
6 year old girl
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Granulosa-Theca Cell Tumor in a 6-Year-Old Girl
This is a classic exam vignette for a Juvenile Granulosa Cell Tumor (JGCT) — a sex cord-stromal tumor of the ovary.
Clinical Scenario Breakdown
| Feature | Significance |
|---|---|
| 6-year-old girl | Pre-pubertal — any signs of puberty are pathological |
| Taller than peers | Excess estrogen → advanced bone age → tall stature initially |
| Breast development + pubic/axillary hair | Isosexual precocious puberty due to estrogen secretion by tumor |
| Abdominal distension + pain | Mass effect from large ovarian tumor |
| Blood at introitus | Estrogen-stimulated vaginal bleeding (uterine stimulation) |
| Abdominal/ovarian mass on USG | Ovarian tumor confirmed |
Diagnosis = Granulosa-Theca Cell Tumor (Juvenile type)
Why This Tumor Causes Precocious Puberty
Granulosa cells are the normal estrogen-producing cells of the ovary. When they form a tumor, they secrete large amounts of estrogen autonomously — independent of the hypothalamic-pituitary axis. This produces:
- Isosexual precocious pseudopuberty (peripheral/GnRH-independent): breast development, pubic/axillary hair, vaginal bleeding
- Advanced bone age → initially tall, but early epiphyseal fusion → ultimately short adult stature
This is pseudoprecocious puberty (not true central precocious puberty), because the HPG axis is not activated — the estrogen comes directly from the tumor.
Histological Features
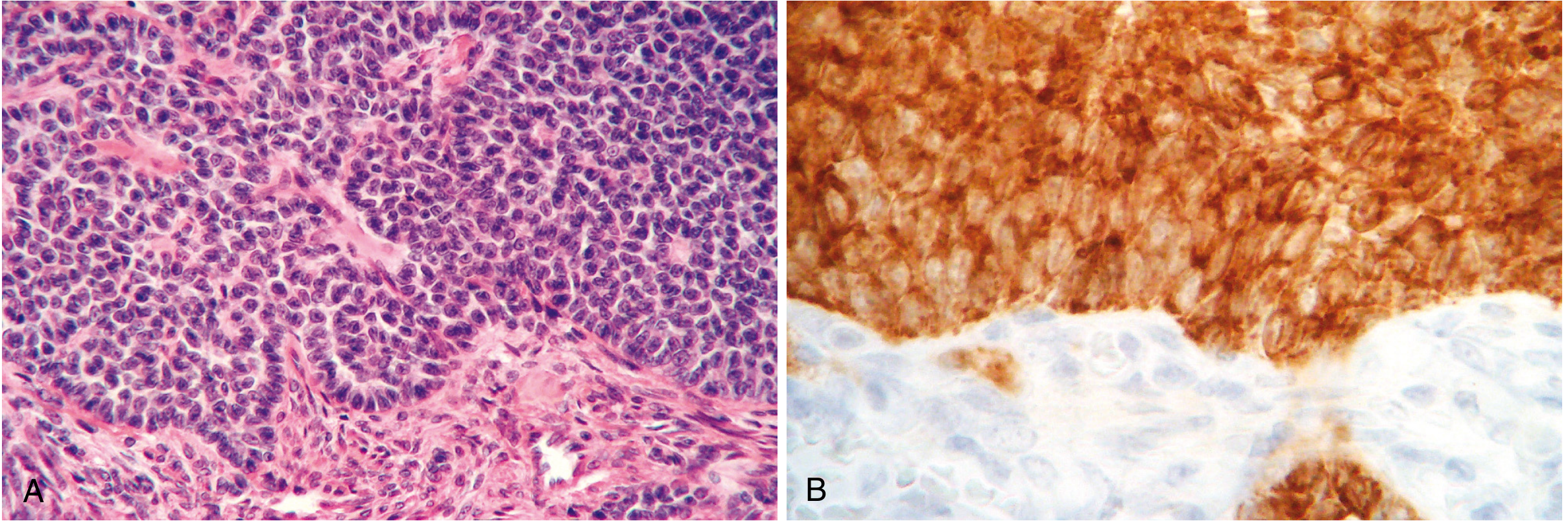
- Call-Exner bodies: Small follicle-like rosettes with acidophilic material — pathognomonic
- "Coffee bean" grooved nuclei (adult type)
- Juvenile type: rounder, more hyperchromatic nuclei, large irregular follicle spaces, numerous mitoses
- Inhibin positive on IHC (tumor marker)
Key Facts for Exams
| Feature | Detail |
|---|---|
| Tumor type | Sex cord-stromal tumor |
| Age group in this scenario | Juvenile (<10 years) |
| Hormone secreted | Estrogen (rarely androgens → virilization) |
| Tumor marker | Inhibin (also Anti-Müllerian hormone) |
| FOXL2 mutation | 97% of adult granulosa cell tumors |
| Juvenile type mutations | AKT1 (60%) and GNAS (30%) |
| Associated syndromes | DICER1 syndrome, Ollier disease, Maffucci syndrome |
| Malignant potential | Low-grade malignant; recurrence 5–25% |
| 10-year survival (Stage I) | ~90–95% |
| Treatment | Surgical removal (unilateral oophorectomy in young girls) |
Distinguishing from Central Precocious Puberty
| Granulosa Cell Tumor | Central Precocious Puberty | |
|---|---|---|
| Mechanism | Peripheral (autonomous estrogen) | Central (GnRH-dependent) |
| GnRH stimulation test | No LH surge | LH surge present |
| Ovarian USG | Mass present | Enlarged ovaries, no mass |
| FSH/LH | Suppressed | Elevated |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 948; Berek & Novak's Gynecology, p. 2399–2400
This is a shared conversation. Sign in to Orris to start your own chat.