Constipation management
Reading File
Finding Sources
Searching PubMed
"constipation" AND "management"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have sufficient, comprehensive content to write a thorough answer. Let me compile everything.
Constipation Management
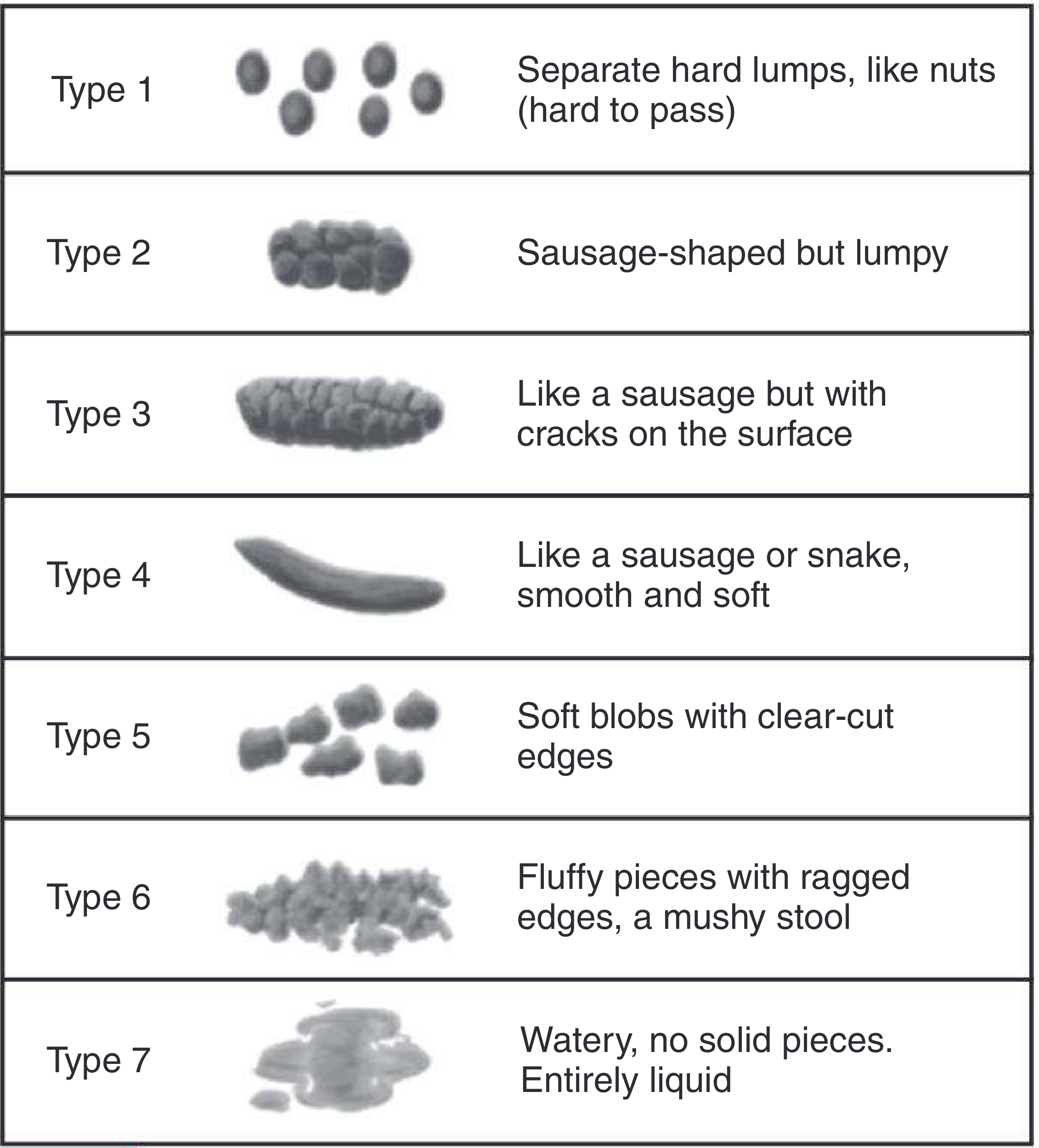
Bristol Stool Form Scale
Types 1-2 indicate constipation. The goal of treatment is stools resembling Types 3-4.
Definition & Pathophysiology
Patients define constipation not just as decreased frequency, but also as difficulty initiating defecation, passage of firm or small-volume feces, or a sensation of incomplete evacuation. Up to 60% of patients presenting with constipation actually have normal colonic transit - they either have IBS or define constipation in non-frequency terms. In the remainder, the problem is either:
-
Delayed colonic transit - defect in colonic motility
-
Outlet disorder - dysfunction of the rectoanal neuromuscular apparatus
-
Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1728
Secondary / Reversible Causes to Exclude
- Low dietary fiber intake
- Medications: opioids, anticholinergics, CCBs, iron supplements, antacids (calcium/aluminum)
- Hormonal: hypothyroidism, hyperparathyroidism, diabetes
- Neurogenic: Parkinson's, spinal cord lesions, Hirschsprung's disease
- Systemic illness: scleroderma, amyloidosis
Step 1: Non-Pharmacologic Measures (First-Line)
Most guidelines recommend these as primary measures:
-
Dietary fiber: 20-35 g/day - fruits, vegetables, whole grains
-
Adequate fluid intake
-
Physical activity
-
Bowel habit training: regular toilet time, positive reinforcement (especially in children)
-
Review and reduce constipating medications where possible
-
Goodman & Gilman's, p. 1732-1734
Step 2: Pharmacologic Management
A. Osmotic Laxatives (First-Line)
Current evidence supports osmotic or stimulant laxatives as first treatment strategies in functional and chronic constipation.
| Agent | Mechanism | Dose / Notes |
|---|---|---|
| Polyethylene glycol (PEG/Macrogol) | Non-absorbable polymer; retains water osmotically | 17 g in 8 oz water/juice daily; first-line for both disimpaction and maintenance |
| Lactulose | Synthetic disaccharide; hydrolyzed by colonic bacteria to short-chain fatty acids, draws water osmotically | 15-30 mL at night; effects in 24-48 h; best alternative if PEG unavailable |
| Sorbitol | Similar to lactulose; equally efficacious | 15-30 mL of 70% solution |
| Magnesium citrate / Mg hydroxide | Osmotic + stimulates CCK release | 4 mL/kg/day; use with caution in renal insufficiency or cardiac disease |
| Sodium phosphate | Osmotic enema | Avoid in children <2 yrs; risk of acute nephropathy |
- Harriet Lane Handbook, 23rd ed., p. 423 | Goodman & Gilman's, p. 1843-1844
B. Stimulant (Irritant) Laxatives
Recommended when patients do not respond to osmotic laxatives. They act directly on enterocytes, enteric neurons, and smooth muscle to promote water/electrolyte accumulation and stimulate motility.
| Agent | Notes |
|---|---|
| Bisacodyl (diphenylmethane) | Oral, suppository, or enema. Marketed as enteric-coated tablets (avoid with antacids/milk - premature dissolution). 1-2 suppositories/day |
| Senna (anthraquinone) | Oral. Frequently used; 2 tbsp at bedtime for opioid-induced constipation prevention |
| Ricinoleic acid (castor oil) | Anthraquinone derivative; rarely used in modern practice |
Use at lowest effective dose for the shortest period necessary. Chronic overuse can cause electrolyte loss, secondary aldosteronism, steatorrhea, protein-losing enteropathy, and osteomalacia.
- Goodman & Gilman's, p. 1855-1858
C. Stool Softeners / Emollients
| Agent | Mechanism | Notes |
|---|---|---|
| Docusate sodium (100 mg twice daily) | Anionic surfactant; lowers stool surface tension, allows aqueous/fatty mixing | Well tolerated but marginal efficacy in chronic constipation; not first-line |
| Mineral oil | Softens/lubricates stool; interferes with water reabsorption | Risk: impairs fat-soluble vitamin absorption, lipid pneumonitis if aspirated, foreign-body reactions. Avoid in infants and at bedtime |
- Goodman & Gilman's, p. 1850-1852
D. Bulk-Forming Agents
| Agent | Notes |
|---|---|
| Psyllium, methylcellulose, polycarbophil | Increase stool bulk and water content. Require adequate fluid intake to avoid obstruction. Useful adjuncts but generally not first-line for established constipation |
Note: Bulk-forming laxatives should be avoided in chronic intestinal pseudo-obstruction (CIPO) as they increase the load on an already dysmotile colon. - Yamada's Gastroenterology, 7th ed.
E. Secretagogues (for Refractory/Chronic Constipation)
| Agent | Mechanism | Use |
|---|---|---|
| Lubiprostone | Activates ClC-2 chloride channels in intestinal epithelium; increases fluid secretion | Chronic idiopathic constipation; opioid-induced constipation unresponsive to standard laxatives |
| Linaclotide / Plecanatide | Guanylate cyclase-C agonists; stimulate intestinal secretion and transit | Chronic idiopathic constipation and IBS-C |
F. Prokinetics
| Agent | Use |
|---|---|
| Prucalopride (5-HT4 agonist) | Chronic constipation refractory to laxatives; particularly useful in chronic intestinal pseudo-obstruction |
Opioid-Induced Constipation (OIC)
Nearly all patients on opioids develop constipation. Prevention is the preferred strategy - do not wait for constipation to develop.
First-line prevention:
- Bulk-forming agents: psyllium 1 tbsp daily
- Osmotic laxatives: PEG 1 tbsp daily
- Stimulant laxatives: senna 2 tbsp at bedtime
Refractory OIC:
-
Methylnaltrexone (peripherally restricted mu-opioid antagonist) - reverses OIC without affecting central analgesia; causes laxation within 24 h in placebo-controlled trials
-
Naloxegol - similar peripherally limited opioid antagonist
-
Lubiprostone
-
Harrison's Principles of Internal Medicine, 22nd ed., p. 465 | Goodman & Gilman's, p. 497
Special Populations
Pediatric (Harriet Lane Handbook, 23rd ed.)
Disimpaction:
- Oral/NG: PEG - 1 to 1.5 g/kg/day for 3 days (>3 years); or magnesium citrate
- Rectal: Saline or mineral oil enemas
- Infants (<1 year): Glycerin suppositories; 2-4 oz of 100% prune or pear juice. PEG used off-label. Avoid mineral oil, stimulant laxatives, phosphate enemas
Maintenance therapy (3-12 months):
- Daily PEG (first-line)
- Lactulose as second-line
- Stimulant laxatives and stool softeners as adjuncts
- Evidence does not support probiotics
- Dietary: increased fruits, vegetables, whole grains, fluids (limit cow's milk)
- Behavioral: regular toilet schedule with positive reinforcement; mental health referral if encopresis is a concern
- Discontinue therapy gradually only after return of regular bowel movements with good evacuation
Geriatric
- Osmotic laxatives (PEG, lactulose, sorbitol) are safe and effective
- Avoid sodium phosphate enemas (electrolyte/renal risk)
- Review polypharmacy as the primary driver
Renal Impairment
- Avoid magnesium-containing preparations (Mg toxicity)
- Avoid sodium phosphate (acute nephropathy)
- PEG is safe
Home Cleanout Protocol (Harriet Lane, Box 12.1)
- Take a stimulant laxative (bisacodyl or senna) with 8 oz liquid per dosing instructions
- Drink PEG mixed with water or clear non-carbonated liquid - full amount over 2 hours
- 1-2 hours after finishing PEG, expect passage of formed/thick brown stool progressing to thinner, clearer stool
Red Flags Warranting Investigation
Constipation with any of these warrants further workup (colonoscopy, imaging, anorectal manometry):
- Rectal bleeding / haematochezia
- Weight loss, anorexia
- Iron-deficiency anemia
- New onset in patients >50 years
- Family history of colorectal cancer
- Failure to respond to 4-6 weeks of laxatives
- Suspected outlet disorder (prolonged straining, incomplete evacuation, need for manual maneuvers)
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th ed. | Harriet Lane Handbook, 23rd ed. (Johns Hopkins) | Harrison's Principles of Internal Medicine, 22nd ed. (2025)
This is a shared conversation. Sign in to Orris to start your own chat.