Sick sinus syndrome
Reading File
Finding Sources
Searching PubMed
"sick sinus syndrome"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full response:
Sick Sinus Syndrome (Sinus Node Dysfunction)
Definition
Sick sinus syndrome (SSS), also called sinus node dysfunction (SND), is a term applied to a collection of sinus nodal abnormalities. These include:
- Persistent spontaneous sinus bradycardia inappropriate for the physiologic circumstance
- Sinus arrest or sinoatrial (SA) exit block
- Combinations of SA and AV conduction disturbances
- Bradycardia-tachycardia syndrome - alternation of paroxysmal rapid atrial tachyarrhythmias with periods of slow atrial and ventricular rates
- Chronotropic incompetence - failure to increase heart rate appropriately with physiologic demand
More than one of these conditions can be seen in the same patient on different occasions, and their mechanisms are often causally interrelated.
- Braunwald's Heart Disease, p. 575-577
Epidemiology
- SSS is the leading diagnosis for pacemaker implantation
- Most common in the elderly: occurs in 1 in 600 cardiac patients >65 years of age
- Acquired causes include cardiomyopathy, congestive heart failure, ischemic heart disease, and metabolic diseases
- "Idiopathic SND" (no identifiable cardiac anomaly) can occur at any age, including in utero
- Familial forms exist with both autosomal dominant (reduced penetrance) and autosomal recessive (complete penetrance) inheritance
- In children, it most frequently occurs with congenital or acquired heart disease, particularly after corrective cardiac surgery (Mustard, Senning, or Fontan procedures)
Pathophysiology / Anatomy
The anatomic basis can involve:
- Total or subtotal destruction of the sinus node
- Areas of nodal-atrial discontinuity
- Inflammatory or degenerative changes in the nerves and ganglia surrounding the node
- Pathologic changes in the atrial wall (fibrosis and fatty infiltration)
The sclerodegenerative process typically involves the sinus node AND the AV node or the bundle of His and its branches. This is why SSS is best thought of as a diffuse degenerative disease of the heart's electrical system, not an isolated sinus node problem.
Occlusion of the sinus node artery can also cause sinus node dysfunction.
Genetic Basis
Four genes are implicated in idiopathic SSS:
| Gene | Mechanism | Notes |
|---|---|---|
| SCN5A | Loss-of-function sodium channel variants | 15 putative causative variants; also linked to Brugada syndrome and cardiac conduction disease (CCD) - mixed phenotypes common |
| HCN4 | Encodes the I_f ("funny") pacemaker current - key to sinus node automaticity. Loss-of-function variants | p.D553N-HCN4: associated with severe bradycardia, syncope, QT prolongation, and polymorphic VT (TdP) |
| ANK2 | Ankyrin-B - scaffolding protein for ion channels | |
| MYH6 | Myosin heavy chain 6 |
Clinical Manifestations
Symptoms result from both the bradyarrhythmias and tachyarrhythmias:
- Dizziness, lightheadedness
- Syncope (Stokes-Adams attacks) - though isolated sinus node dysfunction rarely causes syncope; syncope in SSS is more often due to reentrant atrial tachycardia
- Palpitations (from tachyarrhythmia episodes)
- Fatigue, exercise intolerance (from chronotropic incompetence)
- Sudden cardiac death (rare but recognized)
The course is frequently intermittent and unpredictable, influenced by the severity of underlying heart disease.
ECG Recognition
Bradycardia-Tachycardia Syndrome
The classic pattern: paroxysmal tachyarrhythmia (usually atrial fibrillation or flutter) followed by a prolonged post-conversion pause before sinus rhythm resumes.

Figure: SSS with bradycardia-tachycardia (Braunwald's, Fig. 68.3). Top - intermittent sinus arrest with junctional escape beats (red circles). Bottom - atrial flutter followed by ~5 seconds of asystole before junctional escape resumes. The patient became presyncopal.
Sinus Node Exit Block
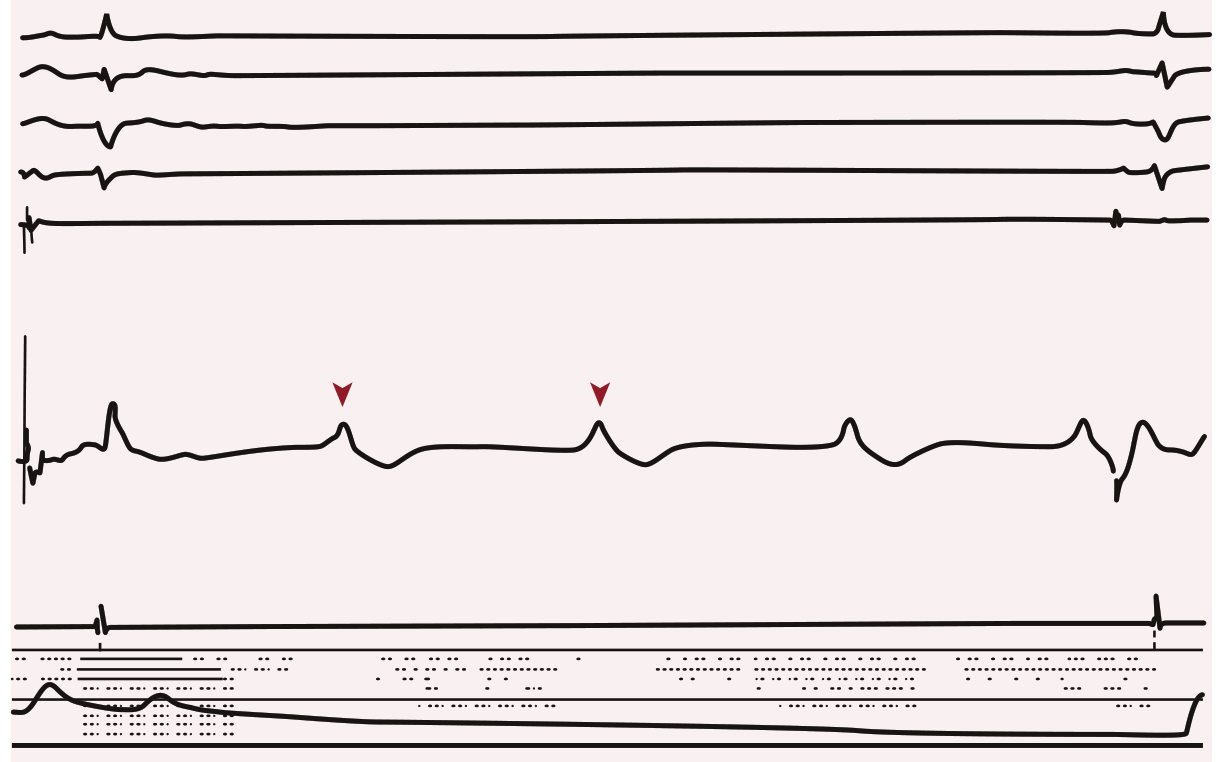
Figure: Sinus node exit block. Sinus node potentials (arrowheads) visible on intracardiac recording, failing to conduct to the atrium. Leads I, II, III, V1, right atrial (RA), sinus node (SN), and right ventricular apex (RVA) recordings shown, with femoral artery blood pressure at bottom.
Holter/Loop Recorder Findings
A loop recorder in a patient with syncope showing a paroxysmal sinus pause of nearly 30 seconds is a classic finding (Braunwald's, Fig. 68.2). The sinus cycle length often lengthens just before the pause - suggesting an autonomic component.
Tachycardia-Bradycardia Syndrome (TBS)
A subtype where the tachyarrhythmia (typically AF or atrial flutter) terminates with an excessive post-conversion pause. TBS can also occur during AF when rapid ventricular rate periods alternate with excessive bradycardia from high-grade AV block. While TBS can occur without medications, it typically occurs as a result of treatment with beta blockers or calcium channel blockers.
Chronotropic Incompetence
Defined as failure to achieve 80-85% of the maximal expected heart rate (or inadequate heart rate reserve) during physiologic demand. The normal heart rate increase with exercise relies on an exquisite balance of sympathetic and parasympathetic inputs to the sinus node. Chronotropic incompetence reflects failure of this balance.
Diagnosis
- 12-lead ECG: May show sinus bradycardia, SA exit block, or prolonged pauses
- Holter monitoring (24-48 hours): Most useful for episodic symptoms; can detect extremely slow heart rates, prolonged pauses, and alternating tachycardias
- Implantable loop recorder: For infrequent symptoms - can reveal paroxysmal sinus arrest (as in Fig. 68.2)
- Exercise stress test: For chronotropic incompetence
- Electrophysiology (EP) study: Can assess sinus node recovery time and SA conduction time; useful when non-invasive testing is inconclusive
Management
Treatment depends on the nature and severity of the rhythm problem:
| Situation | Treatment |
|---|---|
| Symptomatic bradycardia / sinus pauses | Permanent pacemaker implantation |
| Bradycardia-tachycardia syndrome | Pacing + antiarrhythmic drug therapy (pacing protects against bradycardia while drugs control tachycardia) |
| Chronotropic incompetence | Rate-responsive pacemaker |
| Tachyarrhythmia component | Beta blockers, calcium channel blockers, antiarrhythmics - with caution (may worsen bradycardia) |
Key caveat from Tintinalli's: Pacemaker placement prevents bradycardia but not tachycardia - sudden death can still occur after pacemaker placement in SSS because tachyarrhythmias are not addressed by pacing alone.
Preferred pacing mode: Physiologic (atrial-based) pacing (AAI or DDD) is preferred over VVI pacing in SSS, as it reduces the risk of AF and pacemaker syndrome.
Related Conditions (Differential)
- Lénègre's disease: Idiopathic sclerodegeneration of the AV node and bundle branches
- Lev's disease: Fibrosis/calcification invading the conduction system from adjacent cardiac structures
- Vagotonia (excessive physical training can heighten vagal tone and produce sinus bradycardia/syncope in otherwise normal individuals)
- Medications (beta blockers, calcium channel blockers, digoxin, amiodarone, lithium - SSS is a contraindication to lithium use)
Summary Table
| Feature | Detail |
|---|---|
| Synonym | Sinus node dysfunction (SND), tachycardia-bradycardia syndrome |
| Age group | Primarily >65 years (1/600 cardiac patients); can occur at any age |
| Key ECG findings | Sinus bradycardia, sinus arrest, SA exit block, post-tachycardia pauses |
| Leading diagnosis for | Pacemaker implantation |
| Key genes | SCN5A, HCN4, ANK2, MYH6 |
| Key treatment | Permanent pacemaker ± antiarrhythmics |
| Diagnostic tool | Holter monitoring / implantable loop recorder |
Recent literature (PubMed): A 2025 review in Clinical Science (PMID 40497650) highlights aging mechanisms and future therapeutic directions in sinus node dysfunction, including the role of fibrosis, ion channel remodeling, and potential biological pacemaker strategies.
Sources: Braunwald's Heart Disease, p. 575-577; Ganong's Review of Medical Physiology, 26th ed.; Tintinalli's Emergency Medicine, 9th ed.; Tintinalli's EM (Pediatric Arrhythmias section)
This is a shared conversation. Sign in to Orris to start your own chat.