Hypertension management every details with reasoning ab recently usko kyse treatment dete hain sab Davidsons book se Harrison book se p j Mehta book se sab kitne b books hain sab me treatment alag alag Ho to comparison me samjao
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
hypertension treatment guidelines antihypertensive
Ab mere paas sabhi major books ka content hai. Ek comprehensive, detailed comparison answer likhta hoon Hinglish mein.
Hypertension Management - Complete Textbook Comparison
Kya hai available library mein?
Library mein ye major books hain jo hypertension cover karti hain:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Sabse latest
- Goldman-Cecil Medicine International Edition - Complete reference
- Lippincott Illustrated Reviews: Pharmacology - Drug mechanisms detail mein
- Fuster & Hurst's The Heart, 15th Edition - Cardiology perspective
- Braunwald's Heart Disease - Cardiology specialist text
Note: Davidson's aur P.J. Mehta ki books is library mein available nahi hain. Jo bhi comparison hoga woh upar listed books ke beech hoga - in sab mein Harrison's + Cecil sabse comprehensive hain.
PART 1: DEFINITION aur CLASSIFICATION
Harrison's 22E (2025) ke anusaar:
- Normal BP: <120/80 mmHg
- Elevated: 120-129 / <80 mmHg
- Stage 1 HTN: 130-139 / 80-89 mmHg
- Stage 2 HTN: ≥140/90 mmHg
- Treatment threshold: Zyada tar patients ke liye 130/80 mmHg - kyunki CVD risk 100 mmHg systolic se hi shuru ho jaati hai
Goldman-Cecil Medicine ke anusaar:
BP ko 4 stages mein classify karta hai - Normal (<120/<80), Slightly elevated systolic (120-129/<80), Stage 1 (130-139/80-89), Stage 2 (≥140/≥90), Hypertensive urgency (≥180/>120). Yahan bhi diagnosis confirm karna chahiye multiple visits + ambulatory/home BP monitoring se.
PART 2: LIFESTYLE MODIFICATIONS (Non-Pharmacological Treatment)
Yeh sabse pehla step hai - har book isme agree karti hai.
Goldman-Cecil ke anusaar (Table 64-6):
| Intervention | BP Reduction |
|---|---|
| DASH diet (fruits, vegetables, whole grains, low-fat dairy, nuts) | 7-15 mmHg |
| Dietary sodium restriction <1500 mg/day | Significant |
| Aerobic/resistance exercise 90-150 min/week | Significant |
| Alcohol restriction (men ≤2 drinks/day, women ≤1 drink/day) | 3-4 mmHg |
| Weight loss (overweight patients) | ~1 mmHg per kg |
Reasoning: Lifestyle changes alone 7 se 15 mmHg tak systolic BP kam kar sakti hain. Lekin yeh pharmacological treatment delay karne ke liye zyada effective hain, complete replacement nahi.
Harrison's 22E ke anusaar:
6 key personal exposures pe focus karta hai jo BP raise karte hain:
- Unhealthy diet quality
- Excessive body weight / obesity
- Excessive dietary sodium (almost sabhi adults WHO limit se zyada lete hain)
- Insufficient dietary potassium (potassium heart protective hai - stroke risk kam karta hai)
- Physical inactivity (25%+ U.S. adults koi activity nahi karte)
- Alcohol consumption
PART 3: PHARMACOLOGICAL TREATMENT - FIRST-LINE DRUGS
Yahan sabse interesting comparison hai!
Goldman-Cecil Medicine:
First-Line Drugs - THREE groups:
- Calcium Channel Blockers (CCBs)
- ACE Inhibitors (ACEi) ya Angiotensin Receptor Blockers (ARBs)
- Thiazide or Thiazide-like Diuretics
Guidelines recommend 2 ya zyada drugs se shuru karna for most patients with significant HTN.
Lippincott Pharmacology (Drug mechanism detail):
1. Thiazide Diuretics (Hydrochlorothiazide, Chlorthalidone)
- Mechanism: Shuru mein Na+ aur water excretion badhate hain → intravascular volume kam hota hai → cardiac output aur renal blood flow kam hota hai. Long-term mein peripheral vascular resistance kam karti hain.
- Chlorthalidone preferred over HCTZ (zyada potent, longer acting)
- Contraindication: eGFR <30 mL/min (wahan kaam nahi karte - loop diuretics chahiye)
- Side effects: Hypokalemia, hyperuricemia, hyperglycemia
2. Beta-Blockers (Metoprolol, Atenolol, Nebivolol)
- Mechanism: Cardiac output kam karte hain (heart rate aur contractility ghata ke) + CNS se sympathetic outflow inhibit + renin release kam karte hain → Angiotensin II aur aldosterone bhi kam hota hai
- Selective β1-blockers (metoprolol, atenolol) - asthma patients mein relative contraindication, but non-selective (propranolol) mein absolute contraindication for asthma
- Nebivolol - β1 selective + nitric oxide production badhata hai → peripheral vasodilation bhi
- Use: Especially when concomitant heart disease ya heart failure ho
- Note: Acute heart failure ya peripheral vascular disease mein cautiously use karein
3. ACE Inhibitors (Lisinopril, Enalapril, Ramipril, Perindopril)
- Mechanism: Angiotensin I → Angiotensin II conversion rokta hai → Vasoconstriction nahi hoti, Aldosterone kam nikalta hai, Bradykinin breakdown bhi rokta hai (yahi cough ka reason hai)
- CKD benefits: Glomerular efferent arteriolar vasoconstriction kam karte hain → intraglomerular pressure kam → kidney protection (systemic BP se independent benefit!)
- Side effects: Dry cough (bradykinin se), Angioedema, Hyperkalemia
- Contraindications: Pregnancy (absolute), Bilateral renal artery stenosis, History of angioedema
- Note: ACEi + ARB combination avoid karein (ONTARGET trial evidence - harm)
4. ARBs (Losartan, Valsartan, Telmisartan, Candesartan, Olmesartan)
- Mechanism: Angiotensin II ke AT1 receptor ko block karte hain - same benefits as ACEi but NO cough (bradykinin pathway involved nahi hota)
- Alternative to ACEi when cough ya angioedema ho
- Same contraindications as ACEi for pregnancy aur renal artery stenosis
5. Calcium Channel Blockers (CCBs)
3 classes hain:
| Class | Drug | Action | Special Use |
|---|---|---|---|
| Dihydropyridines | Amlodipine, Nifedipine, Felodipine | Vascular smooth muscle pe kaam - vasodilation | Preferred in Black patients, Diabetes, Stable IHD |
| Benzothiazepines | Diltiazem | Cardiac + vascular effect | Angina, AF |
| Diphenylalkylamines | Verapamil | Negative chrono/dromo/inotropic | Angina, SVT, migraine prevention |
- Warning: Short-acting CCBs (nifedipine immediate release) avoid karein - MI risk increase hota hai
- Dihydropyridines sabse zyada use hote hain hypertension mein kyunki pure vasodilators hain
6. Aliskiren (Direct Renin Inhibitor)
- Mechanism: Renin ko directly inhibit karta hai - RAAS system mein sabse upar kaam karta hai (ACEi/ARB se bhi pehle)
- Combination avoid karein with ACEi ya ARB
- Side effects: Diarrhea, rare cough/angioedema
- Contraindicated in pregnancy, Diabetic patients with ACEi/ARB
PART 4: DRUG SELECTION BY COMORBIDITY (Individualized Therapy)
Yeh Lippincott aur Cecil dono mein detailed diya gaya hai:
| Condition | Preferred Drug | Avoid |
|---|---|---|
| Stable Ischemic Heart Disease | Beta-blocker + ACEi/ARB, CCB | - |
| Heart Failure with reduced EF | ACEi/ARB + Beta-blocker + Aldosterone antagonist | Non-DHP CCBs (Verapamil, Diltiazem), Direct vasodilators |
| Chronic Kidney Disease (CKD) | ACEi or ARB (first choice) | NSAIDS, K+-sparing diuretics cautiously |
| CKD with Diabetes/Proteinuria >1g/24h | ACEi or ARB mandatory, target <130/80 | ACEi + ARB combination |
| Stroke prevention (recurrent) | ACEi + Thiazide combination | - |
| Black Patients | CCB (dihydropyridine) + Thiazide | ACEi/ARB less effective as monotherapy |
| Diabetes | ACEi or ARB preferred | - |
| Pregnancy | Methyldopa, Labetalol, Nifedipine (slow release) | ACEi, ARB, Aliskiren (all absolutely contraindicated) |
| Atrial Fibrillation | Beta-blocker or Verapamil/Diltiazem | Dihydropyridine CCBs alone |
| Primary Aldosteronism | Spironolactone/Eplerenone | - |
| Asthma/COPD | CCB, ACEi/ARB | Non-selective Beta-blockers |
PART 5: BP TARGETS - Books mein kuch differences hain
Yahan major differences milte hain across sources:
Harrison's 22E (2025):
- General population: <130/80 mmHg
- Older adults (≥80 years) - ESC/ESH guideline: BP ≥160 mmHg pe treat karein
- Older adults - American College of Physicians: SBP ≥150 mmHg pe treat karein
- SPRINT trial evidence: SBP <120 mmHg target se CV events kam - but diabetics, stroke history wale, heart failure wale excluded the
- Elderly mein person-centered approach - comorbidities dekhni hain (fall risk, postural hypotension)
Goldman-Cecil:
- General: ≥130/80 mmHg pe treat karein (higher risk individuals)
- Low-risk: ≥140/90 mmHg pe treat karein
- Clinical trial mein <120 mmHg systolic most beneficial, but office target 130/80 mmHg reasonable hai kyunki office BP usually higher hota hai than research settings
Fuster & Hurst's Heart (Cardiology perspective):
- BP control rates suboptimal hain globally - 44% control in 2017-18 (decline from 54% in 2013-14)
- Therapeutic inertia (doctor ka antihypertensive therapy na badhana jab BP high ho) ek major problem hai
- 87% visits mein therapy intensify nahi ki gayi jab BP ≥140/90 tha!
PART 6: RESISTANT HYPERTENSION
Fuster & Hurst aur Cecil dono se:
Resistant Hypertension = BP >140/90 despite 3+ drugs including a diuretic at optimal doses
Causes:
- Pseudoresistance (sabse common) - Poor adherence, White coat effect, Incorrect measurement
- Secondary causes - Primary aldosteronism (11% prevalence in resistant HTN), Sleep apnea, Renal artery stenosis
- Drug interference - NSAIDs, Cocaine, Oral contraceptives, VEGF inhibitors, Cyclosporine
Treatment of Resistant HTN:
- Spironolactone (50-100mg/day) - most effective add-on
- Amiloride
- Renal denervation (catheter-based) - newer option, less evidence
Cecil note: 44,644 patients mein se only 15% ko optimal antihypertensive therapy di gayi thi - iska matlab hai ki most "resistant" hypertension actually undertreated hai
PART 7: SECONDARY HYPERTENSION - Screening aur Treatment
Cecil mein detailed table hai (Table 64-5):
| Cause | Clinical Clue | Test | Treatment |
|---|---|---|---|
| Primary Aldosteronism | Resistant HTN, Hypokalemia, Adrenal adenoma | Plasma renin + aldosterone ratio | Unilateral: Adrenalectomy (cures in 50%+); Bilateral: Spironolactone/Eplerenone |
| Renovascular disease | BP down with ACEi, Flash pulmonary edema, Abdominal bruit | Renal artery duplex, CTA | Angioplasty/Stenting |
| CKD | eGFR <60, Proteinuria | Creatinine, Urine ACR | ACEi/ARB, Salt restriction |
| Coarctation of Aorta | Arm BP > Leg BP, Rib notching | MR angiography | Surgery/Catheter |
| Cushing Syndrome | Central obesity, Striae | Dexamethasone suppression test | Cause-specific |
| Pheochromocytoma | Paroxysmal HTN, Sweating, Pallor | Serum/urine metanephrines | Alpha-blocker first, then Beta-blocker, then surgery |
| Sleep Apnea | Snoring, Daytime sleepiness | Polysomnography | CPAP (modestly lowers BP) |
PART 8: SPECIAL SITUATIONS
CKD mein Hypertension (Harrison's, block 34):
- First line: Salt restriction (maatra limited ho)
- Drug choice: ACEi or ARBs - glomerular efferent arteriolar vasoconstriction kam karte hain (systemic BP se alag benefit!)
- Warning: eGFR <30% baseline drop acceptable hai (intraglomerular pressure kami ka sign)
- K+ monitoring zaruri hai - Patiromer (K+ binder) use kar sakte hain ACEi ke sath
- SGLT2 inhibitors (gliflozins) - new addition, kidney + cardiac protection dono mein
Pregnancy (Harrison's):
- Gestational Hypertension: New-onset ≥20 weeks
- Chronic Hypertension: Pre-existing or <20 weeks diagnosis
- ACEi, ARB, Aliskiren - teratogenic, absolute contraindication
- Safe drugs: Methyldopa, Labetalol, Nifedipine extended-release, Hydralazine
PART 9: DRUG DOSES - Quick Reference (Cecil, Table 64-7)
Thiazide Diuretics:
- Chlorthalidone: 12.5-25 mg/day (preferred over HCTZ)
- Hydrochlorothiazide: 25-50 mg/day
- Indapamide: 1.25-2.5 mg/day
ACE Inhibitors:
- Lisinopril: 10-40 mg/day OD
- Ramipril: 2.5-20 mg/day OD-BD (cardioprotective evidence)
- Enalapril: 5-40 mg/day OD-BD
- Perindopril: 4-16 mg/day OD-BD (stroke prevention - PROGRESS trial)
ARBs:
- Losartan: 25-100 mg/day OD
- Telmisartan: 20-80 mg/day OD (longest half-life)
- Valsartan: 80-320 mg/day OD
- Olmesartan: 20-40 mg/day OD
- Candesartan: 8-32 mg/day OD
CCBs:
- Amlodipine: 2.5-10 mg/day OD (most commonly used DHP)
- Nifedipine CR/XL: 30-90 mg/day OD
- Diltiazem CD: 120-540 mg/day OD
- Verapamil SR: 120-480 mg/day OD-BD
Beta-Blockers:
- Metoprolol succinate (XL): 25-200 mg/day OD
- Atenolol: 25-100 mg/day OD
- Carvedilol: 12.5-50 mg/day BD
- Nebivolol: 5-40 mg/day OD
PART 10: KEY COMPARISON TABLE - Books ke beech differences
| Point | Harrison's 22E (2025) | Goldman-Cecil | Lippincott Pharmacology | Fuster/Hurst's Heart |
|---|---|---|---|---|
| Definition | ≥130/80 mmHg | ≥130/80 mmHg | ≥130/80 mmHg | Same |
| First-line drugs | CCB, ACEi/ARB, Thiazide | CCB, ACEi/ARB, Thiazide (2+ drugs se shuru) | Same 4 classes | Same + emphasizes individualization |
| Beta-blocker status | Not first-line (compelling indication pe) | Not primary first-line | "Treatment option" with cardiac comorbidity | Same |
| BP target (general) | <130/80 | <130/80 (clinical) / <120 ideal | <130/80 | <140/90 most common practice |
| Elderly target | Person-centered (<130 to <150) | <140/90 threshold | Not specifically detailed | Emphasizes undertreatment |
| SGLT2 inhibitors | Mentioned for CKD | Mentioned for CKD | Not in HTN chapter | - |
| Resistant HTN | Mentioned | Very detailed | Not focused | Very detailed (15% undertreated) |
| Focus | Pathophysiology + Clinical | Practical management | Drug mechanisms | Epidemiology + control gaps |
Summary - Sabse important points:
- Pehle lifestyle modification (DASH diet, Na restriction, exercise, weight loss) - sab books agree
- First-line: ACEi/ARB + CCB (amlodipine) + Thiazide-like diuretic (chlorthalidone) - near-universal consensus
- Beta-blockers - first-line se hata diye gaye hain (except compelling indications: IHD, HF, AF)
- Target: <130/80 for most, personalized for elderly
- CKD mein: ACEi/ARB mandatory (dual protection - systemic + renoprotection)
- Black patients mein: CCB + Thiazide preferred (RAAS drugs less effective as monotherapy)
- Pregnancy mein: ACEi/ARB/Aliskiren strictly contraindicated - safe: Methyldopa, Labetalol, Nifedipine SR
- Resistant HTN: Spironolactone add karein + secondary causes exclude karein
Sources: Harrison's Principles of Internal Medicine 22E (2025) - p. 1777-1884; Goldman-Cecil Medicine International Edition - Ch. 64, p. 740-834; Lippincott Illustrated Reviews: Pharmacology - Ch. 8, p. 290-310; Fuster & Hurst's The Heart 15th Ed - p. 226-230
Recent Evidence Update (PubMed 2024-2025): A 2025 Lancet systematic review (PMID: 40902616) found intensive BP control (<120-130 mmHg) reduces cardiovascular outcomes but increases risk of adverse effects like hypotension/syncope. A 2024 Cochrane review (PMID: 39688187) specifically addresses older adults - evidence for higher BP targets (150 mmHg) in frail elderly remains controversial. Yeh Harrison's ki "person-centered approach for elderly" recommendation ko support karta hai.
I want all follow up suggestions
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Ab mere paas comprehensive follow-up data hai - Washington Manual, Katzung's, Harrison's, Cecil sab se. Ab ek full, structured follow-up guide likhta hoon.
Hypertension - Complete Follow-Up Suggestions
(Hypertension ke patient ko kab, kya, aur kaise monitor karein)
SECTION 1: PEHLA DIAGNOSIS KARTE WAQT - Baseline Tests
Washington Manual of Medical Therapeutics ke anusaar, follow-up shuru karne se pehle baseline establish karna zaroori hai:
Routine Lab Tests (Har newly diagnosed HTN patient mein):
| Test | Purpose |
|---|---|
| Urinalysis | Proteinuria, hematuria - renal damage check |
| Serum Creatinine + eGFR | Baseline kidney function |
| Serum Potassium | Baseline - diuretics/ACEi affect karenge |
| Serum Calcium | Hypercalcemia secondary HTN cause ho sakta hai |
| Fasting Blood Glucose + HbA1c | Diabetes coexistence + drug choice guide |
| Fasting Lipid Profile | Global CV risk assessment |
| Uric Acid | Thiazide diuretics hyperuricemia karte hain |
| Hematocrit/CBC | Baseline |
| Serum Sodium | Especially if diuretics start karein |
Imaging / Cardiac Tests:
| Test | When |
|---|---|
| ECG | Har patient - LVH (Left Ventricular Hypertrophy) detect karna |
| Chest X-Ray | Cardiac size, pulmonary congestion |
| Echocardiography | LVH assessment, EF, valvular disease - selective patients mein |
| Ambulatory BP Monitoring (ABPM) | White coat hypertension suspected ho, ya drug resistance evaluate karni ho |
SECTION 2: BP MEASUREMENT - Sahi Technique (Follow-Up ka aadhar)
Washington Manual specifically keh ta hai:
- BP measurements multiple occasions pe leni chahiye, nonstressful circumstances mein:
- Rest ke baad (5 min)
- Sitting position, legs crossed nahi
- Bladder empty
- Comfortable temperature
- Ek reading pe diagnosis mat karo - jab tak BP >180/120 na ho ya target organ damage ho
- 2+ abnormal readings, preferably weeks ke antar mein leni chahiye diagnosis confirm karne ke liye
- Pseudohypertension elderly mein exclude karo - Osler's sign (cuff inflate karne ke baad bhi artery palpable rahe)
Home BP Monitoring encourage karo:
- Home BP readings office se better correlate karte hain target organ damage ke sath
- Ambulatory BP monitoring sabse accurate hai
- BP logs maintain karne se adherence improve hoti hai
SECTION 3: FOLLOW-UP VISIT SCHEDULE
Katzung's Basic & Clinical Pharmacology ke anusaar:
"Follow-up visits should be frequent enough to convince the patient that the physician thinks the illness is serious. With each follow-up visit, the importance of treatment should be reinforced and questions concerning dosing or side effects of medication encouraged."
Recommended Follow-Up Intervals:
| Situation | Follow-Up Interval |
|---|---|
| Stage 1 HTN (130-139/80-89), low risk | Lifestyle changes try karein - recheck 1-3 months mein |
| Stage 2 HTN (≥140/90) | Drug therapy shuru - recheck 1 month mein |
| Stage 2 HTN with target organ damage | More frequent visits - 2-4 weeks |
| New drug started ya dose adjusted | 4-6 weeks mein reassess |
| BP at goal, stable | Har 3-6 months |
| BP well controlled, low risk, stable | Har 6-12 months |
| Drug dose every 1-2 months adjust | Washington Manual - jab tak goal na mile |
SECTION 4: FOLLOW-UP MEIN KYA ASSESS KAREIN
A. Blood Pressure Control Check:
- Goal: <130/80 mmHg for most patients
- Both arms mein check karein (>10 mmHg difference = subclavian/aortic disease suspect)
- Orthostatic BP check karein (elderly, diabetics) - standing BP measure karein 1-3 min baad
B. Target Organ Damage Assessment (Regular):
| Organ | Signs/Symptoms | Test |
|---|---|---|
| Heart | Chest pain, dyspnea, palpitations | ECG (annual), Echo if symptoms |
| Kidney | Edema, decreased urine output | Creatinine, eGFR, Urine ACR (annual) |
| Brain | Headache, TIA symptoms, vision changes | Neurological exam |
| Eyes | Vision blurring | Fundoscopy (ophthalmology referral) - at least once |
| Peripheral Vasculature | Leg pain, claudication | ABI (ankle-brachial index) if suspected |
C. Side Effects of Antihypertensive Drugs:
| Drug Class | What to Monitor |
|---|---|
| ACE Inhibitors | Dry cough (ask specifically), Serum K+, Creatinine, Angioedema |
| ARBs | Serum K+, Creatinine |
| Thiazide Diuretics | K+, Na+, Mg2+, Uric acid, Glucose, Lipids |
| Loop Diuretics | K+, Na+, Ca2+ (hypocalcemia), Volume depletion |
| Beta-Blockers | Heart rate, Fatigue, Dyspnea (asthma aggravation), Glucose (masks hypoglycemia) |
| CCBs (Dihydropyridines) | Ankle edema, Flushing, Reflex tachycardia |
| CCBs (Verapamil/Diltiazem) | Bradycardia, Heart block (ECG), Constipation |
| Spironolactone | Serum K+ (hyperkalemia risk), Gynecomastia |
| Aliskiren | Serum K+, Renal function, Diarrhea |
D. Drug Adherence Check (MOST IMPORTANT):
Katzung ke anusaar, before changing therapy:
- Poor compliance - sabse pehle check karo
- Antagonistic drugs - NSAIDs, decongestants, oral contraceptives, cocaine, amphetamines, VEGF inhibitors, cyclosporine
- High sodium intake - diet history lena
- High alcohol consumption
- Secondary causes - consider karo agar previously effective regimen fail ho jaye
SECTION 5: LABS - Follow-Up Frequency
Recommended Annual Labs:
- Serum Creatinine + eGFR - kidney function, especially ACEi/ARB pe
- Serum Potassium - diuretics, ACEi, ARB all affect K+
- Fasting Glucose / HbA1c - thiazides hyperglycemia karte hain
- Urine Albumin-to-Creatinine Ratio (ACR) - early diabetic/hypertensive nephropathy
- Lipid profile - every 1-3 years (CV risk reassessment)
When to Recheck Labs More Frequently:
- ACEi/ARB shuru karne ke 1-2 weeks baad - creatinine/K+ (especially CKD patients)
- Dose increase ke baad
- Renal function deterioration signs ho
- Spironolactone add karne ke baad - K+ closely monitor karein
SECTION 6: GLOBAL CV RISK REASSESSMENT (Annual)
Goldman-Cecil ke anusaar, follow-up mein sirf BP hi nahi, poora cardiovascular risk reassess karna chahiye:
Use the ASCVD Risk Calculator (http://tools.acc.org/ASCVD-Risk-Estimator):
| Risk Factor | Reassess |
|---|---|
| Smoking status | Every visit |
| Diabetes control (HbA1c) | Every 3-6 months |
| Lipids (LDL, HDL) | Annual / as needed |
| BMI / Weight | Every visit |
| Physical activity level | Every visit |
| Family history update | Annual |
SECTION 7: LIFESTYLE MODIFICATION FOLLOW-UP
Har visit pe reinforce karna chahiye - Washington Manual aur Katzung dono stress karte hain:
| Modification | What to Ask | Target |
|---|---|---|
| Dietary Salt | "Aap roz kitna namak lete ho?" | <1500-2000 mg/day |
| DASH Diet | Fruits, vegetables, low-fat dairy? | Standard DASH |
| Weight | BMI measure karo | Normal BMI or at least 10 kg reduction |
| Exercise | Weekly exercise kitna? | ≥150 min/week aerobic |
| Alcohol | Drinks per week? | Men ≤2/day, Women ≤1/day |
| Smoking | Still smoking? | Complete cessation |
| Stress | Psychosocial stress assessment | Stress management counsel |
| Caffeine | Excess intake? | Moderate |
| Drug use | Cocaine, amphetamines? | Cessation |
SECTION 8: WHEN TO REFER / ESCALATE
Refer to Specialist (Nephrologist/Cardiologist) When:
- Resistant Hypertension - 3+ drugs at maximum doses including a diuretic, BP still uncontrolled
- Secondary Hypertension suspected - young patient, abrupt onset, unprovoked hypokalemia, abdominal bruit, episodic symptoms (pheochromocytoma)
- Target Organ Damage progressive hona - deteriorating kidney function, LV dysfunction
- Hypertensive Emergency/Urgency - BP >180/120 with organ damage
- Pregnancy + Hypertension - obstetric + physician team coordination
- Complex comorbidities - CKD Stage 3+, Severe heart failure, bilateral renal artery stenosis
Emergency (Hospital mein bhejo immediately):
| Condition | BP Level | Features |
|---|---|---|
| Hypertensive Emergency | Usually >180/120 | + Chest pain (MI/Aortic dissection), Stroke symptoms, Acute pulmonary edema, Encephalopathy, Retinal hemorrhage |
| Hypertensive Urgency | >180/120 | No acute organ damage - oral meds se controlled kar sakte |
| Hypertensive Encephalopathy | Very high BP | Confusion, seizures, papilledema |
SECTION 9: MEDICATION ADJUSTMENT PROTOCOL
Washington Manual: Dose ko every 1-2 months adjust karo jab tak goal na mile.
Step-by-step approach:
Step 1: Lifestyle modification trial (1-3 months) - Stage 1, low-risk
↓ (if not controlled)
Step 2: Start 1st drug (ACEi/ARB or CCB or Thiazide)
↓ (4-6 weeks follow-up - goal mile ya nahi?)
Step 3: If partial response - dose increase OR
If no response - switch class OR
Add 2nd drug from different class
↓ (4-6 weeks follow-up)
Step 4: If 2 drugs fail - add 3rd drug
↓
Step 5: If 3 drugs fail including diuretic = Resistant HTN
→ Add Spironolactone
→ Secondary causes workup
→ Specialist referral
SECTION 10: PATIENT EDUCATION - Follow-Up mein Kya Batayein
Katzung specifically keh ta hai - education is ESSENTIAL:
- Disease ka natural history batao - hypertension silent killer hai, symptoms nahi hote
- Treatment adherence ki importance - "Jab tak BP normal hai tab bhi dawai band mat karo"
- Drug side effects ke baare mein inform karo - cough (ACEi), ankle swelling (CCBs), etc.
- Home BP monitoring sikhao - log maintain karo
- Dosing simplification - OD dosing ke drugs prefer karo compliance ke liye
- Abrubt stoppage avoid karein - Beta-blockers, Clonidine abruptly band karne pe rebound hypertension
- Follow-up visits miss na karein - doctor ko serious dikhana hai disease ke baare mein
- Other CV risk factors control karo - smoking, diabetes, lipids
Summary Table - Follow-Up at a Glance
| Follow-Up Point | Frequency | What to Check |
|---|---|---|
| BP measurement | Every visit | Both arms, orthostatic |
| Weight / BMI | Every visit | Target organ, compliance |
| Side effects review | Every visit | Drug-specific |
| Adherence check | Every visit | Pill count, refills |
| Lifestyle review | Every visit | Salt, exercise, alcohol |
| Basic labs (K+, Cr, Glucose) | 1-2 weeks after new drug, then annually | Drug toxicity |
| Urine ACR | Annual | Renal damage |
| Lipid profile | Annual / every 2-3 years | Global CV risk |
| ECG | Annual or if symptoms | LVH, arrhythmia |
| ASCVD risk score | Annual | Treatment decisions |
| Fundoscopy | At diagnosis, then annually | Hypertensive retinopathy |
| Secondary cause workup | If resistant / red flags | Aldosterone, renin, renal imaging |
Sources: The Washington Manual of Medical Therapeutics - Ch. 3, p. 77-89; Katzung's Basic & Clinical Pharmacology 16th Ed. - Ch. 11, p. 290-292; Goldman-Cecil Medicine - Ch. 64; Harrison's Principles 22E; Fuster & Hurst's The Heart 15th Ed.
Pitting and non pitting edema
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent! Bahut comprehensive content aa gaya hai sab books se. Ab ek full structured answer likhta hoon.
Pitting aur Non-Pitting Edema - Complete Guide
Pehle Samjho: Edema Hota Kya Hai?
Edema = Tissues mein fluid ka abnormal accumulation - jab capillaries se fluid interstitial space mein zyada nikle aur lymphatics usse drain na kar paayein.
Normal balance (Starling Forces):
- Capillary hydrostatic pressure → fluid bahar dhakelta hai
- Plasma oncotic pressure (albumin se) → fluid andar kheechta hai
- Thoda excess fluid lymphatics drain karte hain
- Jab yeh balance bigad jaaye → EDEMA
CORE DIFFERENCE: Pitting vs Non-Pitting
| Feature | Pitting Edema | Non-Pitting Edema |
|---|---|---|
| Definition | Finger se press karo → "Pit" (gadda) banta hai aur slowly bhar ta hai | Finger se press karo → koi pit nahi banta |
| Mechanism | Protein-poor fluid (transudate) interstitium mein - easily displaced hoti hai | Proteins / glycosaminoglycans / fibrous tissue deposit ho jaate hain - fluid move nahi hota |
| Nature of fluid | Watery, protein-poor transudate | Thick, protein-rich / mucopolysaccharide laden |
| Common causes | Heart failure, CKD, Nephrotic syndrome, Cirrhosis, Venous insufficiency | Lymphedema (late), Myxedema (Hypothyroidism), Pretibial myxedema (Graves') |
PATHOPHYSIOLOGY - 4 Mechanisms
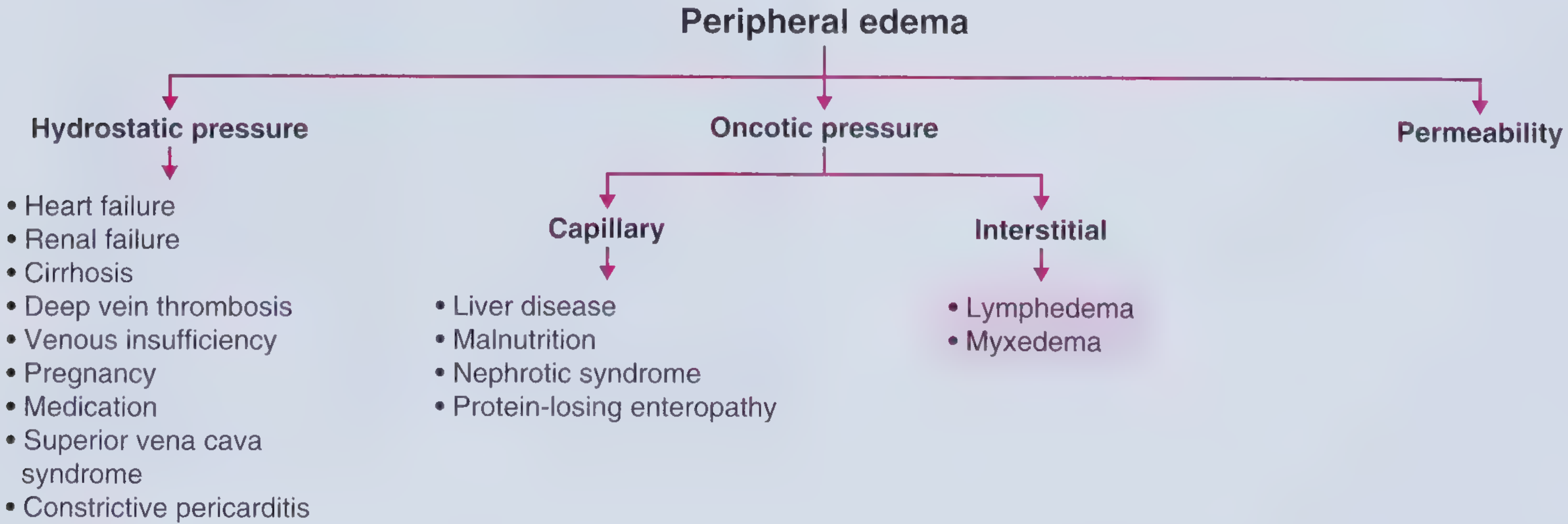
(Diagram from Frameworks for Internal Medicine - sabhi 4 mechanisms dikhata hai)
Mechanism 1: ↑ Hydrostatic Pressure (PITTING edema)
Venous pressure badhta hai → capillary se fluid bahar → interstitium mein jama
Causes:
- Heart Failure - venous congestion from impaired pumping
- Renal Failure - Na+ aur water retention
- Cirrhosis / Ascites - portal hypertension
- DVT - local venous obstruction
- Venous Insufficiency - incompetent valves
- Pregnancy - IVC aur iliac vein compression
- SVC Syndrome - face, neck, arms pe edema
- Constrictive Pericarditis - elevated JVP + Kussmaul's sign
- Prolonged dependency / inactivity - gravity effect
Mechanism 2: ↓ Capillary Oncotic Pressure (PITTING edema)
Albumin kam hota hai → oncotic pull kam → fluid interstitium mein jaata hai
Robbins Pathology ke anusaar: "Albumin accounts for almost half of total plasma protein; conditions leading to inadequate synthesis or increased loss are common causes of reduced plasma oncotic pressure."
Causes:
| Cause | Mechanism |
|---|---|
| Nephrotic Syndrome | Proteinuria ≥3.5g/day → albumin loss in urine |
| Liver Cirrhosis | Liver kam albumin synthesize karta hai (normal: ~15g/day) |
| Malnutrition / Kwashiorkor | Insufficient protein intake |
| Protein-losing Enteropathy | GI tract se protein leak |
Note: Nephrotic syndrome ka edema - bilateral, dependent, pitting, generalized hota hai.
Mechanism 3: ↑ Interstitial Oncotic Pressure (NON-PITTING edema)
Interstitium mein protein-rich fluid ya mucopolysaccharides jam jaate hain → fluid wapas capillary mein nahi jaata
Causes:
- Lymphedema - protein-rich fluid interstitium mein accumulate hoti hai
- Myxedema (Hypothyroidism) - glycosaminoglycans jama hote hain
- Pretibial Myxedema (Graves' disease) - pretibial region, bilateral asymmetric, peau d'orange appearance
Mechanism 4: ↑ Capillary Permeability (PITTING ya NON-PITTING dono)
Capillary membrane damage → proteins leak out → oncotic gradient kam
Causes:
- Local inflammation - cytokine release
- Preeclampsia - HTN + proteinuria + edema in 35th week pregnancy
- Angioedema - ACE inhibitor se (tongue, lips, hands swelling)
- Burns
- Allergic reactions
- Sepsis - diffuse capillary leak
PITTING EDEMA - Detail mein
Grading (Clinical):
| Grade | Description |
|---|---|
| 1+ | Barely palpable pit; disappears rapidly |
| 2+ | Deeper pit (~4mm); disappears in 15 seconds |
| 3+ | Deep pit (~6mm); may last >1 minute; obvious swelling |
| 4+ | Very deep pit (>8mm); lasts 2-5 min; severe, frank swelling |
Major Causes with Characteristics:
Heart Failure:
- Bilateral, symmetric, dependent, pitting
- Gradual onset
- Lower extremities, presacral (bed-ridden patients mein)
- Ascites bhi possible (right heart failure mein)
- Pulmonary edema + pleural effusion left heart failure mein
- Associated: Elevated JVP, S3, Crackles
- Treatment: Diuretics (furosemide/torsemide), salt + fluid restriction
Nephrotic Syndrome (Frameworks for Internal Medicine):
- Typically generalized, dependent, pitting
- Periorbital edema bhi ho sakta hai (especially subah)
- Associated: Proteinuria ≥3.5g/day, hypoalbuminemia, hyperlipidemia
- Urine: Protein +++ but bland sediment (no RBC casts typically)
Cirrhosis:
- Bilateral, symmetric, dependent, pitting
- Gradual onset
- Lower extremities + Ascites (ascites usually more prominent than edema)
- Associated: Spider angiomata, gynecomastia, normal/low JVP, splenomegaly
- Terry's nails (white opacification of most nail bed, narrow pink band distally)
DVT:
- Unilateral, dependent, pitting, ACUTE onset
- Pain + erythema associated
- Treatment: Anticoagulation + compression stockings
Venous Insufficiency (Chronic):
- Bilateral (mostly) or asymmetric
- Soft, pitting EARLY - but may become indurated/non-pitting later
- Dependent, gradual onset
- Associated: Varicosities, hemosiderosis (skin darkening), ulcers near medial malleoli
- Treatment: Compression stockings (first-line)
Renal Failure:
- Similar to right-sided heart failure
- Bilateral, symmetric, dependent, pitting
- Treatment: Dietary Na restriction + dialysis (hemodialysis/peritoneal)
Drug-Induced Edema:
Most common drugs (Frameworks for Internal Medicine):
- Dihydropyridine CCBs (amlodipine) - most common
- Direct vasodilators (hydralazine, minoxidil)
- NSAIDs
- Thiazolidinediones (pioglitazone) - ek important cause
- Corticosteroids
- Estrogen/progesterone hormones
- MAO inhibitors
- Beta-blockers
NON-PITTING EDEMA - Detail mein
1. Lymphedema
Types:
| Type | Onset | Cause |
|---|---|---|
| Primary | Congenital / puberty (Lymphedema Praecox) / after age 20 (Lymphedema Tarda) | Idiopathic, often bilateral |
| Secondary (more common) | Any age | Usually UNILATERAL |
Secondary Causes:
- Malignancy (most common in industrialized world) - lymphoma, breast cancer
- Infection - Filariasis (Wuchereria bancrofti - most common worldwide)
- Surgery - Post-mastectomy lymphedema
- Radiation therapy
- Recurrent lymphangitis, TB
Characteristics (Frameworks for Internal Medicine):
- Localized, dependent, NON-PITTING
- Pitting occurs EARLY in disease course - but over time becomes non-pitting
- Skin becomes thickened, darkened, warty projections (lymphostatic verrucosis)
- Ipsilateral side pe
- Treatment: Diuretics USUALLY UNSUCCESSFUL
Lipedema vs Lymphedema:
- Lipedema = fatty substance deposition, not fluid
- Predominantly in women, lower extremities, usually spares feet
- Frequently mistaken for lymphedema
2. Myxedema (Hypothyroidism)
Mechanism: Hypothyroidism → ↑ capillary permeability + ↓ lymphatic clearance → glycosaminoglycans + albumin accumulate in interstitium → non-pitting edema
Characteristics:
- Non-pitting, bilateral
- Most often lower extremities
- Can be generalized - involves nondependent areas: eyelids, face, dorsum of hands
- Associated symptoms: Weight gain, constipation, dry hair, bradycardia, cold intolerance
- Treatment: Thyroxine replacement
3. Pretibial Myxedema (Graves' Dermopathy)
Mechanism: Inflammatory glycosaminoglycan accumulation (Graves' disease - hyperthyroidism mein paradoxically bhi ho sakta hai)
Characteristics:
- Over pretibial region (shin ke upar)
- Bilateral, asymmetric
- NON-DEPENDENT, non-pitting, painless
- Yellow-brown to erythematous nodules and plaques
- Peau d'orange appearance (orange peel texture) in advanced disease
DISTRIBUTION-BASED CLINICAL APPROACH
Symptom to Diagnosis ke anusaar (Clinical Approach Framework):
Step 1: Bilateral ya Unilateral?
Bilateral Leg Edema → SYSTEMIC cause suspect karo first
Unilateral Leg Edema → LOCAL cause (DVT, cellulitis, Baker's cyst)
Localized edema → Burns, Angioedema, Trauma, Cellulitis
Step 2: Bilateral Edema mein - Systemic ya Venous/Lymphatic?
Systemic causes (most common):
- Cardiac → Heart failure (rEF, pEF), Constrictive pericarditis, Pulmonary hypertension
- Hepatic → Cirrhosis
- Renal → Nephrotic syndrome, Advanced CKD
- Hematologic → Severe anemia
- GI → Malnutrition, Protein-losing enteropathy
- Endocrine → Myxedema (hypothyroidism)
- Drugs → CCBs, NSAIDs, Pioglitazone, steroids
Venous/Lymphatic causes:
- Bilateral DVT
- Venous insufficiency
- Primary lymphedema
Step 3: Key Differentiating Features
| Feature | Heart Failure | Cirrhosis | Nephrotic | Hypothyroidism | Lymphedema |
|---|---|---|---|---|---|
| Pitting | Yes | Yes | Yes | No | Early: Yes → Late: No |
| JVP | Elevated | Normal/Low | Normal | Normal | Normal |
| Ascites | Possible | Prominent | Possible | No | No |
| Proteinuria | Mild | No | Massive (≥3.5g) | No | No |
| Albumin | Low (mild) | Very low | Very low | Normal | Normal |
| Dyspnea | Common | Absent | Absent | Absent | Absent |
| Skin changes | Hemosiderin | Spider angiomata | None | Dry skin | Thick, warty |
| JVP + Kussmaul's sign | No | No | No | No | No → Constrictive pericarditis |
INVESTIGATION APPROACH
Basic workup for all edema patients:
| Test | What it finds |
|---|---|
| Urinalysis + Urine ACR/PCR | Nephrotic (protein +++), Renal failure |
| Serum Albumin | Hypoalbuminemia → nephrotic, cirrhosis, malnutrition |
| Serum Creatinine / eGFR | Renal failure |
| LFTs + PT/INR | Liver cirrhosis |
| TSH | Hypothyroidism (myxedema) |
| BNP / NT-proBNP | Heart failure |
| ECG + Echo | Heart failure, constrictive pericarditis |
| Doppler Ultrasound (leg) | DVT |
| Chest X-ray | Pulmonary edema, pleural effusion |
| Lymphoscintigraphy | Lymphedema confirm karna |
| CBC | Anemia (can cause edema) |
TREATMENT APPROACH
| Cause | Treatment |
|---|---|
| Heart Failure | Loop diuretics (furosemide/torsemide) + Salt/fluid restriction + ACEi/ARB/SGLT2i |
| Nephrotic Syndrome | Treat underlying cause + Salt restriction + Loop diuretics |
| Cirrhosis | Spironolactone + Furosemide (100:40 ratio) + Salt restriction + Paracentesis for ascites |
| Renal Failure | Fluid restriction + Dialysis; severe: Ultrafiltration |
| DVT | Anticoagulation + Compression stockings |
| Venous Insufficiency | Compression stockings (first-line) + Leg elevation |
| Lymphedema | Diuretics usually INEFFECTIVE; Manual lymphatic drainage, compression garments |
| Hypothyroid Myxedema | Thyroxine replacement |
| Drug-induced | Stop offending drug (e.g., amlodipine, pioglitazone) |
| Preeclampsia | Antihypertensives, Delivery planning |
Quick Memory Trick - Pitting vs Non-Pitting
PITTING = "DRENCH" → Drain system fail → watery fluid
D - DVT
R - Renal failure
E - (h)Eart failure
N - Nephrotic syndrome
C - Cirrhosis
H - Hypoalbuminemia (malnutrition)
NON-PITTING = "LM" → Lymph & Mucus (glycosaminoglycans)
L - Lymphedema (late stage)
M - Myxedema (Hypothyroidism)
+ Pretibial myxedema (Graves')
Sources: Frameworks for Internal Medicine - p. 307-312; Symptom to Diagnosis 4th Ed. - Ch. 17, p. 323-325; Robbins & Kumar Pathologic Basis of Disease - Ch. 4, p. 116-118; Washington Manual of Medical Therapeutics; Goodman & Gilman's Pharmacological Basis of Therapeutics
Pretibial Myxedema (Graves' disease) - pretibial region, bilateral asymmetric, peau d'orange appearance ?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Ab mere paas 4 major textbooks ka content hai - Fitzpatrick's Dermatology, Harrison's 22E, Goldman-Cecil, aur Andrews' Diseases of Skin. Ek comprehensive answer likhta hoon.
Pretibial Myxedema (Graves' Dermopathy) - Complete Detail
Actual Clinical Image (Fitzpatrick's Dermatology se):

Classic thyroid dermopathy - anterior shins pe hyperkeratotic infiltrated plaques, foot pe nodule bhi (Fitzpatrick's Dermatology)
Naam ki Confusion - Clear Karte Hain
| Old Name | New Preferred Name | Reason |
|---|---|---|
| Pretibial Myxedema | Thyroid Dermopathy / Graves' Dermopathy | Lesions sirf pretibial region tak limited nahi - kahin bhi ho sakti hain. "Myxedema" naam misleading hai kyunki yeh hypothyroidism mein nahi, Graves' (hyperthyroidism) mein hoti hai |
Fitzpatrick's Dermatology (sabse authoritative dermatology text): "The term thyroid dermopathy is used because the lesions can occur at any site on the body, are not limited to the pretibial region, and the name does not suggest myxedema as a cause."
DISEASE kya hai - Ek line mein
Graves' disease mein ek autoimmune skin condition jisme shin (pindli) ki skin pe glycosaminoglycans (mucopolysaccharides) deposit ho jaate hain, non-pitting, indurated, orange-peel texture wali plaques bana kar.
Pathophysiology - Mechanism
Step-by-step samjho:
Graves' Disease
↓
Thyrotropin Receptor Autoantibodies (TRAb) - VERY HIGH levels
↓
TSH Receptor dermal fibroblasts pe expressed hota hai
↓
Autoantibodies TSH receptor se bind karti hain → dermal fibroblasts activate hote hain
↓
Activated fibroblasts → GLYCOSAMINOGLYCANS synthesize karte hain
(mainly Hyaluronic Acid)
↓
Glycosaminoglycans + albumin interstitium mein accumulate hote hain
↓
Interstitial oncotic pressure ↑ → fluid retain hota hai
↓
NON-PITTING edema + skin thickening + peau d'orange texture
Cecil ke anusaar: "Activated dermal fibroblasts that express the TSH receptor are the likely mediators."
Fitzpatrick's ke anusaar: "Autoantibodies that bind the TSHR on fibroblasts are seen and may trigger synthesis of glycosaminoglycans. However, antibodies that bind TSHR on fibroblasts are present in patients without thyroid dermopathy, indicating there are likely other factors involved."
Extra factor: Lower extremity mein dependent edema bhi fibroblast stimulation mein contribute karta hai - isliye shin pe predominance hoti hai.
Biopsy findings (Fitzpatrick's): "Thickened dermis with splayed collagen fibrils and abundant mucin (usually hyaluronic acid) in the interstitial space."
EPIDEMIOLOGY - Kitne patients mein hota hai?
| Source | Prevalence |
|---|---|
| Harrison's 22E | <5% of Graves' disease patients |
| Andrews' Diseases of Skin | 4% of patients who have/had Graves' disease |
| Fitzpatrick's | <1% mein elephantiasic variant |
| Thyroid Acropachy (related condition) | 0.1-1% of Graves' patients |
Harrison's: "Dermopathy occurs almost always in the presence of moderate or severe ophthalmopathy." Cecil: "All patients with Graves' dermopathy have concomitant hyperthyroidism and Graves' ophthalmopathy."
CLINICAL FEATURES - Kitne types hote hain
Morphological Variants (Andrews' & Fitzpatrick's se):
| Variant | Description | Frequency |
|---|---|---|
| Nonpitting plaque (most common) | Indurated, waxy, painless, pink-purple to yellow-brown plaques | Most common |
| Nodular form | Nodules, can be isolated or multiple | Less common |
| Diffuse form | Larger area involvement | Less common |
| Elephantiasic variant | Skin knees se feet tak thick, firm, hyperpigmented, woody edema + nodule formation - disfiguring | <1% - rarest, most severe |
KEY CLINICAL CHARACTERISTICS - Ek jagah par
Location:
- Pretibial region (shin) - most common (anterior + lateral lower leg)
- But can extend to calf, foot dorsum
- Rarely: shoulder, hands, thighs, scalp, forearms (preradial area)
- Andrews' note: ~50% Graves' patients mein forearm (preradial) mucopolysaccharide deposit hota hai clinically apparent nahi hota
Character of Lesion:
- Non-pitting (non-pitting edema)
- Bilateral, asymmetric
- Painless (hallmark)
- Indurated (hard to feel)
- Waxy texture
- Color: Deep pink, purple, orange-violet, yellow-brown to erythematous
- Surface: Peau d'orange (orange peel) appearance - like an orange skin texture
- Over time: Coalesce, thicken, harden
Associated Features (Harrison's):
- Graves' Ophthalmopathy - almost always present (strongest association)
- Thyroid Acropachy - rarely (digital clubbing + periosteal reaction)
- Presence of dermopathy = marker of severity of autoimmune disease
Timing:
- Usually late manifestation of thyroid disease
- Can rarely be the initial finding
- Acropachy usually appears after treatment of hyperthyroidism
GRAVES' DISEASE KI TRIAD (Classic)
GRAVES' DISEASE
/ | \
/ | \
Goiter Ophthalmopathy Dermopathy
(Diffuse) (Exophthalmos) (Pretibial)
Andrews' ke anusaar: "Ophthalmopathy, pretibial myxedema, and thyroid acropachy are findings almost always limited to patients with Graves disease (not other hyperthyroid states)."
Graves' Acropachy - Associated Condition
Yeh bhi sirf Graves' mein hoti hai, <1% patients mein:
- Digital clubbing (fingers)
- Soft tissue swelling of hands and feet
- Periosteal reaction - diaphyseal proliferation in acral bones (metacarpals, phalanges, tibia, fibula, radius, ulna)
- Usually appears after treatment of hyperthyroidism
- X-ray: Lamellar periosteal reaction - pathognomonic
- 80% patients mein smokers (Fitzpatrick's)
- Can mimic: Acromegaly, Pachydermoperiostosis, Pulmonary osteoarthropathy
DIAGNOSIS
Lab Tests:
| Test | Finding in Graves' |
|---|---|
| TSH | LOW / suppressed (most sensitive) |
| Free T4 | Elevated |
| Free T3 | Elevated |
| TRAb (TSH Receptor Antibodies) | Very HIGH - confirms Graves' + predicts dermopathy severity |
| Radioiodine uptake scan | Diffuse high uptake (vs toxic adenoma which is focal) |
Harrison's: "In 2-5% of patients, only T3 is increased (T3 toxicosis)."
Biopsy (when needed):
- Thickened dermis
- Splayed collagen fibrils
- Abundant mucin (hyaluronic acid) - key finding
TREATMENT
1. Underlying Graves' Disease treat karna:
| Option | Details |
|---|---|
| Antithyroid drugs | Methimazole (first-line in most) or Propylthiouracil (PTU - preferred in pregnancy, thyroid storm) |
| Radioactive Iodine (RAI / 131I) | Common definitive treatment; some cases of elephantiasic PTM bhi resolve hua hai after 131I |
| Surgery (Thyroidectomy) | Third option |
| Beta-blocker (Propranolol) | Symptomatic - tremor, tachycardia, sweating |
2. Local Treatment - Pretibial Lesion ke liye:
| Treatment | Evidence |
|---|---|
| High-potency topical corticosteroids under occlusion | First-line for local lesions - most commonly used. Steroid occlusive dressing technique (SODT) |
| Intralesional triamcinolone acetonide | Effective for localized plaques |
| Systemic corticosteroids | May help in severe cases |
| Compression stockings | Useful + safe |
| Complete Decongestive Physiotherapy | Manual lymphatic drainage + bandaging + exercise |
| IVIG (Intravenous Immunoglobulin) | Small series mein improvement reported (skin + eyes + immunologic) |
| Pentoxifylline | Small series mein reported |
| Octreotide | Reported in small numbers |
| Plasmapheresis | Extreme severe cases |
| Cytotoxic drugs | Reported in small numbers (negative reports bhi hain) |
Andrews' note: Elephantiasic form mein low-dose oral steroids dramatic effect dikhaya hai.
IMPORTANT DISTINCTIONS - Exam Point of View
Pretibial Myxedema (Graves') vs Myxedema (Hypothyroidism):
| Feature | Pretibial Myxedema (Graves') | Generalized Myxedema (Hypothyroid) |
|---|---|---|
| Disease | Graves' (HYPER thyroid) | HYPOthyroidism |
| Location | Pretibial (shin) - localized | Generalized - lower extremities, eyelids, face, hands |
| Pitting | NON-pitting | NON-pitting |
| Texture | Peau d'orange, indurated, waxy | Boggy, doughy |
| Color | Orange-pink to violet | Pale, yellowish (carotenemia) |
| Mechanism | TSHRAb → fibroblast → glycosaminoglycan deposit | ↑ capillary permeability + ↓ lymphatic clearance + glycosaminoglycan |
| Ophthalmopathy | Present (Graves' eye disease) | Absent (periorbital puffiness only) |
| TRAb | Very HIGH | Absent |
| TSH | LOW | HIGH |
| Treatment | Antithyroid therapy + topical steroids | Thyroxine replacement |
Summary - Ek Nazar mein
Pretibial Myxedema = Graves' Dermopathy
- Graves' disease mein (<5% patients)
- Almost always + Graves' ophthalmopathy
- TRAb → dermal fibroblasts activate → hyaluronic acid deposit
- Shin pe bilateral, asymmetric, non-pitting, painless, indurated plaques
- Peau d'orange appearance (orange peel texture)
- Pink to purple-violet color
- Biopsy: splayed collagen + abundant mucin
- Treatment: Topical high-potency steroids under occlusion (first-line)
- Elephantiasic variant (<1%) - most severe form
Sources: Fitzpatrick's Dermatology - Ch. 137, p. 2534-2535; Harrison's Principles 22E - Ch. 396, p. 197-198; Goldman-Cecil Medicine - Ch. 207, p. 2439; Andrews' Diseases of the Skin - Ch. 24, p. 581-582
CRP test
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Details
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.