of Heme Synthesis
| Inhibitor | Enzymes Inhibited | Effect |
|---|---|---|
| Lead (Pb²⁺) | ALA dehydratase + Ferrochelatase | Anemia + ↑ ALA + ↑ zinc protoporphyrin in RBCs |
| Vitamin B₆ deficiency | ALA synthase (needs PLP) | ↓ ALA synthesis → microcytic, hypochromic anemia with iron overload |
| Iron deficiency | Ferrochelatase (no Fe²⁺ substrate) | ↓ Heme → anemia |
Key Points to Remember
- 8 enzymes involved; first step is rate-limiting
- Starts and ends in mitochondria (steps 1 and 6, 7, 8)
- Steps 2-5 in cytosol
- Precursors: Succinyl-CoA + Glycine; coenzyme: Pyridoxal phosphate
- ALA synthase (ALAS1) is the key regulatory enzyme
- Heme = negative feedback regulator of ALAS1
- Lead inhibits step 2 (ALAD) and step 8 (ferrochelatase)
- Each enzyme deficiency causes a specific porphyria
- AIP (step 3 deficiency) is the most common acute porphyria - precipitated by drugs, fasting, hormones
Explain lead poisoning effects on heme synthesis (5 marks(3+5) marks
What are porphyria’s classify and write in detail about acute intermittent porphyria (3+5) marks
QUESTION 1: Lead Poisoning - Effects on Heme Synthesis
Lead Poisoning - Overview (3 marks)
Mechanism of Inhibition
Enzymes Inhibited
- Normally uses Zn²⁺ as cofactor
- Lead displaces Zn²⁺ → enzyme inactivated
- Result: δ-ALA accumulates (cannot form PBG)
- Catalyzes insertion of Fe²⁺ into protoporphyrin IX → Heme
- Lead inhibits by complexing with -SH groups
- Result: Protoporphyrin IX accumulates; Fe²⁺ is replaced by Zn²⁺ to form zinc protoporphyrin (ZPP) instead of heme
Biochemical Consequences (5 marks)
| Accumulated Substance | Site of Block | Test Significance |
|---|---|---|
| ↑ δ-ALA in urine | Step 2 blocked | Diagnostic marker |
| ↑ Porphobilinogen (mild) | Step 2 blocked | Detected in urine |
| ↑ Protoporphyrin IX in RBCs | Step 8 blocked | Key test |
| ↑ Zinc protoporphyrin (ZPP) | Zn²⁺ substitutes for Fe²⁺ | Sensitive screening test |
| ↑ Coproporphyrin III in urine | Back-accumulation | Detected in urine |
| ↓ Heme | Both steps blocked | Core defect |
Clinical Effects of Lead Poisoning
- ↓ Heme → ↓ Hemoglobin → anemia
- RBCs are small and pale
- Elevated δ-ALA is neurotoxic (structurally similar to GABA)
- Developmental delay, learning disabilities, low IQ (especially in children)
- Encephalopathy (in severe poisoning)
- Abdominal pain, constipation, colic
- ↓ Heme → ↓ Cytochromes → impaired mitochondrial respiration → fatigue
- Lead inhibits 5'-nucleotidase → ribosomal RNA accumulates in RBCs → seen as blue stippling on blood smear (characteristic finding)
Diagnostic Tests
- ↑ Blood lead levels (>10 µg/dL in children)
- ↑ Urinary δ-ALA and coproporphyrin III
- ↑ Zinc protoporphyrin (ZPP) in RBCs - most sensitive screening test
- Blood smear: basophilic stippling
- X-ray: dense "lead lines" at metaphysis of long bones in children
Treatment
- Remove source of exposure
- Chelation therapy: Succimer (DMSA) or CaNa₂-EDTA for blood lead >45 µg/dL
QUESTION 2: Porphyrias - Classification and Acute Intermittent Porphyria
What are Porphyrias? (Definition)
Classification of Porphyrias (3 Marks)
A. By Site of Primary Enzyme Defect
| Type | Primary Organ Affected | Examples |
|---|---|---|
| Hepatic Porphyrias | Liver | AIP, PCT, VP, HCP, ALADP |
| Erythropoietic Porphyrias | Bone marrow | CEP, EPP |
B. By Clinical Features
| Type | Predominant Symptoms | Examples |
|---|---|---|
| Acute Porphyrias | Neuropsychiatric + abdominal | AIP, VP, HCP, ALADP |
| Cutaneous Porphyrias | Photosensitivity/skin blisters | PCT, CEP, EPP |
| Mixed (both) | Both neuro + skin | VP, HCP |
Summary of All Porphyrias
| # | Enzyme Deficient | Porphyria | Class | Features |
|---|---|---|---|---|
| 1 | ALAS2 | X-linked sideroblastic anemia | Erythropoietic | Anemia |
| 2 | ALA dehydratase | ALADP | Hepatic/Acute | Abdominal pain, neuro |
| 3 | HMB synthase (PBG deaminase) | AIP | Hepatic/Acute | Abdominal, neuro |
| 4 | UPG III synthase | CEP (Congenital EP) | Erythropoietic | Severe photosensitivity |
| 5 | UPG decarboxylase | PCT | Hepatic/Cutaneous | Skin blisters, most common |
| 6 | CPG oxidase | HCP | Hepatic/Mixed | Abdominal + skin |
| 7 | PPG oxidase | VP (Variegate Porphyria) | Hepatic/Mixed | Abdominal + skin |
| 8 | Ferrochelatase | EPP | Erythropoietic | Photosensitivity |
Most common porphyria overall: PCT (Porphyria Cutanea Tarda) Most common acute porphyria: AIP (Acute Intermittent Porphyria)
Acute Intermittent Porphyria (AIP) in Detail (5 Marks)
Definition
Genetics
- Inheritance: Autosomal dominant (heterozygous)
- Gene: HMBS gene on chromosome 11q23.3
- Penetrance: Low - only ~10-20% of carriers develop symptoms
- Gender: Strong female predominance (attacks often triggered by hormonal changes)
-
550 mutations identified in HMBS gene
Biochemical Defect
PBG → [HMB synthase - DEFICIENT] → Hydroxymethylbilane
Result: PBG and δ-ALA accumulate ↑↑↑
- Accumulated PBG and δ-ALA are neurotoxic → cause all clinical features
Precipitating (Triggering) Factors
| Category | Examples |
|---|---|
| Drugs (most common) | Barbiturates, phenytoin, sulfonamides, griseofulvin, rifampicin, OCP |
| Hormones | Progesterone (attacks in luteal phase of menstrual cycle) |
| Fasting / Low carbohydrate diet | ↑ PGC-1α → ↑ ALAS1 |
| Alcohol | Induces CYP → depletes heme |
| Stress / Infection | ↑ Heme demand |
| Surgery | Stress response |
Clinical Features (The Classic Triad)
- Severe, colicky, diffuse
- With nausea, vomiting, constipation
- May mimic "surgical abdomen" - patients often misdiagnosed and operated on
- Anxiety, confusion, hallucinations, psychosis
- Peripheral neuropathy (motor > sensory) - can lead to ascending paralysis
- Seizures (avoid phenytoin/barbiturates - they worsen the attack!)
- Autonomic instability: tachycardia, hypertension
- PBG is colorless when first voided
- On standing, PBG oxidizes to porphobilin → urine turns red/dark brown/black
- Classic diagnostic sign
No photosensitivity - this distinguishes AIP from cutaneous porphyrias
Laboratory Findings
| Test | Finding |
|---|---|
| Urine PBG (during attack) | ↑↑ Markedly elevated - KEY diagnostic test |
| Urine δ-ALA | ↑↑ Elevated |
| Urine porphyrins | ↑ Uroporphyrin and coproporphyrin |
| Watson-Schwartz test | Positive (pink-red color with Ehrlich's reagent) |
| RBC HMB-synthase activity | ↓ (~50% of normal) |
| Heme in blood | Normal (since 50% enzyme activity is adequate at rest) |
Watson-Schwartz Test
Treatment
- Remove precipitating factors (stop offending drugs, treat infections)
- High carbohydrate loading (IV glucose 300-400 g/day) - suppresses ALAS1 via insulin signaling
- IV Hemin (Hematin/Heme arginate) - drug of choice for severe attacks
- Provides exogenous heme → inhibits ALAS1 by negative feedback → ↓ ALA and PBG
- Dose: 3-4 mg/kg/day × 4 days
- Symptom control: narcotic analgesics (pain), phenothiazines (nausea), benzodiazepines (anxiety)
- Givosiran (siRNA) - new therapy (FDA approved 2019) - silences ALAS1 mRNA → prevents attacks
- Avoid known triggers
- GnRH analogue (for menstrual cycle-related attacks)
- High carbohydrate diet
Complications
- Hypertension
- Chronic kidney disease (up to 59% of symptomatic patients)
- Hepatocellular carcinoma risk (regular liver imaging every 6 months recommended)
- Residual motor neuropathy
Key One-Liners for AIP
| Feature | Detail |
|---|---|
| Enzyme deficient | HMB synthase (PBG deaminase) |
| Inheritance | Autosomal dominant |
| Key metabolites ↑ | PBG and δ-ALA |
| Key diagnostic test | Urine PBG ↑↑ |
| Bedside test | Watson-Schwartz test |
| Classic symptom | Abdominal pain + dark urine |
| What's absent | No photosensitivity |
| Drug of choice | IV Hemin |
| Most common trigger | Drugs (barbiturates, phenytoin) |
Try again
Enumerate hemoglobin derivatives
Hemoglobin Derivatives
Classification
| Category | Derivatives |
|---|---|
| Physiological (Normal) | Oxyhemoglobin, Deoxyhemoglobin, Carbaminohemoglobin, HbA1c |
| Abnormal/Toxic (Dyshemoglobins) | Methemoglobin, Carboxyhemoglobin, Sulfhemoglobin, Cyanmethemoglobin |
| Laboratory | Cyanmethemoglobin (Drabkin's solution) |
1. Oxyhemoglobin (HbO₂)
- Formed when O₂ binds to Hb in the lungs
- Iron remains in Fe²⁺ state (oxygenation, not oxidation)
- Bright cherry-red color
- Normal physiological carrier of oxygen
- Releases O₂ in tissues (facilitated by low pO₂, low pH, high CO₂, high temperature, high 2,3-BPG - Bohr effect)
2. Deoxyhemoglobin (Reduced Hb / HHb)
- Hb after O₂ is released in tissues
- Iron remains in Fe²⁺ state
- Dark purplish-red color
- Responsible for blue coloration (cyanosis) when >5 g/dL in blood
- Also carries CO₂ and H⁺ (buffering)
3. Carbaminohemoglobin (HbCO₂)
- CO₂ binds to free amino (-NH₂) groups of globin chains (not to heme iron)
- Forms carbamino compounds: Hb-NH-COOH
- Carries ~20-25% of CO₂ from tissues to lungs
- Does NOT affect oxygen carrying capacity of heme iron
- Favored in tissues (↑ CO₂, ↓ O₂)
4. Glycated Hemoglobin (HbA1c)
- Hb with glucose non-enzymatically attached to the N-terminal valine of β-chains (Schiff base → Amadori product)
- Normal value: 4-6% of total Hb
- Not affected by short-term fluctuations in blood glucose
- Reflects average blood glucose over past 2-3 months (lifetime of RBC ~120 days)
- Key diagnostic test for diabetes monitoring:
- Diabetic control: <7%
- Poor control: >8%
5. Methemoglobin (MetHb / Hi)
- Iron is oxidized from Fe²⁺ → Fe³⁺ (ferric state)
- Cannot bind O₂ reversibly → functional anemia
- Normal level: <1.5% of total Hb
- Blood color: chocolate brown
- Cyanosis appears at ~1.5 g/dL MetHb (vs. 5 g/dL deoxy-Hb)
- Nitrites, nitrates, chlorates
- Sulfonamides, phenacetin, dapsone, aniline dyes
- Ferrous sulfate (large doses)
- Deficiency of NADH-cytochrome b5 reductase (autosomal recessive)
- Structurally abnormal Hb (Hb M) - tyrosine substituted for histidine in heme pocket
- Normally by NADH-cytochrome b5 reductase (primary)
- Backup: ascorbic acid, reduced glutathione, NADPH-MetHb reductase
- Methylene blue (IV) - activates NADPH-MetHb reductase pathway (rapid)
- Ascorbic acid (for hereditary form)
6. Carboxyhemoglobin (HbCO)
- Carbon monoxide (CO) binds to heme iron at the same site as O₂
- Affinity of CO for Hb is 200-250 times greater than O₂
- Cannot carry O₂ → causes cellular asphyxia
- Also causes left shift of O₂ dissociation curve (remaining Hb binds O₂ more tightly)
- Blood color: bright cherry-red (similar to HbO₂ - can mask cyanosis)
- Source: car exhaust, coal gas, fires, smoking
7. Sulfhemoglobin (SHb)
- Sulfur is incorporated into heme ring during oxidative hemolysis
- Forms a green hemochrome (mixture of oxidized, partially denatured Hb)
- Blood color: mauve-lavender (greenish)
- Cannot carry O₂
- Cannot be reduced back to Hb (irreversible) - remains until RBCs are destroyed
- Can combine with CO to form carboxysulfhemoglobin
- Normal level: <1%
- Sulfonamides, phenacetin, acetanilid
- Clostridium perfringens bacteremia
- Severe constipation (enterogenous cyanosis)
- Exposure to hydrogen sulfide (H₂S)
8. Cyanmethemoglobin (HiCN)
- Formed when methemoglobin reacts with cyanide (CN⁻)
- Has high affinity of MetHb for cyanide
- Stable compound used in laboratory measurement of total Hb (Drabkin's method/Cyanmethemoglobin method - gold standard for Hb estimation)
- Used therapeutically in cyanide poisoning: nitrites → MetHb → MetHb binds CN⁻ → cyanmethemoglobin (less toxic)
Quick Comparison Table
| Derivative | Iron State | O₂ Carrying | Color | Key Feature |
|---|---|---|---|---|
| Oxyhemoglobin | Fe²⁺ | ✓ Yes | Cherry-red | Normal; O₂ in lungs |
| Deoxyhemoglobin | Fe²⁺ | ✓ (released) | Dark red | Normal; O₂ released |
| Carbaminohemoglobin | Fe²⁺ | ✓ Yes | - | CO₂ on globin, not heme |
| HbA1c | Fe²⁺ | ✓ Yes | - | Glucose on β-chain; diabetes marker |
| Methemoglobin | Fe³⁺ | ✗ No | Chocolate brown | Oxidized iron |
| Carboxyhemoglobin | Fe²⁺ | ✗ No | Cherry-red | CO poisoning; 200× affinity |
| Sulfhemoglobin | Altered ring | ✗ No | Mauve-green | Irreversible; sulfonamides |
| Cyanmethemoglobin | Fe³⁺ | ✗ No | - | Lab standard; cyanide antidote basis |
Dyshemoglobins = MetHb + HbCO + SHb + HiCN - collectively cannot carry O₂ and are not measured by pulse oximetry (co-oximetry needed)
Types of normal haemoglobin 3marks answer
Types of Normal Hemoglobin
In Normal Adults
| Type | Chain Composition | % in Adults | Notes |
|---|---|---|---|
| HbA | α₂β₂ | ~96-97% | Major adult hemoglobin |
| HbA₂ | α₂δ₂ | ~2-3% | Minor adult hemoglobin |
| HbF | α₂γ₂ | <1% | Trace in adults (major in fetus) |
During Development (Developmental Sequence)
| Stage | Hemoglobin | Chains |
|---|---|---|
| Embryonic | Hb Gower 1 | ζ₂ε₂ |
| Hb Gower 2 | α₂ε₂ | |
| Hb Portland | ζ₂γ₂ | |
| Fetal | HbF | α₂γ₂ |
| Adult | HbA | α₂β₂ |
| HbA₂ | α₂δ₂ |
Key Points
- All normal Hb types contain α-chains - encoded on chromosome 16
- β, δ, γ, ε chains are encoded on chromosome 11
- HbF has higher O₂ affinity than HbA (less 2,3-BPG binding) → ensures O₂ transfer from mother to fetus
- HbA₂ is elevated (>3.5%) in β-thalassemia trait - important diagnostic marker
- At birth: ~70% HbF, 30% HbA; by 6 months, adult proportions are established
"All adults have A (α₂β₂), a bit of A2 (α₂δ₂), and a forgotten F (α₂γ₂)"
What are hemoglobinopathies describe briefly 6 marks
Hemoglobinopathies
Definition
- Structural abnormality - abnormal globin chain sequence (qualitative defect)
- Reduced synthesis of one or more globin chains (quantitative defect - thalassemias)
Classification
| Type | Defect | Examples |
|---|---|---|
| Structural variants | Abnormal amino acid in globin chain | HbS, HbC, HbE, HbM |
| Thalassemias | Reduced/absent globin chain synthesis | α-thalassemia, β-thalassemia |
| Unstable Hb | Hb precipitates → Heinz bodies | Hb Köln, Hb Zürich |
| Hb with altered O₂ affinity | High or low affinity Hb | Hb Chesapeake (high), Hb Kansas (low) |
| Methemoglobinemia (Hb M) | Iron stays Fe³⁺ | Hb M Boston, Hb M Saskatoon |
1. Sickle Cell Disease (HbS) - Most Important
- Glutamic acid → Valine at position 6 of the β-chain
- HbA (α₂β₂) → HbS (α₂βs₂)
- HbAS = Sickle cell trait (heterozygous) - usually asymptomatic, protective against malaria
- HbSS = Sickle cell disease (homozygous) - severe clinical manifestations
- Under low O₂ tension → HbS polymerizes → RBCs become sickle-shaped
- Sickled RBCs: rigid, occlude small vessels → vaso-occlusive crises
- Sickled RBCs are fragile → hemolytic anemia
- Chronic hemolytic anemia (Hb 6-9 g/dL)
- Painful vaso-occlusive crises (bones, chest, abdomen)
- Splenomegaly → progressive splenic infarction → autosplenectomy
- Susceptibility to infections (especially encapsulated organisms)
- Stroke, avascular necrosis, renal papillary necrosis
- Sickle cells on blood smear
- ↑ Reticulocytes
- HbS on electrophoresis
2. Thalassemias - Most Common Hemoglobinopathy Worldwide
α-Thalassemia
- α-globin genes deleted (normally 4 α-globin genes)
- Caused by gene deletions
| Genotype | Condition | Features |
|---|---|---|
| -α/αα (1 gene deleted) | Silent carrier | No symptoms |
| --/αα or -α/-α (2 deleted) | α-thalassemia trait | Mild microcytic anemia |
| --/-α (3 deleted) | HbH disease | Moderate hemolytic anemia; HbH (β₄ tetramers) |
| --/-- (4 deleted) | Hb Barts (hydrops fetalis) | γ₄ tetramers; fatal in utero |
β-Thalassemia
- β-globin gene mutations (point mutations, deletions)
- Excess α-chains precipitate → damage RBCs
| Genotype | Condition | Features |
|---|---|---|
| β/β⁺ or β/β⁰ | Thalassemia minor (trait) | Mild anemia, ↑HbA₂ (>3.5%) |
| β⁺/β⁺ or β⁰/β⁺ | Thalassemia intermedia | Moderate anemia, splenomegaly |
| β⁰/β⁰ | Thalassemia major (Cooley's anemia) | Severe; transfusion dependent from infancy |
- Severe microcytic, hypochromic anemia
- Hepatosplenomegaly (extramedullary hematopoiesis)
- "Hair on end" skull X-ray (marrow expansion)
- Frontal bossing, "chipmunk face"
- Growth retardation
- HbF elevated (compensatory)
3. HbC
- Glutamic acid → Lysine at position 6 of β-chain
- Common in West African populations
- HbCC: mild hemolytic anemia, target cells on smear
- HbSC: moderate sickle cell disease
4. HbE
- Glutamic acid → Lysine at position 26 of β-chain
- Common in Southeast Asia
- HbEE: mild microcytic anemia
- HbE + β-thalassemia: severe, resembles thalassemia major
Summary Table
| Hemoglobinopathy | Defect | Key Feature |
|---|---|---|
| Sickle cell disease | Glu→Val at β6 | Vaso-occlusion, hemolysis |
| β-Thalassemia major | ↓/absent β-chain | Transfusion dependent, chipmunk face |
| α-Thalassemia | α-gene deletions | HbH disease, hydrops fetalis |
| HbC | Glu→Lys at β6 | Mild hemolysis, target cells |
| HbE | Glu→Lys at β26 | Common in SE Asia, mild anemia |
All structural hemoglobinopathies = qualitative defect (wrong amino acid) All thalassemias = quantitative defect (less/no chain made) Most common hemoglobinopathy worldwide = β-thalassemia trait Most common structural hemoglobinopathy = Sickle cell disease
Detail on sickle cell anaemia (molecular basis classsification consequences diagnosis complications treatment partial advantage 5 marks and short note on thalassemia 5marks
SICKLE CELL ANAEMIA
Definition
Molecular Basis
GAG → GTG (Adenine → Thymidine)
| Normal HbA | Sickle HbS |
|---|---|
| α₂β₂ (β has Glu at position 6) | α₂βs₂ (βs has Val at position 6) |
- Glutamic acid is polar, charged (hydrophilic)
- Valine is non-polar (hydrophobic)
- Substitution creates a hydrophobic "sticky patch" on HbS
- Under low O₂ tension (deoxygenation), HbS molecules polymerize into long rigid fibers
- Polymer formation → sickle-shaped RBCs (drepanocytes)
- On re-oxygenation, polymers disaggregate → reversible sickling initially, but repeated cycles cause irreversible membrane damage
Classification
| Genotype | Type | Features |
|---|---|---|
| HbSS | Sickle cell disease (homozygous) | Severe; full clinical manifestations |
| HbAS | Sickle cell trait (heterozygous) | Usually asymptomatic; protective against malaria |
| HbSC | SC disease | Moderate; both HbS and HbC |
| HbS + β-thalassemia | Sickle-thal | Variable severity |
| HbSS + HbF ↑ | Ameliorated SCD | HbF inhibits polymerization → milder |
Consequences / Pathophysiology
1. Hemolytic Anaemia
- Sickled cells are rigid and fragile → destroyed by macrophages (extravascular hemolysis) or lysed in vessels (intravascular hemolysis)
- RBC lifespan reduced from 120 days to 10-20 days
- Chronic hemolytic anaemia (Hb ~6-9 g/dL)
- ↑ Bilirubin → jaundice, pigment gallstones
2. Vaso-occlusion
- Rigid sickle cells + activated endothelium → block small blood vessels
- Causes tissue ischemia and infarction
- Affects: bones, lungs, brain, spleen, kidneys, penis
Complications
| Organ/System | Complication |
|---|---|
| Blood | Chronic hemolytic anaemia, aplastic crisis (Parvovirus B19) |
| Bones | Painful vaso-occlusive crisis, avascular necrosis (femoral head), dactylitis (hand-foot syndrome in children) |
| Spleen | Splenic sequestration → autosplenectomy by adulthood |
| Lungs | Acute chest syndrome (fever + chest pain + infiltrates) |
| Brain | Stroke (ischemic), cognitive impairment |
| Kidney | Renal papillary necrosis, hematuria, renal failure |
| Eyes | Proliferative retinopathy → blindness |
| Penis | Priapism |
| Liver | Hepatomegaly, cholelithiasis (pigment stones) |
| Infections | ↑ susceptibility (especially encapsulated organisms - pneumococcus, Hib) due to splenic dysfunction |
Diagnosis
- Hb: 6-9 g/dL
- ↑ Reticulocyte count (5-15%)
- ↑ Bilirubin (unconjugated)
- ↑ LDH
| Test | Findings |
|---|---|
| Hb Electrophoresis | HbS (~90%), no HbA, ↑ HbF; gold standard |
| HPLC | Confirms HbS (most accurate) |
| Sickling test (Sickledex/Solubility test) | HbS becomes insoluble in deoxygenated solution → turbid (positive) |
| Sickle preparation (sodium metabisulfite) | RBCs sickle under microscope |
| Newborn screening | Heel prick - HPLC/IEF (identifies HbFS pattern) |
| Prenatal diagnosis | DNA analysis of chorionic villi or amniocentesis |
Treatment
Supportive
- Folic acid supplementation (↑ erythropoiesis demand)
- Prophylactic penicillin (from infancy, due to functional asplenia)
- Vaccinations: pneumococcal, Hib, meningococcal, influenza
- Pain management: NSAIDs, opioids during crises
- Blood transfusions: for severe anaemia, stroke prevention, acute chest syndrome
Disease-Modifying
- Hydroxyurea - drug of choice
- Increases HbF production → HbF inhibits HbS polymerization
- Reduces sickling, frequency of painful crises, acute chest syndrome, transfusion need
- Mechanism: activates guanylate cyclase → ↑ cGMP → reactivates γ-globin gene
- Voxelotor - prevents HbS polymerization directly (newer agent)
- Crizanlizumab - anti-P-selectin antibody, reduces vaso-occlusive crises
Curative
- Allogeneic haematopoietic stem cell transplantation (HSCT) - only cure currently
- Best results in children with matched sibling donor
- Gene therapy (CRISPR-Cas9) - reactivates γ-globin or corrects HBB mutation (emerging)
Partial Advantage (Heterozygote Advantage)
Mechanisms of protection:
- Sickling in parasitized RBCs: Low O₂ in capillaries → RBCs with parasites sickle → phagocytosed before parasites mature
- Impaired parasite growth: Sickle cells are a hostile environment - ↓ K⁺, ↓ pH, altered membrane → poor parasite survival
- Enhanced immune clearance: Sickled infected cells are more readily recognized and destroyed by macrophages
- Reduced rosetting: HbS reduces RBC-RBC adhesion that P. falciparum uses to evade immunity
SHORT NOTE ON THALASSEMIA
Definition
- The name comes from Greek: "thalassa" (sea) - as they were first described around the Mediterranean Sea
Classification
A. By Globin Chain Affected
| Type | Defective Chain | Chromosome | Molecular Defect |
|---|---|---|---|
| α-Thalassemia | α-globin | 16 | Gene deletions (mainly) |
| β-Thalassemia | β-globin | 11 | Point mutations (mainly) |
β-Thalassemia
- Transcription (promoter mutations)
- RNA splicing (most common)
- Translation (nonsense codons, frameshifts)
| Type | Genotype | Hb level | Clinical Features |
|---|---|---|---|
| β-Thalassemia minor (trait) | β/β⁰ or β/β⁺ | Mild ↓ (10-13 g/dL) | Usually asymptomatic; microcytic hypochromic RBCs |
| β-Thalassemia intermedia | β⁺/β⁺ or β⁰/β⁺ | Moderate ↓ (7-10 g/dL) | Moderate anaemia; splenomegaly; not always transfusion-dependent |
| β-Thalassemia major (Cooley's anaemia) | β⁰/β⁰ | Severe ↓ (<7 g/dL) | Severe; transfusion-dependent from 6 months of age |
- ↓ β-chains → ↓ HbA formation → microcytic hypochromic anaemia
- Excess α-chains accumulate → form toxic precipitates → damage RBC membrane
- Ineffective erythropoiesis: erythroid precursors die in bone marrow by apoptosis
- Compensatory: bone marrow expansion → bony deformities; extramedullary haematopoiesis → organomegaly
- ↑ Iron absorption (due to ↓ hepcidin) → iron overload even without transfusions
- Severe microcytic, hypochromic anaemia (presents at 6 months - when HbF is replaced by HbA)
- Hepatosplenomegaly (extramedullary haematopoiesis)
- Skeletal deformities: frontal bossing, prominent cheek bones, "chipmunk face"
- "Hair-on-end" skull X-ray appearance (marrow expansion)
- Failure to thrive, growth retardation
- Iron overload: cardiac failure, liver cirrhosis, diabetes, hypogonadism (from transfusions + ↑ absorption)
- Jaundice, gallstones
α-Thalassemia
| Genes Deleted | Type | Clinical Features | Abnormal Hb |
|---|---|---|---|
| 1 gene (-α/αα) | Silent carrier | Normal | None |
| 2 genes (--/αα or -α/-α) | α-Thalassemia trait | Mild microcytic anaemia | None significant |
| 3 genes (--/-α) | HbH disease | Moderate haemolytic anaemia; splenomegaly | HbH (β₄) |
| 4 genes (--/--) | Hydrops fetalis | Fatal in utero/at birth | Hb Barts (γ₄) |
- HbH (β₄ tetramers) and Hb Barts (γ₄) have very high O₂ affinity → useless for O₂ delivery
- Hydrops fetalis: severe oedema, ascites, cardiac failure in fetus → stillbirth
Diagnosis
| Test | β-Thalassemia minor | β-Thalassemia major |
|---|---|---|
| CBC | Microcytic hypochromic anaemia (mild) | Severe microcytic hypochromic anaemia |
| Blood smear | Target cells, basophilic stippling | Target cells, nucleated RBCs, poikilocytosis |
| Hb electrophoresis | ↑ HbA₂ (>3.5%) - diagnostic | ↑ HbF, absent/↓ HbA, ↑ HbA₂ |
| Serum iron/ferritin | Normal or ↑ (unlike iron deficiency) | ↑↑ |
| DNA analysis | Identifies specific mutation | Confirms diagnosis |
Key: ↑ HbA₂ (>3.5%) is the hallmark of β-thalassemia minor/trait
Treatment
| Condition | Treatment |
|---|---|
| Thalassemia minor | Genetic counseling; folic acid; iron only if truly deficient |
| HbH disease | Folic acid; transfusions during crises |
| Thalassemia major | Regular blood transfusions every 2-5 weeks (maintain Hb >9-10.5 g/dL) |
| Iron overload | Iron chelation: Deferasirox (oral, preferred), Deferoxamine (SC infusion), Deferiprone |
| Splenectomy | If hypersplenism increases transfusion requirements |
| Curative | Allogeneic HSCT (bone marrow transplant) - best in young patients with matched sibling donor |
| Emerging | Gene therapy (CRISPR-Cas9, lentiviral vectors); Luspatercept (reduces ineffective erythropoiesis) |
Thalassemia and Malaria (Advantage)
- Like sickle cell, thalassemia genes are most frequent in malaria-endemic regions
- Thalassemia carriers have partial protection against P. falciparum malaria - another example of balanced polymorphism
- Thalassemia = quantitative defect (less/no chain); SCD = qualitative defect (wrong chain)
- β-thalassemia major diagnosed at ~6 months (when HbF falls and HbA is expected)
- HbA₂ >3.5% = β-thalassemia trait
- "Chipmunk face" + hair-on-end X-ray = β-thalassemia major
- Curative treatment = bone marrow transplant
What is jaundice and types of jaundice and explain findings in urine and blood
What is jaundice and types of jaundice and explain findings in urine and blood