Management of a case of snakebite in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
snakebite management antivenom treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative sources. Here is the complete, detailed management guide:
Management of Snakebite - Comprehensive Clinical Guide
1. Epidemiology and Background
Snakebite is the deadliest neglected tropical disease in the world. Global data from 2019 estimate 63,415 deaths from snake envenomation annually, with a projected rise to ~68,800 by 2030 despite WHO goals to halve mortality. There are an estimated 1.2-5.5 million snakebites worldwide each year, with 421,000-1,200,000 envenomations. The majority occur in developing countries, especially in agricultural and fishing communities in tropical and subtropical climates. Most victims are young males, with up to 60% of bites occurring in individuals who were deliberately provoking the snake.
- Harrison's Principles of Internal Medicine, 22nd Ed.
2. Classification of Venomous Snakes
| Family | Key Species | Venom Type |
|---|---|---|
| Viperidae - Crotalinae (pit vipers) | Rattlesnakes, copperheads, water moccasins, Asian pit vipers | Cytotoxic, hemotoxic |
| Viperidae - Viperinae (true vipers) | Russell's viper, saw-scaled viper, puff adder | Cytotoxic, hemotoxic |
| Elapidae | Cobras, kraits, mambas, coral snakes, sea snakes, Australian species | Neurotoxic |
| Lamprophiidae (Atractaspidinae) | Burrowing asps | Cardiotoxic |
| Colubridae | Rear-fanged colubrids | Mostly mild |
"Dry bites" - approximately 20-25% of pit viper bites and up to 75% of sea snake bites release no venom. All bites must initially be treated as potentially venomous until ruled out.
India's "Big Four": Russell's viper (Daboia russelii), common krait (Bungarus caeruleus), Indian cobra (Naja naja), and saw-scaled viper (Echis carinatus) account for the majority of snakebite deaths on the subcontinent.
3. Pathophysiology of Venom
Crotaline (Pit Viper) Venom
A complex enzyme mixture causing:
- Local tissue injury via proteolytic enzymes, collagenase, elastase
- Vascular damage - increased permeability, plasma extravasation, hypovolemia
- Hematologic effects - fibrinogenolysis, platelet consumption, coagulopathy/DIC
- Hemolysis via phospholipase A2
- Neurotoxicity (in some species) - blocks neuromuscular transmission causing ptosis, respiratory failure
Elapid Venom
Primarily neurotoxic - pre- and post-synaptic neurotoxins cause:
- Tremor, salivation, dysarthria, diplopia
- Bulbar paralysis, ptosis, fixed pupils
- Dysphagia, dyspnea, respiratory muscle failure
- Cobras additionally cause severe local pain and necrosis
Key Venom Enzymes
Phospholipase A2, hyaluronidase (spreading factor), L-amino acid oxidase, prothrombinase activator, alpha-fibrinogenase, acetylcholinesterase, and collagenase.
- Sabiston Textbook of Surgery, 7th Ed.
4. Grading of Envenomation Severity
| Grade | Features |
|---|---|
| None / Dry bite | Fang marks only, no local or systemic effects |
| Mild | Local findings only - pain, ecchymosis, non-progressive swelling |
| Moderate | Clearly progressive swelling, systemic symptoms/signs, laboratory abnormalities |
| Severe | Neurologic dysfunction, respiratory distress, cardiovascular instability/shock |
- Harrison's Principles of Internal Medicine, 22nd Ed.
5. Field Management (Pre-hospital)
What TO Do
- Rapid transport to a medical facility capable of providing antivenom - this is the single most important step
- Remove all jewelry, watches, tight clothing near the bite site (anticipated swelling)
- Wound care - clean with soap and running water, cover with sterile dressing (but do not delay transport for this)
- Splint the limb to limit movement; maintain at approximately heart level in a neutral position
- Keep the victim calm and still - physical activity disperses venom via muscle pumping
- Photograph the snake from a safe distance to assist identification - do not attempt to catch or handle the snake (reflexive bites from dead snakes can still occur)
- Pressure-immobilization technique - recommended specifically for elapid (neurotoxic) bites: wrap the entire bitten limb firmly (snug but not occlusive - one finger should slip under) at 40-70 mmHg for upper limb and 55-70 mmHg for lower limb; immobilize with a splint; carry the patient out
- Do not wash the wound initially - traces of venom on skin can help identify the species and guide antivenom choice
What NOT to Do
-
No incision and suction - exacerbates local tissue damage, increases infection risk, shown to be ineffective
-
No tourniquet for viper bites - viper venom contains procoagulant enzymes; tourniquet concentrates them in a confined space, and release causes sudden venom bolus and risk of embolism
-
No ice/cryotherapy - worsens ischemia
-
No electric shock - ineffective and harmful
-
No traditional/herbal remedies - cause dangerous delays in reaching definitive care
-
Harrison's Principles of Internal Medicine, 22nd Ed.; P.C. Dikshit Textbook of Forensic Medicine and Toxicology
6. Hospital Assessment
History
- Time and location of bite
- Description of snake (color, size, pattern, head shape)
- Symptoms since bite - pain, swelling, paresthesia, weakness, nausea, visual changes
- First-aid measures already applied
- Patient's medical history, medications, allergies (especially equine proteins for older antivenom)
Physical Examination
- Vital signs - BP, HR, RR, temperature, O2 saturation continuously monitored
- Bite wound - fang marks (number, pattern, depth), local swelling, ecchymosis, blistering, necrosis
- Limb circumference - measure every 15 minutes proximal to the bite site until swelling stabilizes, then every 1 hour
- Neurological - ptosis, diplopia, dysarthria, muscle weakness, altered consciousness
- Cardiovascular - hypotension, arrhythmia
- Respiratory - signs of respiratory muscle compromise
Initial Investigations
| Test | Rationale |
|---|---|
| CBC with differential | Leukocytosis, thrombocytopenia |
| PT/INR, PTT | Coagulopathy/DIC |
| Fibrinogen, fibrin degradation products | Consumptive coagulopathy |
| Metabolic panel (electrolytes, BUN, creatinine) | AKI (common with Russell's viper) |
| Serum CK | Rhabdomyolysis |
| Blood type and cross-match | Anticipate transfusion |
| Urinalysis + urine myoglobin | Hemoglobinuria, myoglobinuria |
| ECG (>50 years or cardiac history) | Arrhythmia |
| ABG (if respiratory compromise) | Ventilatory status |
| Repeat CBC + coagulation every 4 hours if normal; every 6 hours after antivenom if abnormal |
- Harrison's Principles of Internal Medicine, 22nd Ed.; Tintinalli's Emergency Medicine, Comprehensive Study Guide
7. Antivenom Therapy
Antivenom is the definitive treatment for snake envenomation. Whenever possible, seek expert poison control consultation regarding species-specific indications and dosing.
Indications for Antivenom
- Progressive local swelling crossing joints or involving more than half the bitten limb
- Any systemic envenomation (coagulopathy, neurotoxicity, cardiovascular instability, shock, respiratory distress)
- Moderate or severe envenomation grade
- Confirmed coral snake envenomation (prophylactic, before symptoms develop, because effects are irreversible once established)
Antivenom Types
Crotalinae (pit vipers):
- CroFab (Crotalidae Polyvalent Immune Fab, Ovine) - purified Fab fragments; starting dose 4-6 vials for moderate, 6 vials for severe
- ANAVIP (Crotalidae Immune F(ab')2, Equine) - starting dose 10 vials; longer half-life (~133 hours vs ~15 hours for CroFab), stored at room temperature, less costly per vial
Elapids:
- Coral snake: Anti-venin (M. fulvius), 3-5 vials IV at first confirmed bite
- Cobras, kraits, others: Species-specific polyvalent antivenoms per regional formulary
Administration Protocol
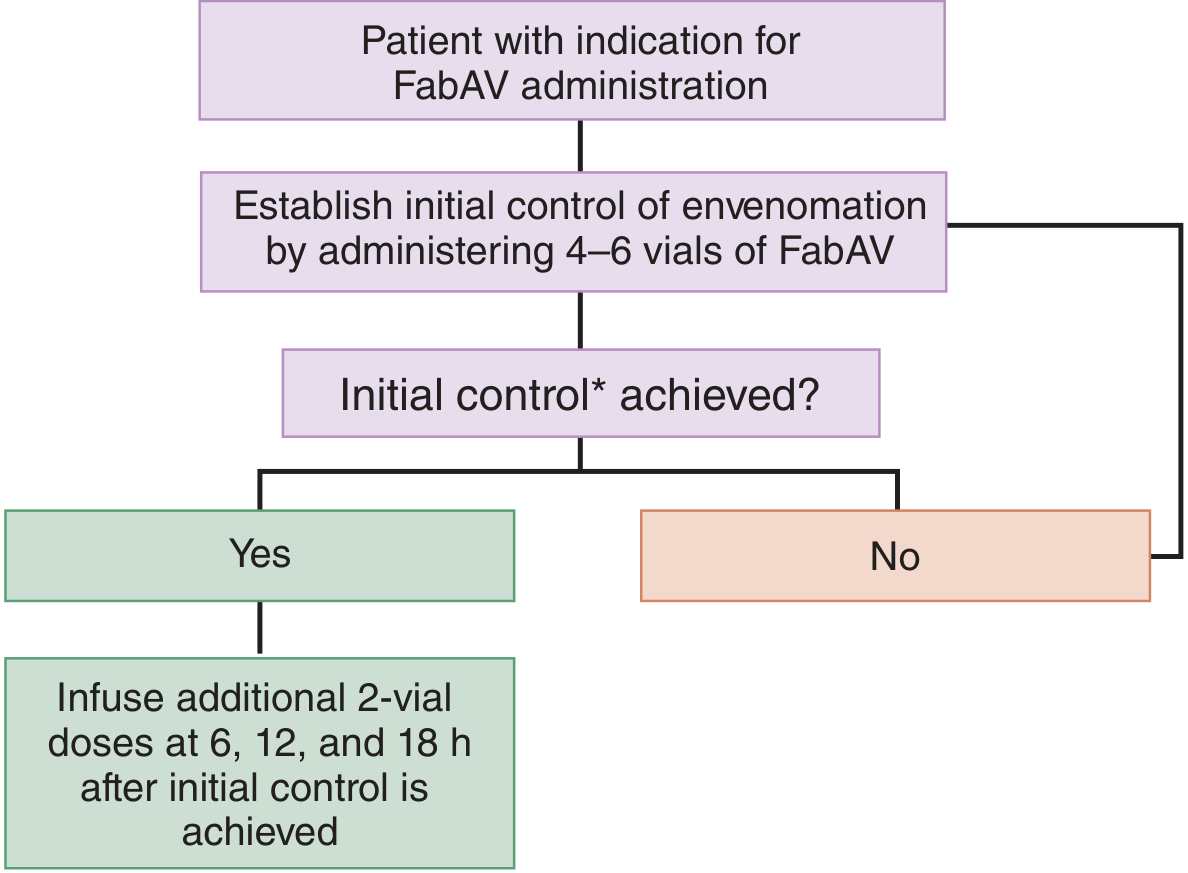
FabAV administration algorithm: Establish initial control with 4-6 vials, then infuse 2-vial maintenance doses at 6, 12, and 18 hours after initial control is achieved. - Tintinalli's Emergency Medicine
- Reconstitute vials and dilute in 250 mL normal saline
- Begin IV infusion at 25-50 mL/h for the first 10 minutes with physician present
- If no reaction, increase to 250 mL/h and complete over 1 hour
- Never give IM or directly into a digit (venom-induced hypovolemia retards absorption; digit injection risks ischemia)
- For FabAV: once initial control is established (cessation of progression of all local effects, systemic effects, coagulopathy), give 2-vial maintenance doses at 6, 12, and 18 hours
- Initial control = cessation of all progression; document initial control carefully - the most common management error is insufficient early dosing
Antivenom Adverse Reactions
| Reaction | Frequency | Management |
|---|---|---|
| Acute allergic/anaphylaxis (CroFab) | 6-14% | Stop infusion; epinephrine IM (IV only for severe hypotension); diphenhydramine IV; methylprednisolone 125 mg IV; airway assessment; fluid resuscitation; restart at 5-10 mL/h when controlled |
| Serum sickness (type III hypersensitivity) | 13-16% (CroFab), less with ANAVIP | Urticaria, arthralgia, nephritis 7-21 days post-infusion; treat with corticosteroids tapered over 7-14 days |
Special populations:
-
Children: same number of vials as adults (children receive proportionally more venom per body mass); may reduce total volume
-
Pregnancy: treat when indicated; coagulopathy can be lethal to mother and fetus; reported fetal loss up to 20% in untreated bites, improved with antivenom
-
Sabiston Textbook of Surgery; Tintinalli's Emergency Medicine; Harrison's 22nd Ed.
8. Supportive Management
Resuscitation
- Establish two large-bore IV lines
- If hypotensive: isotonic crystalloid bolus 20-40 mL/kg IV
- Vasopressors for refractory shock if not responsive to fluids and antivenom
- Supplemental oxygen; be prepared for intubation (particularly in elapid bites causing respiratory failure)
Wound Care
- Clean and dress the wound
- Tetanus prophylaxis as indicated
- Antibiotics only if signs of secondary infection (prophylactic antibiotics are not routinely recommended - snake mouths are not the source of serious infection in typical bites)
Coagulopathy / DIC
- Antivenom is the primary treatment - correct coagulopathy first with antivenom before FFP or platelets
- If severe bleeding despite antivenom: FFP, platelets, cryoprecipitate as needed
- Avoid IM injections until coagulopathy is corrected
Neurotoxic Envenomation (Elapids)
- Monitor serial pulmonary function - inspiratory pressure and vital capacity
- Intensive care monitoring for respiratory depression
- Intubation and mechanical ventilation may be required and prolonged
- Neostigmine + atropine may reverse postsynaptic (not presynaptic) neurotoxicity in some elapid envenomations (e.g., cobras); consult poison control
Acute Kidney Injury
- Monitor urine output closely (especially with Russell's viper envenomation)
- Aggressive IV fluid to maintain urine output >0.5 mL/kg/h
- Hemodialysis for oliguria/anuria not responding to fluids
- Systematic review (PMID: 41776424) confirms AKI as a major complication of snake envenomation requiring early recognition
Rhabdomyolysis
- Aggressive IV hydration
- Forced alkaline diuresis (sodium bicarbonate) to prevent renal tubular damage
- Monitor CK, myoglobin, potassium
9. Compartment Syndrome
Local tissue effects of viper bites can raise compartment pressure. Management is distinct:
| Step | Action |
|---|---|
| 1 | Measure intracompartmental pressure |
| 2 | If <30 mmHg: continue standard management |
| 3 | If signs present + pressure >30 mmHg: elevate limb |
| 4 | Administer mannitol 1-2 g/kg IV over 30 minutes |
| 5 | Simultaneously administer additional antivenom over 60 minutes |
| 6 | If elevated pressure persists 60 minutes later: consider fasciotomy |
The most effective treatment for compartment syndrome from snakebite is neutralization of venom with antivenom, not immediate surgery. Fasciotomy is a last resort.
- Tintinalli's Emergency Medicine
Extensive ecchymosis from severe rattlesnake envenomation (ankle bite, 5 days post):

- Harrison's Principles of Internal Medicine, 22nd Ed.
10. Special Considerations by Snake Type
Viper Bites (Crotalinae and Viperinae)
- Dominant local effects (swelling, hemorrhage, necrosis) + systemic hemotoxicity
- Pressure-immobilization not recommended (may worsen local tissue damage from necrotizing venom)
- Antivenom is the mainstay; dose driven by severity
- Watch for DIC, AKI, compartment syndrome, hypovolemic shock
Elapid Bites (Cobra, Krait, Coral Snake)
- Minimal local effects, predominantly neurotoxic
- Pressure-immobilization technique is appropriate here
- Admit all confirmed bites for observation - symptoms may be delayed hours
- Give antivenom preemptively for confirmed coral snake bite; neurological effects, once established, cannot be reversed
- Prolonged ICU ventilatory support may be needed
- Spitting cobras: ocular venom exposure - irrigate eyes immediately with copious water/saline; ophthalmic review
Sea Snakes (Hydrophiinae - Elapidae)
- Up to 75% dry bites
- True envenomation causes generalized myalgia, trismus, bulbar paralysis, myoglobinuria
- Treat with sea snake antivenom (polyvalent)
11. Criteria for Discharge and Follow-up
Patients are ready for discharge when:
- Swelling begins to resolve
- Coagulopathy has been reversed and remains stable
- Patient is ambulatory
Outpatient instructions:
- Physical therapy for the bitten extremity (especially hand) once swelling and coagulopathy resolve
- Return to ED if symptoms recur, bruising reappears, or signs of recurrent coagulopathy develop
- Educate on symptoms of serum sickness (urticaria, joint pains, fever 7-21 days post-bite) and advise to return
12. What Not to Do - Summary
| Harmful Intervention | Why It Is Harmful |
|---|---|
| Incision and suction | Worsens local damage, increases infection risk, ineffective |
| Tourniquet (viper bites) | Concentrates procoagulant venom; embolic risk on release |
| Ice / cryotherapy | Causes ischemia, worsens necrosis |
| Electric shock therapy | No evidence of benefit; harmful |
| Traditional/herbal healers | Delays definitive care, major contributor to mortality |
| IM antivenom or into digits | Poor absorption, ischemia risk |
| Catching the snake | Risk of second bite; photograph instead |
13. Summary Algorithm
SNAKEBITE
|
v
PREHOSPITAL: Remove jewelry → Clean wound → Splint limb at heart level
Elapid bite? → Pressure-immobilization bandage → Carry (do NOT walk)
Viper bite? → Do NOT use pressure bandage → Rapid transport
|
v
EMERGENCY: ABC assessment → 2 large-bore IVs → O2 → Monitoring
|
v
IDENTIFY: Species if possible, grade severity (none/mild/moderate/severe)
|
v
LABS: CBC, coag, fibrinogen, metabolic, CK, U/A, type & cross
|
v
ANTIVENOM (if moderate/severe/any systemic sign):
Pit viper → CroFab 4-6 vials / ANAVIP 10 vials IV over 1h
Coral snake → Anti-venin (M. fulvius) 3-5 vials IV
Cobra/krait → Regional polyvalent antivenom
|
v
MONITOR: Repeat limb measurements, labs q4-6h
|
v
TREAT COMPLICATIONS:
Shock → Crystalloid bolus ± vasopressors
Coagulopathy → Antivenom first; FFP/platelets if severe bleeding
AKI → IV fluids, dialysis if needed
Compartment → Mannitol + antivenom; fasciotomy last resort
Respiratory failure → Intubation ± ventilator
Neurotoxicity → ICU monitoring; neostigmine for postsynaptic elapid
|
v
DISCHARGE: Stable labs → Ambulatory → Serum sickness education → F/U
Sources
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 471
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Chapter 212
- Sabiston Textbook of Surgery, Biological Basis of Modern Surgical Practice - Chapter 44
- Mulholland and Greenfield's Surgery, Scientific Principles and Practice, 7th Ed.
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology
Recent evidence note: A 2026 systematic review and meta-analysis (PMID: 41776424) confirms AKI as a major complication of snake envenomation across multiple species; early renal monitoring and intervention is supported. A 2025 systematic review (PMID: 40691949) on snakebite outcomes in high-incidence Asian countries highlights the continued burden of delayed presentation and inadequate antivenom access as primary drivers of poor outcomes.
This is a shared conversation. Sign in to Orris to start your own chat.