Hey orris, give me bradycardia and bradyarrhythmia in full detail topics for my medicine viva. Of both the topics, don't miss anything. For both the topics, give in full details which I can read it, read it and be prepared for both the topics in all terms without missing anything.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive viva preparation. Let me compile the complete, detailed answer.
BRADYCARDIA & BRADYARRHYTHMIA - Complete Medicine Viva Guide
Sources: Braunwald's Heart Disease 12e, Guyton & Hall Medical Physiology, Rosen's Emergency Medicine, Goldman-Cecil Medicine
PART 1: BRADYCARDIA
1. Definition
- Bradycardia = heart rate < 60 beats/min (clinical/conventional definition)
- Based on large population studies of healthy individuals, the lower limit of normal resting heart rate is actually 50 beats/min (Braunwald's)
- For practical purposes, symptomatic bradycardia is defined as a rate < 50 beats/min with associated symptoms
2. Physiological vs Pathological Bradycardia
| Type | Examples |
|---|---|
| Physiological | Well-conditioned athletes (vagal dominance, increased stroke volume, downregulation of funny current If), sleep, Type I AV block during sleep |
| Pathological | Sick sinus syndrome, AV block, hypothyroidism, drugs, AMI |
Athlete's bradycardia mechanism:
- Increased stroke volume triggers baroreceptor reflex -> increased vagal tone
- Exercise training downregulates ion channels responsible for the "funny current" (If) that drives rhythmic sinus node depolarization (Guyton & Hall)
3. Classification of Bradycardia
Bradycardias are categorized by the level of disturbance in the hierarchy of impulse generation and conduction:
Sinus Node → AV Node → His-Purkinje System
- Sinus node dysfunction - sinus bradycardia, sinus arrest, SA exit block, sick sinus syndrome
- AV nodal block - 1st, 2nd (Mobitz I), 3rd degree at AV node
- Infranodal block - Mobitz II, 2:1 block, complete heart block (His-Purkinje)
4. ECG Recognition of Sinus Bradycardia
- Rate < 50 beats/min (Braunwald's) / < 60 beats/min (conventional)
- P waves are of normal contour, upright in leads I, II, aVF
- Every P wave followed by a QRS complex
- Constant PR interval > 120 ms
- Sinus arrhythmia often coexists

Sinus bradycardia (lead III) - note slow rate with normal P wave morphology
5. Causes of Bradycardia
A. Physiological
- Athletes, vagal stimulation, sleep
B. Increased Vagal Tone (Neurally Mediated)
- Carotid sinus syndrome (hypersensitive baroreceptors - even mild neck pressure causes intense bradycardia, may cause cardiac standstill for 5-10 sec and syncope)
- Vasovagal syncope
- Inferior wall MI (vagal reflex from inferior wall)
- Raised intracranial pressure (Cushing reflex)
- Hemoperitoneum
C. Intrinsic Sinus Node Disease
- Sick sinus syndrome
- Fibrotic degeneration (elderly)
- Cardiomyopathies
- Post-cardiac surgery (Mustard/Senning repair for TGA, ASD repair, Fontan)
D. Drugs
- Beta-blockers (most common drug cause)
- Calcium channel blockers (diltiazem, verapamil)
- Digoxin
- Amiodarone
- Ivabradine
E. Metabolic / Systemic
- Hypothyroidism
- Hypothermia
- Hypoxia
- Hyperkalaemia
- Jaundice (bile salts)
F. Infections / Inflammatory
- Lyme disease (carditis)
- Myocarditis
- Chagas disease
- Rheumatic fever
G. Cardiac
- Acute inferior wall MI (AV nodal ischemia)
- Cardiac amyloidosis
- Sarcoidosis
- Post-cardiac transplant (atropine is ineffective - no vagal innervation)
6. Clinical Features
Symptoms (when heart rate is insufficient for cardiac output):
- Dizziness, lightheadedness
- Syncope or near-syncope (Adams-Stokes attacks in complete heart block)
- Fatigue, exercise intolerance
- Dyspnea (reduced cardiac output)
- Chest pain (if ischemia occurs)
- Cognitive impairment (in elderly)
- Palpitations (escape beats)
Signs:
- Slow pulse (regular or irregular)
- Low BP (if haemodynamically compromised)
- S3 or S4 may be present
- Cannon A waves (complete heart block - atria contracting against closed TV)
- Variable S1 intensity (complete heart block)
7. When Bradycardia Becomes Symptomatic
Rate at which symptoms occur depends on:
- Adequacy of escape rhythms
- Ventricular function
- Associated conditions (ischemia, heart failure)
- Duration and suddenness of onset
Symptomatic bradycardia typically at rates < 40-50 beats/min or with pauses > 3 seconds.
8. Investigation
- 12-lead ECG - identify the type of bradyarrhythmia
- Holter monitoring (24-48 h) - detect intermittent bradycardia
- Event recorder / Implantable loop recorder (ILR) - for infrequent syncope
- Electrophysiology study (EPS) - localise block (A-H = AV node, H-V = His-Purkinje)
- Carotid sinus massage - with ECG, identifies carotid sinus syndrome
- Tilt table test - vasovagal syncope
- Blood tests: TFTs (hypothyroidism), electrolytes (K+), drug levels, Lyme serology
9. Management of Bradycardia
Acute (Emergency) Management
| Drug | Dose | Notes |
|---|---|---|
| Atropine | 0.5-1 mg IV, every 3-5 min, max 3 mg | First-line; ineffective in post-transplant (no vagal innervation); WORSENS infranodal AV block |
| Dopamine | 2-10 mcg/kg/min IV infusion | If atropine fails |
| Epinephrine | 2-10 mcg/min IV infusion | If atropine fails |
| Isoproterenol | 2-10 mcg/min IV infusion | Post-cardiac transplant (drug of choice) |
Atropine is contraindicated / harmful in:
- Infranodal (His-Purkinje) AV block - can paradoxically worsen block
- Wide-complex escape rhythms
- Post-transplant (use isoproterenol)
Temporary Pacing Indications
- Haemodynamically unstable bradycardia not responding to drugs
- Anterior MI with new complete heart block or bifascicular block
- Post-cardiac surgery
- Drug toxicity with complete AV block
- Bridge to permanent pacemaker
Methods:
- Transcutaneous pacing (emergency, uncomfortable, only temporary)
- Transvenous temporary pacing (more reliable, preferred in-hospital)
Permanent Pacemaker (PPM) Indications
- Symptomatic sinus node dysfunction
- Symptomatic AV block (2nd or 3rd degree)
- Post-MI: transient 2nd or 3rd degree AV block with bundle branch block
- Asymptomatic 3rd degree AV block with rate < 40 or pauses > 3 sec
- Chronotropic incompetence
PART 2: BRADYARRHYTHMIAS (Detailed)
1. Classification of Bradyarrhythmias
Bradyarrhythmias fall into two broad groups:
- Disorders of impulse formation (sinus node)
- Disorders of impulse conduction (AV/His-Purkinje)
2. SINUS NODE DYSFUNCTION (SND)
A. Sinus Bradycardia
(Covered in detail above)
B. Sinus Arrest (Sinus Pause)
- Sinus node fails to generate an impulse
- Results in absence of P wave on ECG
- Pause is NOT a multiple of the preceding P-P interval (distinguishes from SA exit block)
- A junctional or ventricular escape beat typically follows
- Causes: vagal stimulation, drugs, sick sinus syndrome
ECG: Absent P wave; pause not a multiple of P-P interval; followed by escape beat
C. Sinoatrial (SA) Exit Block
- Sinus node generates an impulse, but it fails to exit (conduct to the atria)
- Three degrees (analogous to AV block):
- Type I SA exit block (Wenckebach): Progressive shortening of P-P intervals until one P wave is dropped; the cycle length of the pause is < 2x the preceding P-P interval
- Type II SA exit block: Dropped P waves occur in a regular ratio (2:1, 3:1, 4:1) - the pause IS a multiple of the P-P interval
- Type III / Complete SA block: No P waves (indistinguishable from sinus arrest)
- Causes: intrinsic SA node disease, vagal tone, drugs
D. Sinus Arrhythmia
- Normal variation in sinus rate with respiration
- Respiratory sinus arrhythmia: Rate increases on inspiration (inhibition of vagal tone), decreases on expiration
- Variation < 5% in quiet breathing; up to 30% during deep breathing
- Entirely normal - most common in children and young adults
- Non-respiratory sinus arrhythmia: seen with digitalis toxicity
E. Sick Sinus Syndrome (SSS) - "Sinus Node Disease"
Definition: A syndrome encompassing multiple sinus nodal abnormalities, broadly representing failure of the sinus node and surrounding atrial tissue.
Features (may occur individually or in combination):
- Persistent spontaneous sinus bradycardia inappropriate for the physiological circumstance
- Sinus arrest or SA exit block
- Combinations of SA and AV conduction disturbances
- Bradycardia-tachycardia (Tachy-Brady) syndrome - alternating paroxysms of rapid atrial tachyarrhythmias (usually AF, atrial flutter) and periods of slow atrial/ventricular rates
Epidemiology:
- Most common in older adults due to fibrotic degeneration
- Associated with: cardiomyopathies, connective tissue diseases, amyloidosis, sarcoidosis, myocarditis, certain drugs
Tachycardia-Bradycardia Syndrome (TBS) - key concept:
- Post-tachycardia pauses: When the tachyarrhythmia (usually AF) terminates, the suppressed sinus node takes time to recover - resulting in excessive post-conversion pauses
- Also seen when AF alternates with periods of high-grade AV block causing bradycardia
- Commonly precipitated/worsened by beta-blockers or calcium channel blockers used to treat the tachycardia
ECG findings:
- Sinus bradycardia; sinus pauses; SA block
- Post-tachycardia pauses (after AF)
- Escape beats (junctional or ventricular)
- Alternating fast and slow rates on Holter
Diagnosis:
- 24-h Holter (most useful)
- Event recorder / ILR (for infrequent episodes)
- EPS: sinus node recovery time (SNRT) - prolonged (> 1500 ms) is abnormal
- Intrinsic heart rate (IHR) after autonomic blockade - reduced in intrinsic SND
Management:
- Acute: Treat the specific rhythm (atropine for bradycardia, rate control for tachycardia)
- Long-term: Permanent pacemaker for symptomatic bradycardia + pharmacological therapy for the tachyarrhythmia component (note: drugs alone worsen bradycardia)
- Preferred pacemaker mode: AAI or DDD (rate-responsive AAIR/DDDR)
3. AV CONDUCTION DISORDERS (HEART BLOCK)
Definition of AV Block: The atrial impulse is conducted with delay or is not conducted at all to the ventricles when the AV junction is not physiologically refractory.
Sites of block:
- AV node (most common, usually benign)
- His bundle
- Bundle branches (infranodal - more serious)
Key differentiation using His bundle electrogram (EPS):
- A-H interval prolonged = AV nodal block
- H-V interval prolonged = infranodal (His-Purkinje) block
A. First-Degree AV Block
Definition: Every atrial impulse conducts to the ventricles, but with prolonged PR interval > 0.20 sec (200 ms) in adults.
ECG features:
- PR interval > 200 ms (can be as long as 1000 ms!)
- Every P wave is followed by a QRS
- When PR > P-P interval: "skipped P waves" phenomenon
- If QRS is narrow: block is in AV node
- If QRS has BBB pattern: block may be AV nodal OR His-Purkinje (EPS needed)
Causes:
- Normal variant (up to 2% of healthy young adults)
- Increased vagal tone
- Inferior MI
- Drugs (beta-blockers, CCBs, digoxin, amiodarone)
- Myocarditis, Lyme disease
- Rheumatic fever
Clinical significance:
- Usually asymptomatic, benign
- Can progress to higher-degree block if carotid massage applied or if atrial rate increases
- No treatment required; avoid nodal blocking agents
B. Second-Degree AV Block
Definition: Some (but not all) atrial impulses fail to conduct to the ventricles.
The conduction ratio describes the relationship (e.g., 3:2 means 3 P waves : 2 QRS complexes).
Mobitz Type I (Wenckebach) Block
Mechanism: Progressive fatigue of AV nodal conduction - decremental conduction in AV node
ECG features:
- Progressive lengthening of PR interval from beat to beat
- Until one P wave is suddenly blocked (dropped beat) - no QRS
- After the dropped beat, PR interval resets to shortest value and cycle repeats
- R-R intervals progressively shorten before the dropped beat (though the PR lengthens, the increments decrease each beat)
- The pause containing the dropped beat is less than 2x the preceding R-R interval
- Grouped beating (pairs, trios)
Important subtleties:
- The biggest increment in PR is in the 2nd beat of each cycle
- The greatest shortening of R-R is between 2nd and 3rd beat
- "Footprint" pattern on ladder diagram
Location of block: AV node (narrow QRS usually)
Causes: Increased vagal tone, inferior MI (RCA supplies AV node), drugs, myocarditis, after cardiac surgery
Significance: Usually benign (especially during sleep, in athletes, inferior MI); rarely progresses to complete block in isolation
Treatment: Usually none; treat underlying cause; atropine if symptomatic
Mobitz Type II Block
Mechanism: Sudden failure of conduction in the His bundle or bundle branches without prior PR lengthening
ECG features:
- Fixed PR interval (same before and after blocked P)
- Sudden, unexpected dropped beat (no QRS) without preceding PR prolongation
- QRS is usually wide (BBB pattern) - block is infranodal
- May be associated with bundle branch block
Important distinction from Type I:
- PR is constant; no progressive lengthening
- Block is infranodal (His bundle or below)
- More dangerous - higher risk of progression to complete heart block
Causes: Anterior MI (LAD territory - affects bundle branches), fibrosis (Lenegre/Lev disease), cardiomyopathy, surgical trauma to conduction system
Significance: More serious than Mobitz I. Can progress unpredictably to complete heart block. Carries higher mortality.
Treatment: Permanent pacemaker is indicated even if asymptomatic (high risk of sudden complete heart block)
2:1 AV Block
- 2 P waves : 1 QRS (every other P wave blocked)
- Cannot distinguish between Mobitz I and II from a single strip (need longer strips, other clues)
- If QRS is narrow - more likely Mobitz I (AV nodal)
- If QRS is wide - more likely Mobitz II (infranodal)
- Carotid massage worsens Mobitz II (slows atrial rate - less conduction); atropine improves Mobitz I
- Requires further investigation
High-Grade (Advanced) AV Block
- 2 or more consecutive P waves fail to conduct
- e.g., 3:1, 4:1 block
- Implies near-complete failure of AV conduction
- Usually requires pacing
C. Third-Degree (Complete) AV Block
Definition: No atrial impulse conducts to the ventricles - complete AV dissociation.
ECG features:
- P waves and QRS complexes are completely dissociated (P-P interval is regular, R-R interval is regular, but the two bear NO relationship to each other)
- Atrial rate > ventricular rate (always - because escape pacemakers are slower)
- Escape rhythm:
- Junctional (nodal) escape: QRS narrow (< 120 ms), rate 40-60 bpm - block is in AV node (more benign)
- Ventricular escape: QRS wide (> 120 ms), rate 20-40 bpm - block is infranodal (more dangerous, unstable, risk of asystole)
- Variable S1 intensity (AV dissociation - different PR relationships each beat)
- Cannon A waves in JVP (atrial contraction against closed tricuspid valve)
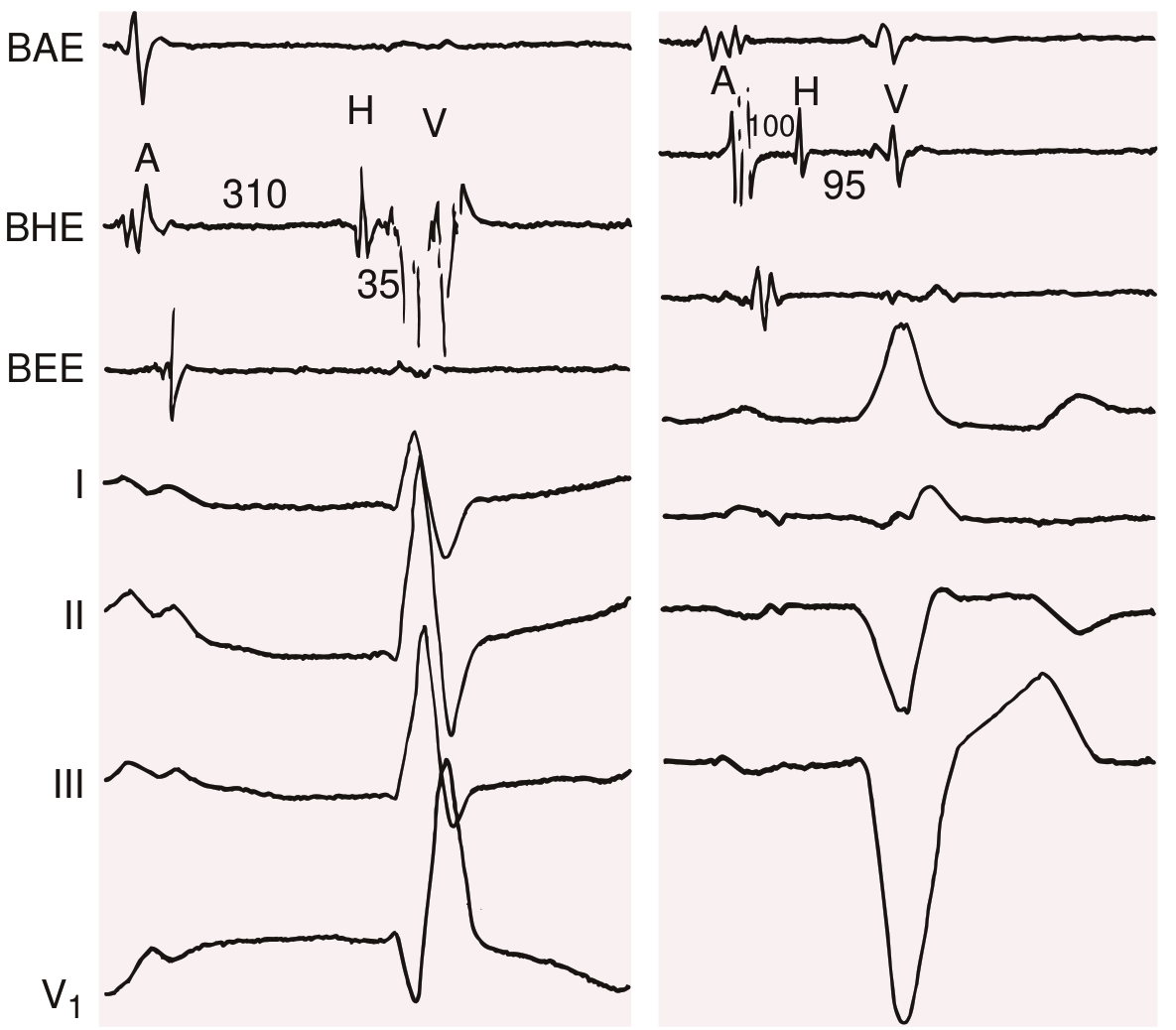
His bundle electrogram showing AV conduction. Left: normal. Right: H-V block (infranodal) - prolonged H-V interval with wide QRS escape
Causes:
- Congenital complete heart block (associated with maternal anti-Ro/La antibodies, corrected TGA)
- Acquired:
- Inferior MI (transient, often nodal - usually recovers)
- Anterior MI (permanent, infranodal - serious)
- Lyme disease (carditis)
- Surgical/catheter trauma
- Drugs (digoxin toxicity, beta-blockers, CCBs)
- Sarcoidosis, amyloidosis
- Fibrocalcific degeneration (Lenegre's/Lev's disease)
- Post-TAVI (transcatheter aortic valve implantation)
Clinical features:
- Adams-Stokes attacks (sudden syncope due to ventricular standstill before escape rhythm kicks in)
- Slow, regular pulse; wide pulse pressure (large stroke volume)
- Cannon A waves in JVP
- Variable S1 intensity
- S4 may be present
- Features of low cardiac output: dyspnea, angina, heart failure
Treatment:
- Acute: Atropine (if nodal block); avoid atropine in infranodal block (can worsen); dopamine/epinephrine infusion; temporary pacing (transcutaneous or transvenous)
- Definitive: Permanent pacemaker (DDD mode preferred in most; rate-responsive DDDR for active patients)
- Post-cardiac transplant: Isoproterenol (atropine is ineffective - no vagal innervation)
4. AV DISSOCIATION
- NOT the same as complete heart block
- AV dissociation = atria and ventricles are driven by independent pacemakers (both independently beating) - but this is because the ventricular pacemaker has ACCELERATED (e.g., junctional tachycardia), not because of block
- In complete heart block: atria faster than ventricles
- In isorhythmic AV dissociation: rates similar
- In AV dissociation from accelerated ventricular rhythm: ventricle faster, captures occur when P waves find the AV node receptive
5. LENEGRE'S DISEASE vs LEV'S DISEASE
| Feature | Lenegre's Disease | Lev's Disease |
|---|---|---|
| Pathology | Primary fibrosis of conduction system | Extrinsic fibrosis/calcification from adjacent structures (aortic/mitral valve, interventricular septum) |
| Age | Younger | Older |
| Mechanism | Idiopathic sclerodegenerative | Extension of valve calcification |
| Result | Progressive bundle branch block -> CHB | CHB |
6. ECG COMPARISON TABLE - Summary
| Arrhythmia | PR Interval | P:QRS Ratio | QRS | Key Feature |
|---|---|---|---|---|
| Sinus bradycardia | Normal constant | 1:1 | Narrow | Rate < 60 (or 50) |
| Sinus arrest | N/A | - | - | Missing P wave, pause not multiple of P-P |
| SA exit block Typ II | Normal | Regular dropped P | Narrow | Pause = multiple of P-P |
| 1st degree AV block | > 200 ms, constant | 1:1 | Usually narrow | Long PR, all conduct |
| Mobitz I (Wenckebach) | Progressive lengthening | Group of P:QRS then dropped | Narrow | PR lengthens then dropped beat |
| Mobitz II | Fixed, normal | Regular dropped P | Wide | Fixed PR, sudden dropped beat |
| 2:1 AV block | Fixed | 2:1 | Narrow/Wide | Every other P blocked |
| Complete AV block | No relationship | P>>QRS | Narrow/Wide | P and QRS completely dissociated |
7. MANAGEMENT ALGORITHM FOR BRADYARRHYTHMIA
BRADYARRHYTHMIA DETECTED
|
Is patient STABLE?
/ \
YES NO
| |
Identify type Emergency:
of bradyarrhythmia Atropine 0.5-1mg IV
| Transcutaneous pacing
|
|---> Sinus bradycardia/SSS
| -> Treat cause, PPM if symptomatic
|
|---> 1st degree AV block
| -> Observe, no treatment
|
|---> Mobitz I (Wenckebach)
| -> Usually observe; PPM if symptomatic
|
|---> Mobitz II
| -> PPM (even if asymptomatic)
|
|---> Complete Heart Block
-> Atropine if nodal, temporary pacing
-> Permanent PPM
8. PACEMAKER BASICS (for Viva)
NBG Pacemaker Code (5-letter):
| Position | Meaning | Common Options |
|---|---|---|
| I | Chamber paced | A (atrium), V (ventricle), D (dual) |
| II | Chamber sensed | A, V, D, O (none) |
| III | Response to sensing | I (inhibit), T (trigger), D (dual), O |
| IV | Rate modulation | R (rate-responsive) |
| V | Multisite pacing | A, V, D, O |
Common modes:
- VVI: Ventricular pacing, ventricular sensing, inhibited - "demand pacing" - used in AF + CHB
- DDD: Dual-chamber, dual-sensing, dual-response - maintains AV synchrony - most physiological
- AAI: Atrial pacing - used in sick sinus syndrome with intact AV conduction
- VVIR/DDDR: Rate-responsive variants for active patients
PPM Indications (ACC/AHA Class I - key ones to know):
- Symptomatic bradycardia (any cause)
- 3rd degree AV block (regardless of symptoms if rate < 40 or pauses > 3 sec)
- Mobitz II AV block (even asymptomatic)
- 2:1 AV block with wide QRS (infranodal)
- Symptomatic chronotropic incompetence
- Post-MI: transient 2nd or 3rd degree AV block with bundle branch block, or persistent symptomatic AV block
9. SPECIAL SCENARIOS (High-Yield Viva Points)
Bradycardia in Acute Inferior MI
- Due to: RCA ischemia affecting AV node (+ increased vagal tone)
- Usually transient and reversible
- Usually nodal (narrow QRS escape)
- Responds to atropine
- Rarely needs pacing
Bradycardia in Acute Anterior MI
- Due to: LAD ischemia affecting bundle branches
- Usually infranodal (wide QRS escape)
- Does NOT respond to atropine (may worsen)
- Carries 4-6x higher in-hospital mortality (marker of extensive myocardial damage)
- Temporary pacing indicated
- Permanent pacing: even if transient 2nd/3rd degree AV block with bundle branch block
Post-Cardiac Transplant Bradycardia
- Denervated heart - no vagal supply
- Atropine is INEFFECTIVE (no muscarinic receptors to block)
- Isoproterenol is drug of choice (direct beta-1 agonist)
- May need pacemaker if persistent
Bradycardia in Lyme Disease
- Lyme carditis: spirochetal invasion of conduction tissue
- Any degree of AV block possible (can fluctuate rapidly)
- Usually temporary and reversible with antibiotics (doxycycline/amoxicillin)
- Monitor closely; temporary pacing for complete heart block
Drug-Induced Bradycardia
- Beta-blockers: Glucagon (0.5-5 mg IV) is specific antidote
- Digoxin toxicity: Digoxin-specific antibody fragments (Digibind/Fab)
- CCBs (verapamil/diltiazem): Calcium gluconate, glucagon, high-dose insulin
Hypersensitive Carotid Sinus Syndrome
- Baroreceptors in carotid sinus are excessively sensitive
- Even light pressure on the neck causes intense vagal discharge
- Can cause cardiac standstill for 5-10 seconds -> syncope
- Diagnosis: carotid sinus massage (with ECG, resuscitation equipment available!)
- Pause > 3 seconds = significant
- Treatment: PPM (DDD or VVI)
10. AUTONOMIC / NEURALLY MEDIATED BRADYCARDIAS
These are an important category:
| Condition | Mechanism | Key Feature |
|---|---|---|
| Vasovagal syncope | Bezold-Jarisch reflex: forceful contraction of underfilled ventricle -> afferent vagal discharge -> bradycardia + vasodilation | Prodrome, young patients, precipitated by standing/pain/fear |
| Carotid sinus hypersensitivity | Excessive baroreceptor sensitivity | Neck pressure causes syncope |
| Situational syncope | Vagal discharge with cough, micturition, defecation, swallowing | History is diagnostic |
| Orthostatic hypotension | Autonomic failure / hypovolemia | BP drops on standing; HR may or may not compensate |
11. KEY DIFFERENTIALS IN VIVA
Q: How do you differentiate Mobitz I from Mobitz II?
- Mobitz I: Progressive PR lengthening + narrow QRS + AV nodal location (benign, inferior MI)
- Mobitz II: Fixed PR + wide QRS + infranodal location + dangerous, needs PPM
Q: What is the risk of Mobitz II?
- Can progress to complete heart block suddenly and unpredictably - risk of syncope and sudden death
Q: Why is atropine contraindicated in infranodal AV block?
- Atropine increases sinus rate; more impulses arrive at the blocked infranodal system -> paradoxically fewer conduct through -> worse bradycardia or asystole
Q: Difference between sinus arrest and SA exit block?
- Sinus arrest: pause is NOT a multiple of P-P interval (node failed to fire)
- SA exit block (Type II): pause IS an exact multiple of P-P interval (node fired but impulse didn't exit)
Q: What is tachycardia-bradycardia syndrome?
- Part of sick sinus syndrome. Post-tachycardia suppression of sinus node -> long pauses after tachycardia terminates. Dangerous because drugs to treat tachycardia worsen bradycardia -> needs PPM + drug therapy
Q: What escape rate suggests block is nodal vs infranodal?
- Junctional escape rate 40-60 bpm (narrow QRS) = nodal block
- Ventricular escape rate 20-40 bpm (wide QRS) = infranodal block (more dangerous)
Q: What investigation is done to localise AV block?
- His bundle electrogram (intracardiac EPS): A-H interval (AV node), H-V interval (His-Purkinje)
Q: What is Stokes-Adams attack?
- Sudden syncope (brief LOC) due to transient cardiac standstill or very slow ventricular rate, classically in complete heart block. Characteristically: sudden fall without warning, rapid recovery, pallor followed by flushing
12. QUICK RECALL: CAUSES OF PROLONGED PR (1st Degree AVB)
Mnemonic - "Drugs And Low Pressure In Hips":
- D - Digoxin, Drugs (beta-blockers, CCBs, amiodarone)
- A - Athletic heart, Autonomic (high vagal tone)
- L - Lyme disease
- P - PR prolongation physiologic (athletes)
- I - Inferior MI, Inflammatory (myocarditis, RF)
- H - Hyperkalaemia, Hypomagnesaemia
- S - Surgery (cardiac)
13. SUMMARY TABLE - Bradyarrhythmias at a Glance
| Arrhythmia | Risk Level | PPM Needed? | Key Drug | Notes |
|---|---|---|---|---|
| Sinus bradycardia | Low | Only if symptomatic | Atropine | Very common, often benign |
| Sick sinus syndrome | Moderate | Yes (symptomatic) | PPM + anti-AF drugs | Tachy-brady syndrome |
| 1st degree AV block | Low | No | None | Benign, observe |
| Mobitz I (Wenckebach) | Low-moderate | Only if symptomatic | Atropine | Nodal, often benign |
| Mobitz II | High | Yes (always) | Temporary pacing | Infranodal, can -> CHB |
| High-grade AV block | High | Yes | Temporary/PPM | Unstable |
| Complete heart block | Very high | Yes (urgent) | Atropine (nodal only), isoprenaline | Stokes-Adams attacks |
Sources: Braunwald's Heart Disease 12e (Chapter 68), Guyton & Hall Medical Physiology (Chapter 13), Rosen's Emergency Medicine 9e (Chapter 65), Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.