Diabetic foot
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetic foot"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Searching Images
diabetic foot ulcer classification Wagner
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Diabetic Foot
Epidemiology
Up to one-third of people with diabetes will develop a foot ulcer during their lifetime. Over half of these ulcers become infected. Diabetic foot ulcers (DFUs) are an independent risk factor for premature death — five-year mortality following a major lower extremity amputation drops from 70% to 43%. Approximately 20% of all diabetic hospitalizations are related to foot problems. — Sabiston Textbook of Surgery, 14e; Rosen's Emergency Medicine
Pathophysiology — The Triad
Three core mechanisms drive diabetic foot disease:
1. Peripheral Neuropathy
- Sensory neuropathy: Polyneuropathic loss begins in a stocking distribution and progresses proximally. Loss of protective sensation is the most common cause of plantar ulcers. Diagnosed by the inability to perceive the 5.07 Semmes-Weinstein monofilament — 90% of patients who cannot feel this have lost protective sensation; carries a 30% risk of ulcer development.
- Autonomic neuropathy: Abnormal sweating → dry foot → fissuring cracks → portal for infection
- Motor neuropathy: Commonly involves the common peroneal nerve → foot drop; intrinsic muscle atrophy → claw toes and toe-tip ulcerations from excessive pressure — Miller's Review of Orthopaedics, 9e
2. Peripheral Vascular Disease
- Occurs in 60–70% of patients with >10 years of diabetes; affects both large and small vessels
- Ankle-brachial index (ABI): minimum for healing 0.45, normal 1.0; values >1.3 indicate arterial calcification (falsely elevated)
- Absolute toe pressures: minimum for healing 40 mmHg; TcPO₂ >40 mmHg predictive of healing — Miller's Review of Orthopaedics, 9e
3. Immune Impairment
- Impaired phagocytosis, altered WBC chemotaxis, and poor cytotoxic environment from hyperglycemia impair bacterial clearance
- Metabolic markers predicting poor healing: albumin <2.5 g/dL, total protein <6.0 g/dL, WBC <1500/mm³
Additional Factor: Hypomobility Syndrome
Excessive glycosylation of soft tissues → decreased joint ROM → altered biomechanics → abnormal plantar pressure distribution
Risk Factors (Harrison's 22E, 2025)
- Peripheral motor, sensory, and autonomic neuropathy
- Neuro-osteoarthropathic deformities (Charcot foot)
- Arterial insufficiency
- Uncontrolled hyperglycemia
- Disabilities (e.g., reduced vision)
- Maladaptive behavior
Classification Systems
Wagner–Meggitt Classification (most widely used)
| Grade | Description | Treatment |
|---|---|---|
| 0 | Skin intact; bony deformity ("at risk") | Extra-depth shoes, pressure-relief insoles |
| 1 | Superficial ulcer; no tendon/bone | In-office débridement + total contact cast |
| 2 | Deep ulcer with exposed tendon/joint capsule | Operative débridement, then casting |
| 3 | Extensive ulcer; exposed bone/osteomyelitis or abscess | Surgical débridement of bone + nonviable tissue |
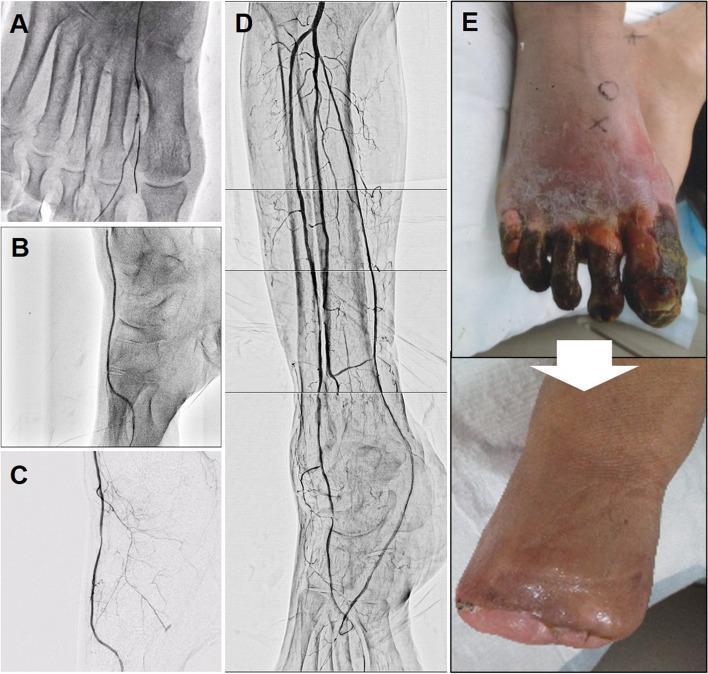
| 4 | Forefoot gangrene | Revascularization; partial foot amputation |
| 5 | Whole foot gangrene | Below- or above-knee amputation |
Limitation: does not account for neuropathy or ischemia; cannot reliably distinguish infectious from ischemic lesions.
IWGDF/IDSA Classification (2023) — Validated
| Grade | Definition |
|---|---|
| 1 — Uninfected | No signs of infection |
| 2 — Mild | ≥2 local signs (swelling, erythema <2 cm, warmth, pain, purulence); no systemic signs |
| 3 — Moderate | Erythema ≥2 cm, or deep tissue involvement (tendon, joint, bone); no SIRS |
| 4 — Severe | Any foot infection + ≥2 SIRS criteria (temp >38°C or <36°C, HR >90, RR >20, WBC >12,000 or <4,000) |
| Add (O) | If osteomyelitis is present |
— Sabiston Textbook of Surgery, Table 35.5; IWGDF/IDSA Guidelines 2023
Clinical photographs of Wagner Grades 1–4:

Microbiology
- Mild infections: Gram-positive cocci — S. aureus (including MRSA) and streptococci
- Moderate–severe infections: Polymicrobial — aerobic gram-positive cocci + gram-negative bacilli (Pseudomonas, Enterobacteriaceae) + anaerobes (especially in chronic wounds)
- MRSA prevalence varies widely (5–43% globally); gram-negative pathogens more common in tropical/developing settings
- Bone biopsy cultures are the gold standard; wound swab–bone biopsy correlation is only 24% — Harrison's 22E; Rosen's Emergency Medicine
Diagnosis
| Test | Notes |
|---|---|
| Clinical exam | Primary method; assess depth, erythema extent, crepitation, lymphangitis |
| Probe-to-bone test | PPV ~90% in high-pretest-probability settings; positive = osteomyelitis likely |
| Plain X-ray | Sensitivity 30–50%; useful for gas, foreign body, follow-up of confirmed osteomyelitis |
| MRI | Best for osteomyelitis — sensitivity 80–100%, specificity 80–90%; earliest diagnosis |
| CT | Identifies deeper abscesses |
| CRP / ESR | Supports diagnosis in equivocal cases; no isolated value is diagnostic |
| Cultures | Deep tissue > superficial swab; bone biopsy for osteomyelitis |
Treatment
General Principles
- Glycemic control (euglycemia maintenance)
- Moist wound environment
- Débridement of necrotic/callused tissue — lowers peak plantar pressure, reduces recurrence
- Offloading — total contact cast (gold standard for neuropathic ulcers); orthotic devices, non-weight-bearing
Antibiotic Therapy
| Severity | Regimen |
|---|---|
| Mild | Oral anti-gram-positive coverage: TMP-SMX 800/160 mg BID, cephalexin 500 mg QID, or clindamycin 300 mg QID |
| Moderate–Severe | IV broad-spectrum: piperacillin-tazobactam 3.375 g q8h + vancomycin 15 mg/kg q12h |
| Osteomyelitis (no resection) | 6-week antibiotic course |
| Osteomyelitis (post-débridement) | 3-week course (non-inferior in RCT) |
Surgical Indications
- Urgent: necrotizing infection, deep abscess, compartment syndrome, limb ischemia
- Débridement combined with antibiotics avoids amputation in ~two-thirds of patients
Adjunctive Therapies
- Negative pressure wound therapy (NPWT): shown effective in randomized trials (systematic review, PMID 39241769)
- Hyperbaric oxygen: some efficacy in complicated infections, especially anaerobic
- Revascularization: required when ischemia is present; transcutaneous oxygen measurements (TcPO₂) guide selection
Footwear (Prevention)
- Extra-depth shoes lined with Plastazote (closed-cell polyethylene) — lightweight, shock-absorbing
- Custom total contact inserts (3/year under the Diabetic Therapeutic Shoe Bill)
Charcot Foot (Neuroarthropathy)
A noninfectious, destructive process from cumulative undetected trauma due to sensory neuropathy. Results in repeated fractures → collapse of foot architecture → "rocker-bottom" deformity (loss of longitudinal arch). Clinically may mimic infection (warm, swollen foot).
Key: Early recognition + non-weight-bearing for ≥8 weeks may prevent severe structural destruction.

Prognosis & Recurrence
- ~50% of healed DFIs recur within 1 year; >90% recur within 10 years
- Up to 15% progress to osteomyelitis; a significant proportion require amputation
- Long-term follow-up ≥1 year needed before declaring infection in remission
Recent Evidence (2024–2026)
- NPWT meta-analysis (PMID 39241769, Wounds 2024): Negative pressure wound therapy is effective for DFUs in RCTs — supports its use as adjunctive treatment.
- Risk factor meta-analysis (PMID 36740805, Vascular 2024): Confirms peripheral neuropathy, poor glycemic control, and prior ulceration as leading risk factors.
Sources: Sabiston Textbook of Surgery 21e · Miller's Review of Orthopaedics 9e · Harrison's Principles of Internal Medicine 22E (2025) · Rosen's Emergency Medicine 10e · IWGDF/IDSA 2023 Guidelines
Peripheral arterial disease
Finding Sources
Finding Sources
Searching PubMed
"peripheral arterial disease"[MeSH Terms] AND management
Reading File
Reading File
Searching Images
peripheral arterial disease ankle brachial index ABI classification
Reading File
Finding Sources
Searching Images
critical limb ischemia rest pain gangrene peripheral artery
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information across all domains. Let me compile the full, structured answer.
Peripheral Arterial Disease (PAD)
Definition
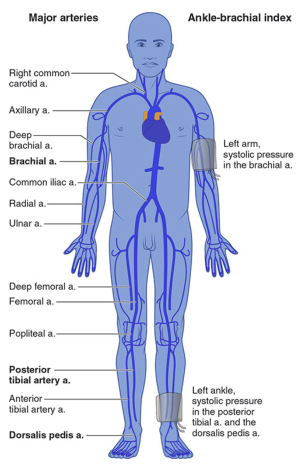
PAD refers to atherosclerotic narrowing or occlusion of peripheral arteries, predominantly the lower extremities. It is defined by an ankle-brachial index (ABI) <0.90 (ratio of highest systolic ankle pressure ÷ highest systolic arm pressure). — Goldman-Cecil Medicine
Epidemiology
- Prevalence in adults ≥40 years: 4.3% overall; rises to 14.5% in those ≥70 years (~4 million individuals in the US)
- In patients with diabetes: prevalence 20–30%
- >95% of PAD patients have at least one traditional cardiovascular risk factor
- >1/3 have significant coronary disease; up to 1/4 have carotid artery disease
- Despite high prevalence, only ~10% of older adults have classic claudication; 50% have atypical symptoms and 40% are asymptomatic
Key systemic risk: PAD is a cardiovascular risk equivalent — nonfatal MI or stroke occur in up to 20% of PAD patients over 5 years, far exceeding limb loss risk. — Goldman-Cecil Medicine; Braunwald's Heart Disease
Risk Factors
| Factor | Notes |
|---|---|
| Cigarette smoking | 2–3× more likely to cause PAD than coronary disease |
| Diabetes mellitus | 2–4× increased PAD risk; 28% increased risk per 1% rise in HbA1c; 7–15× higher amputation risk vs. non-diabetics |
| Hypertension | Strongly associated |
| Dyslipidemia | Risk ↑ 5–10% per 10 mg/dL rise in total cholesterol |
| Hyperhomocysteinemia | 2–3× increased risk |
| CKD / renal impairment | Independent risk factor |
| Age ≥65 | — |
| Non-Hispanic Black race | Disproportionately affected |
Screening indicated in:
- Age ≥65 years
- Age 50–64 with risk factors for atherosclerosis or family history of PAD
- Age <50 with diabetes + ≥1 additional risk factor
- Known atherosclerotic disease in another vascular bed (coronary, carotid, renal, AAA)
— Goldman-Cecil Medicine, Table 65-1
Pathophysiology
- Atherosclerosis is the dominant mechanism, driven by plaque accumulation causing luminal narrowing or occlusion
- Elevated CRP, IL-6, TNF-α, and platelet activation markers reflect the inflammatory substrate
- Acute limb ischemia (ALI): usually from thrombosis (plaque rupture, typically femoral or popliteal artery) or embolism (most commonly mural thrombus from recent MI or atrial appendage thrombus in AF)
- Chronic disease: multisegment atherosclerosis → progressive claudication → critical limb-threatening ischemia (CLTI)
Clinical Syndromes & Classification
PAD manifests as three clinical syndromes: chronic stable ischemia (claudication), chronic critical limb-threatening ischemia (CLTI), and acute limb ischemia (ALI).
Fontaine and Rutherford Classifications
| Fontaine Stage | Clinical | Rutherford Grade | Category | Clinical |
|---|---|---|---|---|
| I | Asymptomatic | 0 | 0 | Asymptomatic |
| IIa | Mild claudication | I | 1 | Mild claudication |
| IIb | Moderate–severe claudication | I | 2 | Moderate claudication |
| — | — | I | 3 | Severe claudication |
| III | Rest pain | II | 4 | Ischemic rest pain |
| IV | Ulceration or gangrene | III | 5 | Minor tissue loss |
| — | — | III | 6 | Major tissue loss |
— Goldman-Cecil Medicine, Table 65-3
Chronic Critical Limb-Threatening Ischemia (CLTI)
- Rest pain, non-healing ulcers, or gangrene
- ABI typically <0.40
- Multisegment disease; risk of limb loss is high without revascularization
Acute Limb Ischemia — The "6 Ps"
Pain, Pallor, Pulselessness, Paresthesias, Paralysis, Poikilothermia (coldness)
- Pallor early → cyanosis with time
- Paralysis = advanced ischemia threatening limb viability → requires urgent revascularization
- Complete motor paralysis = late sign suggesting irreversible injury; progresses to rigor
Differentiating True Claudication from Pseudoclaudication
| Feature | Intermittent Claudication | Spinal Stenosis | Arthritis | Venous Congestion |
|---|---|---|---|---|
| Character | Cramping, tightness | Same or tingling/weakness | Aching | Tightness, bursting |
| Location | Buttock, hip, thigh, calf, foot | Buttock, hip, thigh | Hip, knee | Groin, thigh |
| Exercise-induced | Yes, reproducible distance | Variable | Variable | After walking |
| Occurs with standing | No | Yes | Yes (positional) | Yes (positional) |
| Relief | Rapid with rest | Sitting/position change | Slow | Leg elevation |
— Goldman-Cecil Medicine, Table 65-4
Diagnosis
Ankle-Brachial Index (ABI)
The first-line non-invasive test. Measured with a Doppler probe at the posterior tibial and dorsalis pedis arteries, divided by the highest brachial pressure.
| ABI Value | Interpretation |
|---|---|
| >1.40 | Non-compressible (calcified vessels — falsely elevated) |
| 1.00–1.40 | Normal |
| 0.91–0.99 | Borderline |
| ≤0.90 | PAD (diagnostic) |
| 0.71–0.90 | Mild obstruction |
| 0.41–0.70 | Moderate obstruction |
| 0.00–0.40 | Severe obstruction |
Notes:
- ABI >1.30 in older adults should raise suspicion for arterial calcification; Toe-brachial index (TBI) <0.70 is diagnostic when ABI is unreliable
- Exercise ABI: Claudication = 0.4–0.9; Rest pain = 0.2–0.4; CLTI = 0–0.4
- Probe-to-bone test is not used for PAD but rather for osteomyelitis (as covered in diabetic foot)
Imaging
| Modality | Use |
|---|---|
| Duplex ultrasound | First-line anatomical imaging; maps stenosis location and severity |
| CTA / MRA | Pre-intervention planning; defines anatomy |
| Invasive angiography | Gold standard when revascularization planned |
Treatment
Goals
- Reduce cardiovascular morbidity and mortality (MI, stroke, death)
- Improve walking distance and functional status
- Prevent limb loss
1. Risk Factor Modification (all patients)
- Smoking cessation: Single most important intervention; offer NRT, varenicline, or bupropion; referral to cessation program at every visit
- Statins: High-intensity therapy targeting LDL ≤70 mg/dL; reduces amputation risk and death. PCSK9 inhibitors further reduce major adverse limb events in patients already on statins
- Blood pressure control: Especially in diabetes; β-blockers are NOT contraindicated in PAD
- Glycemic control: Every 1% rise in HbA1c → 28% increased risk of PAD
- Antiplatelet therapy: Aspirin or clopidogrel
2. Exercise Therapy
- Supervised exercise therapy is the preferred initial treatment for claudication — superior to unsupervised programs
- A randomized trial of aortoiliac PAD showed supervised exercise had greater improvement in walking performance vs. primary stenting or home walking + cilostazol
- CMS approved cardiac rehabilitation for symptomatic PAD (2017)
3. Pharmacotherapy
| Drug | Indication | Notes |
|---|---|---|
| Cilostazol 100 mg BID | Intermittent claudication | Phosphodiesterase inhibitor; approved for claudication; contraindicated in heart failure |
| Pentoxifylline | Claudication (second-line) | Inferior to cilostazol |
| Rivaroxaban (low-dose) + aspirin | Symptomatic PAD | Reduces major adverse cardiovascular and limb events (COMPASS trial) |
| Statins | All PAD | Also reduce limb events beyond lipid-lowering |
| Antihypertensives | All PAD with HTN | ACEi/ARB first-line |
4. Revascularization
Indications:
- Disabling claudication refractory to medical therapy and exercise
- Critical limb-threatening ischemia (rest pain, ulcers, gangrene)
- Acute limb ischemia
Approach has shifted from open surgical to endovascular:
| Approach | Preferred When |
|---|---|
| Endovascular (PTA ± stenting, drug-coated balloons, atherectomy) | Aortoiliac (TASC A/B lesions); good short-segment occlusions; high surgical risk |
| Surgical bypass | Complex multilevel disease; long occlusions; failed endovascular; femoropopliteal/tibial |
Acute Limb Ischemia specific management:
- Symptoms <14 days → endovascular-first: intra-arterial thrombolysis (rtPA 0.05–0.1 mg/kg/hr IA) ± catheter thrombectomy ± stenting
- Symptoms >14 days → open surgical thrombectomy ± bypass
- Nonviable limb (irreversible ischemia) → proceed to amputation without angiography
Prognosis
- Natural history of claudication is relatively benign for the limb: critical limb ischemia develops in only 1–2% over 5 years
- However, cardiovascular risk is high: nonfatal MI or stroke occur in ~20% over 5 years
- Critical limb ischemia: high limb-loss risk without revascularization
- Once major amputation occurs, 5-year survival falls substantially due to accelerated cardiovascular disease
Recent Guidelines (2024)
Two major guideline updates were published in 2024:
- 2024 ACC/AHA Guideline for the Management of Lower Extremity Peripheral Artery Disease (PMID 38743805) — Circulation, June 2024
- 2024 ESC Guidelines for the management of peripheral arterial and aortic diseases (PMID 39210722) — European Heart Journal, September 2024
Both guidelines reinforce supervised exercise as first-line for claudication, dual antiplatelet/anticoagulant strategies for high-risk patients, and an endovascular-first approach for most revascularization decisions.
Sources: Goldman-Cecil Medicine, International Edition · Braunwald's Heart Disease, 12e · Fuster and Hurst's The Heart, 15e · 2024 ACC/AHA PAD Guideline · 2024 ESC PAD Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.