Immune Response guyton
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
immune response lymphocytes B cells T cells antibodies Guyton physiology
I now have comprehensive content from Guyton's chapter on immune response. Let me compile a thorough answer.
Immune Response — Guyton and Hall Textbook of Medical Physiology
1. Innate vs. Acquired (Adaptive) Immunity
The body has two broad lines of immune defense:
- Innate immunity — non-specific, present from birth; includes skin barriers, phagocytic cells (neutrophils, macrophages), complement, and natural killer (NK) cells.
- Acquired (adaptive) immunity — develops after exposure to a specific invader; highly specific and forms the basis of immunological memory and vaccination.
Acquired immunity can confer extraordinary protection — e.g., against botulinum or tetanus toxin in doses 100,000× the lethal amount in a non-immune person.
2. Two Types of Acquired Immunity
| Feature | Humoral (B-cell) Immunity | Cell-Mediated (T-cell) Immunity |
|---|---|---|
| Effector | Circulating antibodies (immunoglobulins) | Activated T lymphocytes |
| Produced by | B lymphocytes → plasma cells | T lymphocytes (in thymus-derived lineage) |
| Targets | Extracellular pathogens, toxins, bacteria | Intracellular pathogens, viruses, fungi, transplants, cancer cells |
| Memory | Yes (memory B cells) | Yes (memory T cells) |
3. Antigens
- Antigens are the chemical substances (usually proteins or large polysaccharides, MW ≥ 8,000 Da) that initiate acquired immunity.
- They bear repeating surface groups called epitopes that interact with antigen-specific receptors on lymphocytes.
- Almost any large foreign molecule can be antigenic.
4. Lymphocytes — Central to Acquired Immunity
Lymphocytes are found in:
- Lymph nodes (most abundantly)
- Spleen, thymus, bone marrow
- Submucosal areas of the GI tract (GALT)
- Tonsils and adenoids (intercept upper respiratory antigens)
Without lymphocytes, a newborn dies of fulminant bacterial infection within days.
Origin of B and T Lymphocytes
- Both arise from pluripotent hematopoietic stem cells in the bone marrow.
- T lymphocytes are preprocessed in the thymus (hence "T") → gain antigen specificity and self-tolerance.
- B lymphocytes are preprocessed in the bone marrow (and fetal liver) → gain the ability to form antibodies.
- After preprocessing, millions of B and T cells with different antigen specificities seed the lymphoid tissues of the body.
5. Humoral Immunity — The B-Lymphocyte System
Clonal Selection and Activation
When an antigen enters the body, it contacts B lymphocytes bearing the matching surface receptor. With the help of T-helper (CD4⁺) cells and macrophages (which present antigen and secrete interleukins such as IL-1 and IL-6):
- The matching B cell proliferates rapidly → clonal expansion
- Most daughter cells differentiate into plasma cells, which secrete large quantities of antibody
- Some become memory B cells for a faster secondary response
Antibodies (Immunoglobulins)
Antibodies are gamma globulins (immunoglobulins). The five main classes are IgG, IgA, IgM, IgD, and IgE.
Structure: Each antibody has:
- Two heavy chains + two light chains (connected by disulfide bonds)
- Two Fab regions (antigen-binding)
- One Fc region (activates complement or binds phagocyte receptors)
Mechanisms by Which Antibodies Attack Antigens
- Agglutination — cross-links particulate antigens into clumps
- Precipitation — cross-links soluble antigens until they become insoluble
- Neutralization — covers the toxic or infective sites of antigens
- Lysis — direct rupture of bacterial/cellular membranes (via complement)
- Opsonization — coating pathogens with antibody (and C3b) to enhance phagocytosis
- Activation of complement — triggering the entire complement cascade
Primary vs. Secondary Response
- Primary: Latent period of several days before antibodies appear; peak at ~1–2 weeks; mainly IgM
- Secondary (anamnestic): Starts within hours; far higher antibody titers; mainly IgG; prolonged persistence — basis of immunological memory and vaccination
6. Cell-Mediated Immunity — The T-Lymphocyte System
T-Cell Activation
Antigen is processed by antigen-presenting cells (APCs) — macrophages, dendritic cells, B cells — which display antigen peptides on MHC molecules (Class I or II). T cells recognizing these complexes through their T-cell receptor (TCR) become activated.
Major T-Cell Subsets
| T-Cell Type | Marker | Function |
|---|---|---|
| T-helper (Th) | CD4⁺ | Coordinate immune response; secrete lymphokines; activate B cells and cytotoxic T cells |
| Cytotoxic T cells (CTL) | CD8⁺ | Directly kill antigen-bearing cells; critical vs. viruses, intracellular bacteria, transplants, tumors |
| T-suppressor (Treg) | CD4⁺/CD25⁺/FoxP3⁺ | Suppress excessive immune response; prevent autoimmunity |
How T Cells Kill
- Direct cell lysis — CTLs attach to target cell via TCR-MHC interaction and release perforin/granzymes → apoptosis
- Lymphokines — soluble signals secreted by T-helper cells that amplify the immune response:
- Interleukins (IL-2 and others) — stimulate T and B cell proliferation
- Macrophage migration inhibition factor — keeps macrophages at infection site
- Macrophage-activating factor — boosts phagocytic power of macrophages
- Lymphotoxin (TNF-β) — directly kills cells
- Chemotactic factor — attracts macrophages
- Interferon — antiviral protection
7. Tolerance — Preventing Autoimmunity
The immune system must not attack the body's own tissues. Tolerance is established during lymphocyte preprocessing:
- Central tolerance in the thymus (T cells): T cells that react strongly to self-antigens presented by thymic cells undergo clonal deletion (apoptosis) during development.
- Central tolerance in bone marrow (B cells): Self-reactive B cells are also clonally deleted.
- Peripheral tolerance: Anergy and Treg cells suppress any self-reactive lymphocytes that escape central deletion.
Failure of tolerance → autoimmune diseases (e.g., rheumatoid arthritis, systemic lupus erythematosus, type 1 diabetes).
8. Immunization
- Active immunization (vaccination): Injecting antigens (killed organisms, attenuated organisms, or toxoids) to generate primary immunity and memory; protects against subsequent real infection.
- Passive immunization: Injecting pre-formed antibodies (immunoglobulins) → immediate but transient protection (no memory cells formed). Example: tetanus immunoglobulin after wound exposure.
9. Allergies and Hypersensitivity (Type I — Anaphylactic)
Some individuals produce IgE antibodies (reagins) against otherwise harmless antigens. IgE binds to mast cells and basophils. On re-exposure:
- Antigen bridges two IgE molecules → mast cell degranulation
- Release of histamine, leukotrienes (slow-reacting substance of anaphylaxis), bradykinin, prostaglandins
- Clinical manifestations:
- Anaphylaxis — systemic vasodilation, circulatory shock
- Urticaria (hives) — localized skin histamine release
- Hay fever — nasal mucosal swelling and hypersecretion
- Asthma — bronchiolar smooth muscle spasm (mainly from leukotrienes)
10. Sex Differences in Immunity
- Females generally mount stronger innate and adaptive immune responses than males (influenced by sex chromosomes and estrogen/testosterone)
- Greater interferon production, T-cell expansion, and antibody responses in females
- This confers better vaccine responses but also explains why ~80% of autoimmune disease patients are female (e.g., SLE affects women ~10× more than men)
11. Immune Reactions in Transplantation
- Transplanted tissue expresses foreign MHC (HLA) antigens
- Host T cells recognize these → rejection (primarily cell-mediated)
- Prevention strategies: HLA matching, immunosuppressive drugs (corticosteroids, cyclosporine, tacrolimus, azathioprine), sometimes thymic irradiation
— Guyton and Hall Textbook of Medical Physiology (ISBN 9780443111013), Chapter on Resistance of the Body to Infection: Leukocytes, Granulocytes, Monocyte-Macrophage System, and Inflammation; Immunity and Allergy
Routes of administration
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Goodman & Gilman. Let me compile a thorough answer.
Routes of Drug Administration
Source: Goodman & Gilman's The Pharmacological Basis of Therapeutics (ISBN 9781264258079)
Overview
The route of administration determines:
- Rate and extent of absorption (bioavailability, F)
- Onset and duration of drug action
- Whether first-pass metabolism occurs
- Suitability for the drug's physicochemical properties
Bioavailability (F) = fraction of administered dose reaching systemic circulation (0 < F ≤ 1). IV administration gives F = 1 by definition.
1. Enteral Routes (via GI Tract)
Oral (PO)
- Most common, safest, most convenient, most economical
- Absorption governed by: surface area, blood flow, drug solubility, ionization state, GI motility
- Most absorption occurs in the upper small intestine (large surface area ~200 m²) via passive diffusion — even if the drug is ionized there, the surface area advantage dominates over the stomach
- Disadvantages:
- Erratic/incomplete bioavailability (0.05 < F < 1)
- Destruction by gastric acid or digestive enzymes
- First-pass effect — drug absorbed from GI tract passes through the liver before reaching systemic circulation; extensive hepatic/intestinal metabolism can drastically reduce bioavailability (e.g., morphine, nitroglycerin, lidocaine)
- Requires patient cooperation
- Drug interactions with food, other drugs, gut microbiome (>1,000 species)
- Emesis from GI irritation
Factors affecting gastric emptying (faster emptying → faster absorption):
- Recumbent right-side position speeds emptying
- Caloric content, food volume, osmolality slow emptying
- Estrogen slows emptying in premenopausal women
Enteric coating: Protects acid-labile drugs from gastric pH; also used to prevent gastric irritation (e.g., aspirin EC, mesalamine).
Controlled/Extended-release preparations:
- Slow, uniform absorption over 8+ hours
- Benefits: reduced dosing frequency, better compliance, reduced peak-trough fluctuations
- Most suitable for drugs with short t½ (<4 h)
Sublingual (SL)
- Absorbed through oral mucosa directly into systemic venous drainage, bypassing first-pass metabolism
- Rapid onset (e.g., nitroglycerin — onset ~2 min)
- Ideal for drugs with high first-pass extraction orally
- Small surface area limits use to highly potent, lipid-soluble drugs
Rectal (PR)
- ~50% of rectal venous drainage bypasses portal circulation → partial avoidance of first-pass effect
- Useful when oral route unavailable (unconscious patient, vomiting, pediatrics)
- Absorption often irregular and incomplete
- Can cause rectal irritation
- Examples: diazepam rectal gel (seizures), suppository antiemetics, analgesics
2. Parenteral Routes (bypassing GI tract)
Intravenous (IV)
- F = 1 (100% bioavailability by definition)
- Immediate onset — useful in emergencies
- Allows precise titration of dose
- Can deliver large volumes, irritating substances (when diluted), and high-molecular-weight proteins/peptides (e.g., biologics, insulin)
- Disadvantages:
- Highest risk of adverse effects (no recall once injected)
- Must inject slowly in most cases
- Not suitable for oily solutions or poorly soluble substances
- Risk of infection, phlebitis, air embolism
Intramuscular (IM)
- F: 0.75–1
- Prompt absorption from aqueous solutions; slow/sustained from repository (depot) preparations (e.g., haloperidol decanoate, medroxyprogesterone)
- Can handle moderate volumes; suitable for oily vehicles and some irritating substances
- Appropriate for self-administration (e.g., insulin, epinephrine autoinjector)
- Disadvantages:
- Pain or necrosis from irritating substances
- Contraindicated during anticoagulant therapy (risk of hematoma)
- Can elevate creatine kinase (confounds cardiac enzyme interpretation)
Subcutaneous (SC/SQ)
- F: 0.75–1
- Prompt from aqueous solutions; slow/sustained from implants or repository preparations
- Suitable for poorly soluble suspensions (e.g., insulin suspensions) and slow-release implants (e.g., etonogestrel contraceptive implant)
- Not suitable for large volumes
- Less risk of vascular injury than IM
Intra-arterial
- Delivers drug to specific tissue/organ with high local concentration before systemic dilution
- Used in cancer chemotherapy (e.g., hepatic artery infusion) and diagnostic contrast injection
- Requires great caution — inadvertent injection can cause severe ischemia
Intrathecal / Epidural
- Direct delivery to the cerebrospinal fluid (CSF) or epidural space, bypassing the blood-brain barrier (BBB)
- Used for: spinal anesthesia, intrathecal chemotherapy (e.g., methotrexate), opioid analgesia, baclofen pump
- Allows lower doses with reduced systemic effects
Intraosseous (IO)
- Emergency vascular access into bone marrow cavity when IV access unavailable
- Comparable drug kinetics to IV; used in pediatric resuscitation and adult emergencies
3. Topical / Local Routes
Transdermal
- Systemic absorption through skin; bypasses first-pass metabolism
- Rate-limited by skin permeability
- Suitable for lipid-soluble drugs with low required doses
- Provides sustained, steady plasma levels (e.g., fentanyl patch, nicotine patch, nitroglycerin patch, estradiol patch, scopolamine)
- Patches: controlled by membrane or drug-in-adhesive systems
Inhalation
- Rapid absorption via large alveolar surface area (~70 m²) and rich blood supply
- Near-immediate systemic effect (e.g., volatile anesthetics, inhaled bronchodilators)
- Local pulmonary delivery with inhaled corticosteroids (ICS) reduces systemic side effects
- Requires proper inhaler technique; spacer devices improve lung deposition and reduce oropharyngeal deposition
- Adverse effects of ICS: hoarseness, oropharyngeal candidiasis → rinse mouth after use
Topical (Skin/Mucous Membranes)
- Applied locally for local effect (e.g., dermatological creams, eye drops, nasal sprays)
- Minimal systemic absorption desired; however, systemic toxicity possible with overuse (e.g., topical corticosteroids)
Nasal (Intranasal)
- Can be used for local effects (decongestants, corticosteroids) or systemic delivery (e.g., intranasal desmopressin, fentanyl, sumatriptan)
- Avoids first-pass metabolism
- Rapid absorption via nasal mucosa
Ocular, Otic, Vaginal, Urethral
- Primarily local; systemic absorption may occur (e.g., timolol eye drops → bradycardia)
4. Summary Comparison Table
| Route | Bioavailability | Onset | First-Pass | Key Feature |
|---|---|---|---|---|
| IV | F = 1 (100%) | Seconds | None | Most precise; emergency use |
| IM | 0.75–1 | Minutes | None | Depot preparations possible |
| SC | 0.75–1 | Minutes | None | Implants; not large volumes |
| Oral | 0.05–1 | 30–90 min | Yes | Most convenient; variable F |
| Sublingual | High | 1–5 min | Avoided | Potent, lipophilic drugs only |
| Rectal | Partial (~50%) | 5–30 min | Partial | When oral unavailable |
| Transdermal | Variable | Hours | Avoided | Sustained delivery |
| Inhalation | High (pulmonary) | Seconds–min | Avoided | Volatile/aerosolized drugs |
| Intrathecal | 100% (CNS) | Minutes | N/A | Bypasses BBB |
— Goodman & Gilman's The Pharmacological Basis of Therapeutics (ISBN 9781264258079), Chapter 2: Pharmacokinetics
Spectrophotometer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, illustrated answer.
Spectrophotometer
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods (ISBN 9780323673204); Tietz Textbook of Laboratory Medicine, 7th Edition (ISBN 9780323775724)
Definition
Photometry = measurement of light intensity. Spectrophotometry = measurement of light intensity at selected wavelengths. It is one of the most widely used methods of quantitative and qualitative analysis in clinical and biological sciences, exploiting the light-absorbing properties of a substance (or its derivative) to determine its concentration.
Basic Optical Principle
When a beam of light of intensity I₀ passes through a solution containing an absorbing substance (chromogen):
- A fraction is absorbed by the solute
- The remainder is transmitted as Iₛ
Transmittance (T):
T = Iₛ / I₀
To eliminate contributions from the cuvette and solvent, a reference blank (identical solvent without analyte) is used. The instrument is zeroed against the blank, then the sample is measured.
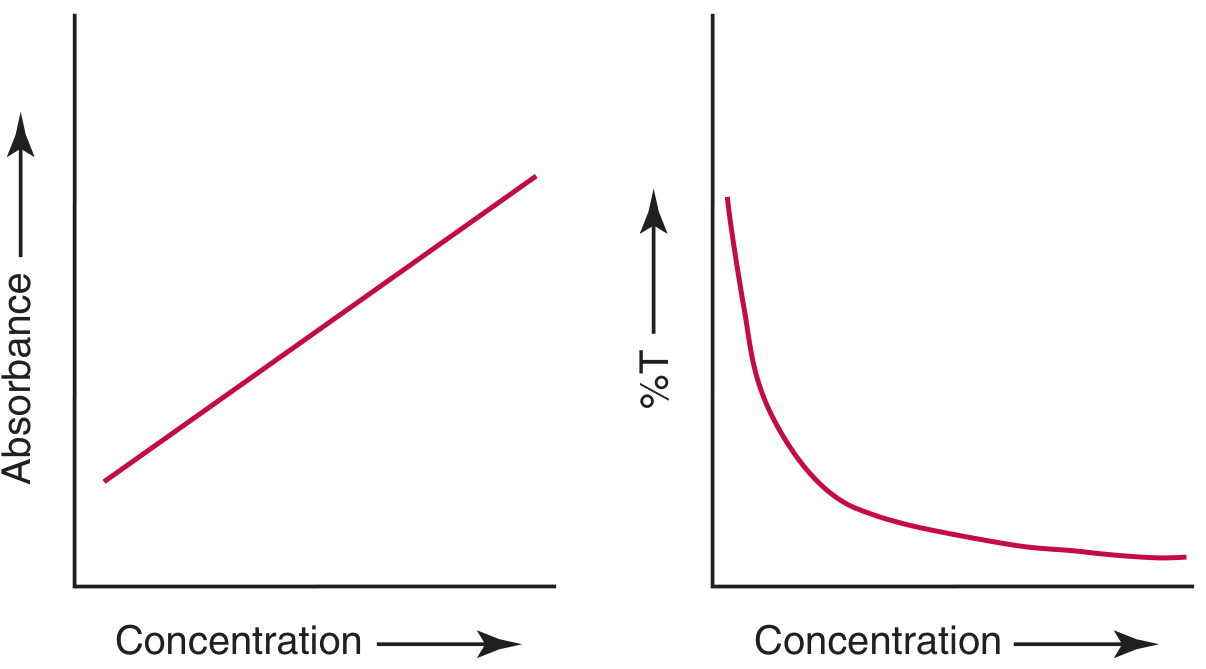
As concentration increases, transmittance decreases logarithmically while absorbance (A) increases linearly:
A = −log T
Beer-Lambert Law
The fundamental quantitative law of spectrophotometry:
A = a · b · c
| Symbol | Meaning |
|---|---|
| A | Absorbance (dimensionless) |
| a | Absorptivity (proportionality constant; units depend on c) |
| b | Path length (cm) — typically 1 cm |
| c | Concentration of analyte (g/L or mol/L) |
When b = 1 cm and c is in mol/L, then a = ε = molar absorptivity (units: L·mol⁻¹·cm⁻¹)
Key points:
- Beer's law holds only over a linear range — calibrators must not exceed this range
- The law is valid at a single, fixed wavelength; polychromatic light causes deviation
- Best measurement at λ_max (wavelength of maximum absorption) for greatest sensitivity
Clinical example: Bilirubin in chloroform at 453 nm has ε = 60,700 cm⁻¹M⁻¹. A 5 mg/L solution gives A = 0.520 at 1 cm path length.
Components of a Spectrophotometer
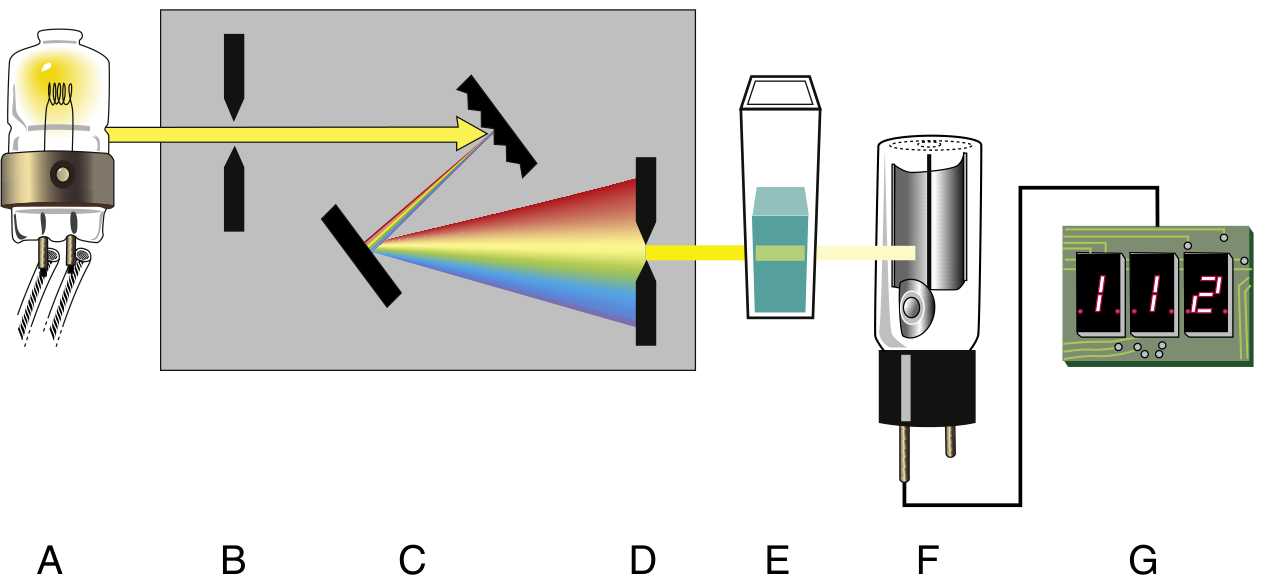
1. Radiant Energy Source (Light Source)
Provides polychromatic light. Two types:
- Continuum sources (emit radiation continuously over a range):
- Tungsten/tungsten-halogen lamp — visible region (380–780 nm); halogen gas prevents filament vaporization, giving brighter/whiter light
- Deuterium lamp — UV region (~190–380 nm); ~100 V applied excites atoms to emit UV photons
- Xenon arc lamp — covers both UV and visible; high-pressure discharge; pulsed output
- Line sources (emit discrete wavelengths):
- Mercury/sodium vapor lamps — sharp lines in UV/visible
- Hollow cathode lamp — used in atomic absorption spectroscopy; metal-specific
- Laser — extremely narrow bandwidth, high intensity; used in high-resolution spectroscopy, nephelometry, MALDI-MS
2. Wavelength Selector (Monochromator)
Isolates a narrow band of wavelengths from the polychromatic source. Types:
- Filters (simple photometers):
- Absorption filters — broad bandpass; transmit a range of wavelengths
- Interference filters — narrow bandpass (~2–10 nm); preferred for greater specificity
- Prisms — disperse light by refraction; less commonly used
- Diffraction gratings — disperse light by diffraction; most widely used in modern spectrophotometers; provide uniform dispersion across the spectrum
- Holographic gratings — laser-etched, superior to ruled gratings; minimal stray light
Spectral bandwidth = range of wavelengths passed at half-peak transmittance. Narrower bandwidth → greater wavelength resolution and reduced stray light.
3. Sample Holder (Cuvette)
- Holds the solution to be measured
- Must be optically clear at the wavelength used:
- Glass — suitable for visible light
- Quartz/fused silica — required for UV measurements
- Path length is standardized at 1 cm for most clinical work
4. Photodetector
Converts transmitted light into an electrical signal:
-
Photomultiplier tube (PMT) — most sensitive and widely used:
- Contains a photocathode + 10–15 dynodes in a vacuum tube
- Photons hit photocathode → emit electrons → cascade amplification at dynodes → 10⁵ to 10⁷ electrons per photon
- ~1,500 V applied; extremely rapid response; sensitive to stray light (must be shielded)
- Dark current = residual current in the absence of light (noise)
-
Photodiodes — solid-state (silicon, GaAs, etc.); detect 250–1,100 nm; more durable
-
Photodiode array (PDA) — multiple diodes detecting different wavelengths simultaneously; allows full-spectrum capture in one measurement (1–2 nm resolution per diode)
-
Charge-coupled device (CCD) and charge-injection device (CID) — two-dimensional arrays; read entire wavelength range at once; CCD reads row-by-row destructively; CID reads each pixel independently and non-destructively
5. Signal Processor
- Amplifies, rectifies, filters, and mathematically transforms the electrical signal
- Performs operations: log conversion (T → A), integration, differentiation
6. Readout Device
- Digital meters, LED displays, LCD screens, X-Y recorders, computer interfaces
Single-Beam vs. Double-Beam Configuration
| Feature | Single-Beam | Double-Beam |
|---|---|---|
| Design | One light path through sample | Beam split: one through reference, one through sample simultaneously |
| Reference correction | Manual (blank measured separately) | Automatic, continuous |
| Drift compensation | Poor | Excellent |
| Typical use | Routine clinical assays | Research, spectral scanning |
Spectrophotometry Nomenclature (Tietz Table)
| Name | Symbol | Definition |
|---|---|---|
| Absorbance | A | −log T |
| Absorptivity | a | A/bc (c in g/L) |
| Molar absorptivity | ε | A/bc (c in mol/L) |
| Path length | b | Internal cell length, cm |
| Transmittance | T | I_transmitted / I_incident |
| Wavelength unit | nm | 10⁻⁹ m |
| Absorption maximum | λ_max | Wavelength of maximum absorption |
Types of Photometric Instruments (Spectrum of Complexity)
| Instrument | Wavelength Selector | Detector | Notes |
|---|---|---|---|
| Colorimeter | Human eye | Eye | Compares colour visually |
| Filter photometer | Absorption/interference filter | Photodiode | Simple, robust, routine use |
| Spectrophotometer | Prism or diffraction grating | PMT or PDA | Precise wavelength selection |
| Spectrofluorometer | Two monochromators (excitation + emission) | PMT | For fluorescent compounds |
| Atomic absorption spectrophotometer | Grating + hollow cathode lamp | PMT | Trace metal analysis |
Quality Assurance in Spectrophotometry
Parameters monitored periodically per regulatory/accrediting standards:
- Wavelength accuracy — verified using didymium glass (broad peak ~600 nm) or holmium oxide (sharp peak at 360 nm)
- Photometric (absorbance) accuracy — measured using glass filters or solutions of known absorbance
- Linearity — ability to yield a linear A vs. concentration relationship (Beer's law range); evaluated by slope and intercept
- Stray light — any light reaching the detector that does not originate from the monochromator; assessed using cutoff filters; causes positive error at high absorbances
Sources of Error / Deviations from Beer's Law
| Cause | Effect |
|---|---|
| Polychromatic light (wide bandpass) | Apparent non-linearity at high A |
| Stray light | Flattening of calibration curve at high concentrations |
| Turbid/scattering samples | Falsely elevated absorbance |
| Fluorescent analytes | Falsely elevated readings |
| Temperature variation | Shifts λ_max; changes absorptivity |
| Cuvette misalignment or scratches | Random error |
| Chemical deviation (ionic interactions, polymerization) | Non-linearity at high concentrations |
— Henry's Clinical Diagnosis and Management by Laboratory Methods (ISBN 9780323673204), Chapter 4; Tietz Textbook of Laboratory Medicine 7th ed. (ISBN 9780323775724), Chapter 16
Histology of tonsils
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.