Latest guidelines for management of hypertension in pregnancy
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "pregnancy" AND "management"
Searching the Web
hypertension pregnancy management guidelines 2024 2025 ACOG ISSHP
Reading File
Reading File
Searching PubMed
"hypertensive disorders of pregnancy" AND "antihypertensive"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data. Let me compile the full answer.
Management of Hypertension in Pregnancy
Classification of Hypertensive Disorders
Hypertension in pregnancy is defined as BP ≥140/90 mmHg and is classified into five categories:
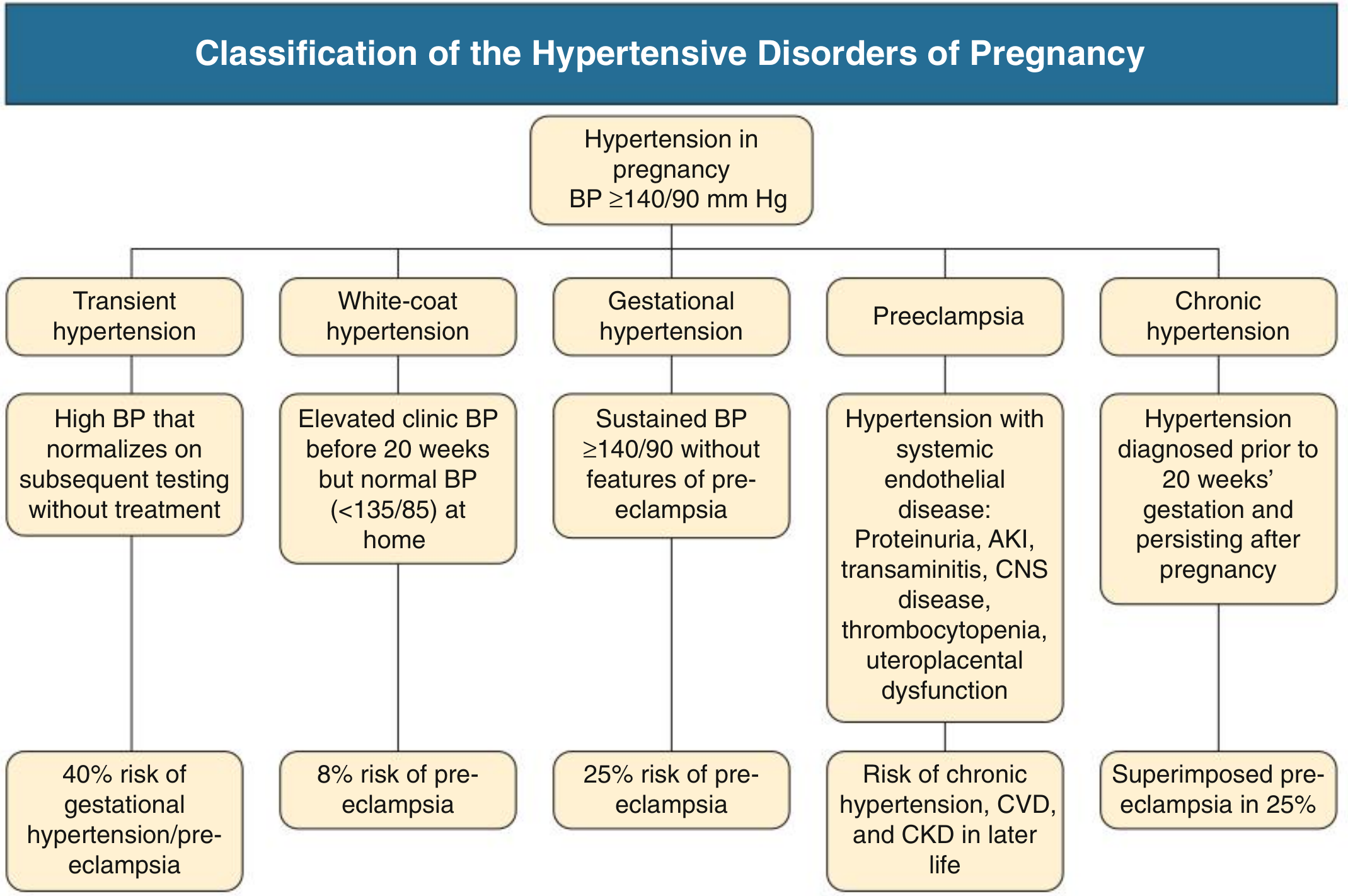
| Category | Definition | Risk |
|---|---|---|
| Transient HTN | BP normalizes on repeat testing without treatment | 40% risk of gestational HTN/preeclampsia |
| White-coat HTN | Office BP ≥140/90, home BP <135/85 | 8% risk of preeclampsia |
| Gestational HTN | New HTN after 20 weeks, no features of preeclampsia | 25% progress to preeclampsia |
| Preeclampsia | New HTN after 20 weeks + organ/uteroplacental dysfunction | CVD, CKD risk in later life |
| Chronic HTN | Present before 20 weeks, persists >12 weeks postpartum | 25% risk of superimposed preeclampsia |
The median BP in normal pregnancy falls to a nadir of 113/69 mmHg at 18-19 weeks and peaks at 121/78 mmHg at term, with an upper reference limit (97th centile) of 136/86 mmHg at midpregnancy and 144/95 mmHg at term.
- Comprehensive Clinical Nephrology, 7th Ed.
Diagnosis of Preeclampsia
Preeclampsia requires new hypertension after 20 weeks with at least one of:
- Proteinuria (uPCR >30 mg/mmol or uACR >8 mg/mmol)
- Acute kidney injury (AKI)
- Elevated transaminases
- Neurological/CNS disturbance
- Thrombocytopenia
- Uteroplacental dysfunction (fetal growth restriction, abnormal umbilical artery Doppler)
Importantly, proteinuria is not required if other features of organ dysfunction are present.
- Comprehensive Clinical Nephrology, 7th Ed.
BP Treatment Thresholds and Targets
When to treat:
- Severe hypertension: SBP ≥160 mmHg or DBP ≥105-110 mmHg - antihypertensive therapy is clearly indicated to prevent maternal stroke and cardiovascular complications.
- Mild-to-moderate HTN (140-159/90-109 mmHg): evidence-base is less clear. Aggressive lowering may impair uteroplacental blood flow and restrict fetal growth without demonstrating clear maternal benefit.
The CHIPS Trial (landmark RCT):
"Tight" BP control (target DBP 85 mmHg) vs. "less-tight" (target DBP 100 mmHg):
- No significant difference in pregnancy loss or need for high-level neonatal care
- "Tight" control significantly reduced severe hypertension (27.5% vs 40.6%), thrombocytopenia, and elevated transaminases
- No increase in small-for-gestational-age infants
This evidence supports a target of DBP 85 mmHg as safe and beneficial. ACOG advises maintaining SBP 120-160 mmHg and DBP 80-105 mmHg.
- Brenner & Rector's The Kidney; Comprehensive Clinical Nephrology
Antihypertensive Drug Therapy
First-Line Oral Agents
| Drug | Notes |
|---|---|
| Methyldopa | Most safety data; centrally acting alpha-2 agonist. Short half-life requires multiple daily dosing. Rare: elevated LFTs, hemolytic anemia |
| Labetalol | Combined alpha/beta blocker - alpha blockade may preserve uteroplacental flow. Available oral and IV |
| Long-acting Nifedipine | Calcium channel blocker; once-daily dosing (slow-release). May cause edema |
Second-Line Agents
| Drug | Notes |
|---|---|
| Hydralazine | Extensive clinical use but increased risk of maternal hypotension and placental abruption with acute IV use |
| Metoprolol | Less safety data than labetalol |
| Verapamil/Diltiazem | No evidence of adverse fetal effects; limited data |
| Clonidine | Comparable to methyldopa but fewer data |
Acute/IV Management (Hypertensive Emergency)
- Labetalol IV: 20 mg, escalate to 40 mg at 10 min if needed
- Hydralazine IV/IM: 5-10 mg, repeat every 20 min
- Nicardipine IV: Extensive safety data (also used as tocolytic)
- Oral nifedipine: also used in acute management
Drugs to Avoid or That Are Contraindicated
| Drug | Reason |
|---|---|
| ACE inhibitors | Multiple fetal anomalies (renal dysgenesis, oligohydramnios, skull ossification defects) - contraindicated |
| ARBs | Same risks as ACE inhibitors - contraindicated |
| Atenolol | Associated with fetal growth restriction |
| Sodium nitroprusside | Risk of fetal cyanide poisoning if used >4 hours |
| Diuretics | May impair pregnancy-associated plasma volume expansion (generally avoided, though no direct fetal toxicity proven) |
| Spironolactone | Theoretical risk of inadequate virilization of male fetuses; eplerenone may be a safer alternative when needed |
- Brenner & Rector's The Kidney; Goodman & Gilman's Pharmacological Basis of Therapeutics
Magnesium Sulfate
For severe preeclampsia or any CNS manifestations (headache, visual disturbance, altered mental status), magnesium sulfate is given as seizure prophylaxis - not for BP control. It is also effective treatment for eclamptic seizures. Approximately 20% of eclampsia episodes occur >48 hours after delivery, so postpartum vigilance is essential.
- Goodman & Gilman's
Prevention of Preeclampsia
In women at high risk (prior preeclampsia, chronic HTN, CKD, antiphospholipid syndrome, diabetes, multifetal pregnancy, first pregnancy, age >40, BMI >30):
- Low-dose aspirin (75-150 mg/day), started before 16 weeks, reduces the risk of preeclampsia by ~10-20%
- Calcium supplementation is recommended in low-calcium-intake populations (reduces risk of preeclampsia by ~50% in calcium-deficient women)
Prepregnancy and Early Pregnancy Assessment (Chronic HTN)
- Evaluate for secondary hypertension (renal artery stenosis, primary hyperaldosteronism, OSA, pheochromocytoma) - present in at least 10% of women with chronic HTN in pregnancy
- Switch to pregnancy-safe antihypertensives before conception
- Counsel on risks: preeclampsia, preterm birth, IUGR
- Consider reducing antihypertensives if BP falls to 130/80 mmHg (common in first/second trimester)
Delivery Timing
- Severe preeclampsia with a mature fetus: delivery is the definitive treatment
- If very preterm: hospitalization, antihypertensives, and MgSO4, with glucocorticoids for fetal lung maturation, to gain time for fetal maturity
- Gestational HTN without features of preeclampsia: delivery typically at 37 weeks
- Chronic HTN without superimposed preeclampsia: individualized, typically 37-39 weeks
Postpartum Management
BP often remains elevated or worsens in the first few days postpartum. Continue antihypertensives. Postpartum diuretics may have a role in reducing BP burden (2025 meta-analysis, PMID 40811831). A 2026 systematic review on postpartum management of HDP (PMID 41421750) confirmed the need for structured follow-up and individualized treatment in the postpartum period.
Recent Evidence Updates (2024-2026)
| Study | Key Finding |
|---|---|
| Oral antihypertensives network meta-analysis, 2025 (PMID 40216176) | Target BP: treat when SBP ≥160 or DBP ≥110 acutely; maintain 140-150/90-100 mmHg; avoid SBP <130 or DBP <80 (may reduce uteroplacental perfusion) |
| Remote BP monitoring meta-analysis, 2025 (PMID 39611763) | Remote/home BP monitoring improves detection and management of HDP |
| ISSHP guidelines update (Pregnancy Hypertens. 2025;13:291-310) | Updated international classification, diagnosis, and management recommendations |
Summary of Key Principles
- Classification matters - treatment approach differs across the 5 categories
- Treat severe HTN promptly (SBP ≥160 or DBP ≥105-110)
- First-line orals: methyldopa, labetalol, or long-acting nifedipine
- ACE inhibitors and ARBs are absolutely contraindicated
- MgSO4 for seizure prophylaxis/treatment in severe preeclampsia/eclampsia
- Low-dose aspirin from <16 weeks in high-risk women
- Delivery is the cure for severe preeclampsia with adequate fetal maturity
- Postpartum monitoring is essential - 20% of eclampsia occurs after delivery
Sources: Brenner & Rector's The Kidney; Comprehensive Clinical Nephrology 7th Ed.; Goodman & Gilman's Pharmacological Basis of Therapeutics; Goodman-Cecil Medicine; ISSHP 2025 Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.