Biodegradable implants how are they what r they made of advantages and applications disadvantages and cons indications and novelty explain in detail with appropriate illustrative diagrams
biodegradable implants biomaterials clinical applications
biodegradable implants materials composition advantages disadvantages clinical applications diagram 2024
https://pmc.ncbi.nlm.nih.gov/articles/PMC12462970
biodegradable implant degradation mechanism diagram orthopedic bone fixation stent
Biodegradable Implants - Complete Reference
What Are They?
Material Composition
1. Synthetic Polymers (most common)

| Polymer | Degradation | Time | Best For |
|---|---|---|---|
| PGA (polyglycolic acid) | Hydrolysis of ester bonds | 6-12 weeks | Sutures, short-term fixation |
| PLA (polylactic acid) | Hydrolysis | 1-2 years | Plates, screws, drug delivery |
| PLGA (PLA+PGA copolymer) | Hydrolysis (tunable by ratio) | Weeks to months | FDA-approved, widest use |
| PCL (polycaprolactone) | Hydrolysis (slow) | 2-4 years | Tissue scaffolds, long-release drugs |
| PDS (polydioxanone) | Hydrolysis | ~6 months | Sutures, cardiovascular |
| PEEK | Enzymatic/surface | Very slow | Spinal implants |
2. Natural Biopolymers
| Material | Degraded by | Applications |
|---|---|---|
| Collagen | Collagenase | Wound healing, tendon/ligament repair, vascular wraps |
| Chitosan | Lysozyme | Wound dressings, cartilage scaffolds, drug delivery |
| Silk fibroin | Proteases | Ligament repair, corneal scaffolds |
| Hyaluronic acid | Hyaluronidase | Joint injections, ophthalmic viscosurgery |
| Fibrin | Plasmin | Hemostatic sealants, tissue glue |
| PLLA (Sculptra) | Hydrolysis | Injectable facial volume filler (Andrews' Diseases of the Skin) |
3. Biodegradable Metals (newest class)
| Metal | Corrosion Products | Key Advantage | Limitation |
|---|---|---|---|
| Magnesium (Mg) | Mg(OH)₂ → Mg²⁺ (renal excretion) | Stiffness matches bone (41-45 GPa vs bone 15-25 GPa); stimulates osteogenesis | H₂ gas evolution in early alloys |
| Zinc (Zn) | Zn²⁺ | Slower than Mg, antimicrobial | Less studied |
| Iron (Fe) | Fe³⁺/iron oxides | Highest mechanical strength | Too slow to degrade |
4. Ceramics and Composites
- Hydroxyapatite (HA) and tricalcium phosphate (TCP): Resorbable bone substitutes that dissolve as osteoclasts remodel the defect
- Polymer-HA composites: Combine PLA/PCL matrices with ceramic filler to mimic the organic-inorganic architecture of natural bone
Degradation Mechanisms
Ester bonds + H₂O → carboxylic acids + alcohols → CO₂ + H₂O
Collagen + Collagenase → amino acids → protein metabolism (predictable, gradual)
Mg + 2H₂O → Mg(OH)₂ + H₂↑ → Mg²⁺ ions → renally excreted
Clinical Indications and Applications
Orthopedics (75% of all biodegradable implant use)
- Fracture fixation plates, screws, pins - especially in children (avoids growth restriction and transcranial migration risk from permanent plates). PLA/PGA systems used for pediatric facial fractures with good outcomes (Cummings Otolaryngology, p. 3941)
- Suture anchors for rotator cuff and Bankart repair
- Interference screws for ACL/PCL reconstruction
- Bone void fillers (HA/TCP composites)
- Osteomyelitis treatment: Biodegradable antibiotic carriers with osteoinductive + osteoconductive properties for infected bone defects (Rockwood & Green's Fractures, p. 175)
Cardiovascular
- Bioresorbable vascular scaffolds (BVS) - PLLA-based (e.g., Abbott Absorb); support vessel lumen for 6-12 months then fully resorb, restoring natural vasomotion
- Biodegradable Mg/Zn/Fe stents for coronary and peripheral use
- Perivascular sirolimus-eluting biodegradable collagen wraps at AV fistula anastomosis - Phase III RCT underway for dialysis patients (Comprehensive Clinical Nephrology, p. 1031)
Ophthalmology
- Ozurdex (dexamethasone 700 µg PLGA intravitreal implant) - FDA-approved for macular edema from CRVO/BRVO and posterior uveitis. The GENEVA trial showed sustained visual + anatomical improvement (Kanski's, p. 997)
ENT
- Propel corticosteroid-releasing biodegradable stent - only FDA-approved drug-eluting bioresorbable implant for post-FESS sinus surgery; releases mometasone furoate to prevent re-stenosis (K.J. Lee's Otolaryngology)
General Surgery / Hernia
- Biological and biodegradable meshes for abdominal wall, pelvic floor, and hiatal hernia repair - expensive but eliminate permanent mesh complications (Bailey and Love's Surgery, p. 1783)
Drug Delivery
- PLGA microspheres for controlled release (contraceptives, GnRH agonists, cancer drugs)
- Gliadel wafers (carmustine BCNU) - biodegradable polymer wafers implanted in glioblastoma resection cavity
- Sculptra (PLLA) - injectable biodegradable filler stimulating collagen synthesis for facial atrophy (Andrews' Diseases of the Skin)
Wound Closure
- Absorbable sutures (Vicryl = PGA/PLA; Monocryl; PDS) - the original biodegradable implants, universally used
Dentistry
- Guided bone/tissue regeneration (GBR/GTR) biodegradable membranes
- Biodegradable drug-laden films for local antibiotic delivery in periodontitis
Advantages
| Advantage | Explanation |
|---|---|
| No second surgery | Eliminates removal operation, anesthesia, hospital stay, cost |
| Eliminates stress shielding | Especially Mg alloys - load transferred back to bone as implant degrades, stimulating remodeling |
| Reduced long-term infection | No permanent foreign body for late biofilm formation |
| Drug elution built-in | Can deliver antibiotics, steroids, growth factors locally at controlled rates |
| MRI-compatible | Polymer implants generate no artifact (unlike Ti/stainless steel) |
| Tissue regeneration scaffold | Guides cell infiltration and neo-tissue formation |
| Pediatric growth safety | Avoids growth restriction and plate migration seen with permanent fixation |
| Restores vessel physiology | BVS restore vasomotion once scaffold resorbs |
| Reduced long-term hardware complications | No late fracture, migration, corrosion, or metallic staining |
Disadvantages and Challenges
| Limitation | Clinical Impact |
|---|---|
| Inferior mechanical strength | Cannot use in load-bearing areas (femur shaft, mandible) - FDA has not approved resorbable plates for these areas |
| Unpredictable in vivo degradation | Local pH, perfusion, mechanical loading all alter degradation rate |
| Inflammatory reaction (6-18 months) | Acid byproducts from hydrolysis cause swelling, fluid collections, granulomas, osteolysis, or hardware extrusion (Cummings, p. 3943) |
| Bulk degradation failure risk | Polyesters may suddenly lose integrity before healing is complete |
| Technically demanding | Require thermal contouring, pretapping, specialized tools - more skill-intensive than titanium |
| Bulkier profile | Higher profile than titanium plates - palpable/visible under thin skin |
| Radiolucency | Cannot be seen on plain X-ray - harder to confirm placement or detect failure |
| Higher cost | Complex synthesis, high-purity standards, sterilization = expensive |
| Hydrogen gas evolution | First-generation Mg alloys produced gas pockets in tissue (addressed by alloying) |
| Foreign body response | Long-term immunological interaction with degradation products incompletely characterized |
| Insufficient RCT data | A Cochrane review found insufficient evidence comparing resorbable vs titanium fixation for facial fractures (Cummings, p. 3945) |
Novel Developments (2024-2026)
-
Biodegradable zinc alloys - Emerging as a "middle ground" metal: slower degradation than Mg, faster than Fe, with excellent cytocompatibility (Rao et al., ACS Biomater Sci Eng 2024 - PMID 39082869)
-
Rare-earth Mg alloys (Y, Ce, Nd) - Improved corrosion resistance and mechanical performance for bone implants (Yue et al., 2025 - PMID 41448776)
-
4D-printed shape-memory implants - Shape-memory polymers that self-fit after implantation in response to body temperature or pH
-
GelMA hydrogels (gelatin methacryloyl) - Photocrosslinkable, cell-laden resins for cardiac and neural tissue regeneration with programmable stiffness
-
Degradable elastomers - Combine full degradability with elasticity for soft tissues (myocardium, trachea, bladder)
-
Patient-specific 3D-printed biodegradable implants - CT/MRI-guided craniofacial reconstruction in pediatric patients (referenced in Cummings Otolaryngology)
-
Biodegradable electronic implants - Dissolving sensors embedded in polymer matrix to monitor healing then self-destruct
-
Market growth - Global biodegradable implant market projected to grow from USD 6.57 billion (2024) to USD 9.94 billion by 2030 (CAGR 7.07%), reflecting rapid clinical adoption
Quick Reference Comparison
| Feature | Biodegradable Implant | Permanent Implant |
|---|---|---|
| Second removal surgery | Not needed | Often required |
| MRI artifact | None (polymers) | Significant |
| Stress shielding | Low/none | High |
| Mechanical strength | Moderate | High |
| Long-term infection risk | Lower | Higher |
| Drug delivery | Yes | Limited |
| Load-bearing use | Limited | Full |
| Initial cost | Higher | Lower |
| X-ray visibility | Poor (polymers) | Excellent |
| Pediatric growth impact | None | Yes |
Reflex arc explain in detail with flowcharts problems with it causes and effects due to impairment and everything else related to it for 10 marks question with appropriate illustrative diagrams rehabilitation
reflex arc anatomy components flowchart diagram impairment rehabilitation 2024
reflex arc impairment UMN LMN signs rehabilitation physiotherapy spasticity areflexia treatment
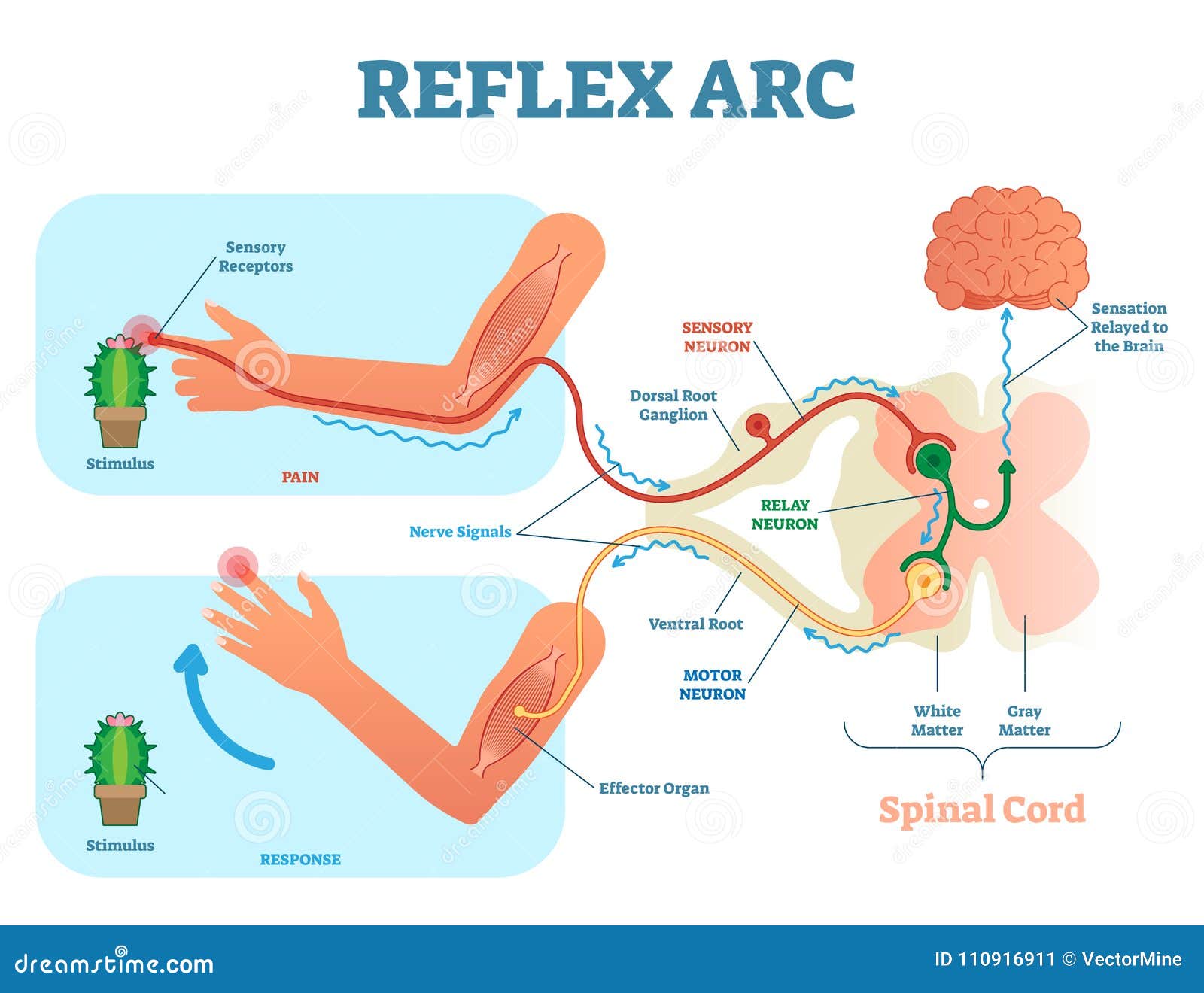
The Reflex Arc - Complete 10-Mark Answer
1. Definition
2. Components of the Reflex Arc
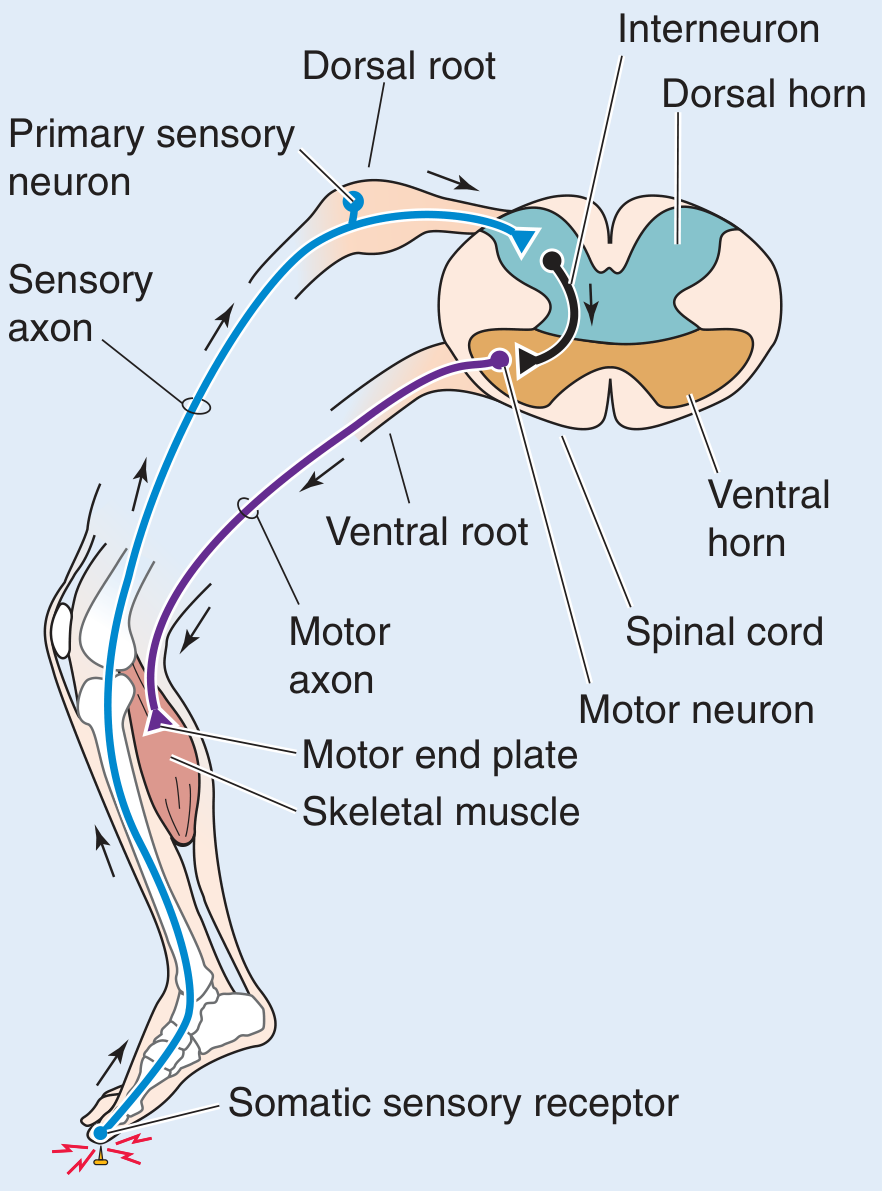
Component 1: Receptor
- A specialized sensory structure at the periphery that detects a specific stimulus
- Transduces the physical/chemical stimulus into an electrical nerve impulse (action potential)
- Types: mechanoreceptors, nociceptors, thermoreceptors, chemoreceptors
- Examples: muscle spindles (stretch), Golgi tendon organs (tension), Meissner's corpuscles (touch), free nerve endings (pain)
Component 2: Afferent (Sensory) Neuron
- Carries the action potential from receptor toward the CNS
- Cell body located in the dorsal root ganglion (DRG)
- Axon enters the spinal cord via the dorsal (posterior) root
- Classified by fiber type:
- Ia fibers (large, fast, myelinated) - from muscle spindles
- Ib fibers - from Golgi tendon organs
- II fibers - secondary endings of muscle spindles
- Aδ and C fibers - pain/temperature (slow)
Component 3: Interneuron (Relay/Integration Neuron)
- Located entirely within the gray matter of the spinal cord (dorsal and intermediate horns)
- Processes and integrates information; may be excitatory or inhibitory
- In monosynaptic reflexes (stretch reflex): absent - Ia fiber synapses directly on alpha motor neuron
- In polysynaptic reflexes (withdrawal reflex): one or more interneurons are present
- Enables reciprocal inhibition: excites agonist motor neurons while inhibiting antagonist motor neurons via Ia inhibitory interneurons
Component 4: Efferent (Motor) Neuron
- Alpha (α) motor neurons in the ventral horn - innervate extrafusal muscle fibers
- Gamma (γ) motor neurons in the ventral horn - innervate intrafusal fibers of muscle spindle (adjusts spindle sensitivity)
- Axon exits the spinal cord via the ventral (anterior) root
- Forms the peripheral motor nerve
Component 5: Effector Organ
- The target of the motor command - usually skeletal muscle
- Motor axon terminal releases acetylcholine (ACh) at the neuromuscular junction (motor end plate)
- ACh binds nicotinic receptors → end plate potential → muscle contraction → reflex response
3. Flowchart of the Reflex Arc
STIMULUS (external/internal)
│
▼
RECEPTOR (transduces stimulus → action potential)
│
▼
AFFERENT SENSORY NEURON (travels in peripheral nerve)
│
▼
DORSAL ROOT GANGLION (cell body of sensory neuron)
│
▼ (enters via dorsal root)
SPINAL CORD GRAY MATTER
├──▶ INTERNEURON(s) [polysynaptic only]
│ │
│ ▼
└──▶ ALPHA MOTOR NEURON (ventral horn)
│ (exits via ventral root)
▼
PERIPHERAL MOTOR NERVE
│
▼
NEUROMUSCULAR JUNCTION (ACh release)
│
▼
EFFECTOR (skeletal muscle contraction)
│
▼
REFLEX RESPONSE (withdrawal / muscle contraction)
│
▼ (collateral branch of sensory neuron ascends)
BRAIN (conscious perception AFTER reflex occurs)
4. Types of Reflexes
A. By Synapse Number
| Type | Synapses | Example |
|---|---|---|
| Monosynaptic | 1 (Ia → α motor neuron) | Knee-jerk (patellar) reflex, biceps reflex |
| Polysynaptic | 2 or more | Withdrawal/flexion reflex, crossed extension reflex |
B. By Nature
| Type | Arc Location | Example |
|---|---|---|
| Somatic | Spinal cord / brain | Stretch reflex, withdrawal reflex |
| Autonomic | Autonomic ganglia | Pupillary reflex, bladder reflex, micturition |
| Cranial | Brainstem | Corneal reflex, gag reflex, pupillary light reflex |
C. Clinically Important Reflexes
| Reflex | Stimulus | Response | Segment |
|---|---|---|---|
| Patellar (knee jerk) | Tap patellar tendon | Knee extension | L3-L4 |
| Achilles (ankle jerk) | Tap Achilles tendon | Plantar flexion | S1-S2 |
| Biceps | Tap biceps tendon | Elbow flexion | C5-C6 |
| Triceps | Tap triceps tendon | Elbow extension | C7-C8 |
| Babinski (plantar) | Stroke lateral sole | Toe flexion (normal adult) | L5-S1 |
| Corneal | Touch cornea | Bilateral blink | CN V-VII |
| Pupillary | Bright light | Pupil constriction | CN II-III |
| Abdominal | Stroke abdominal wall | Umbilical deflection | T8-T12 |
| Cremasteric | Stroke inner thigh | Testis elevation | L1-L2 |
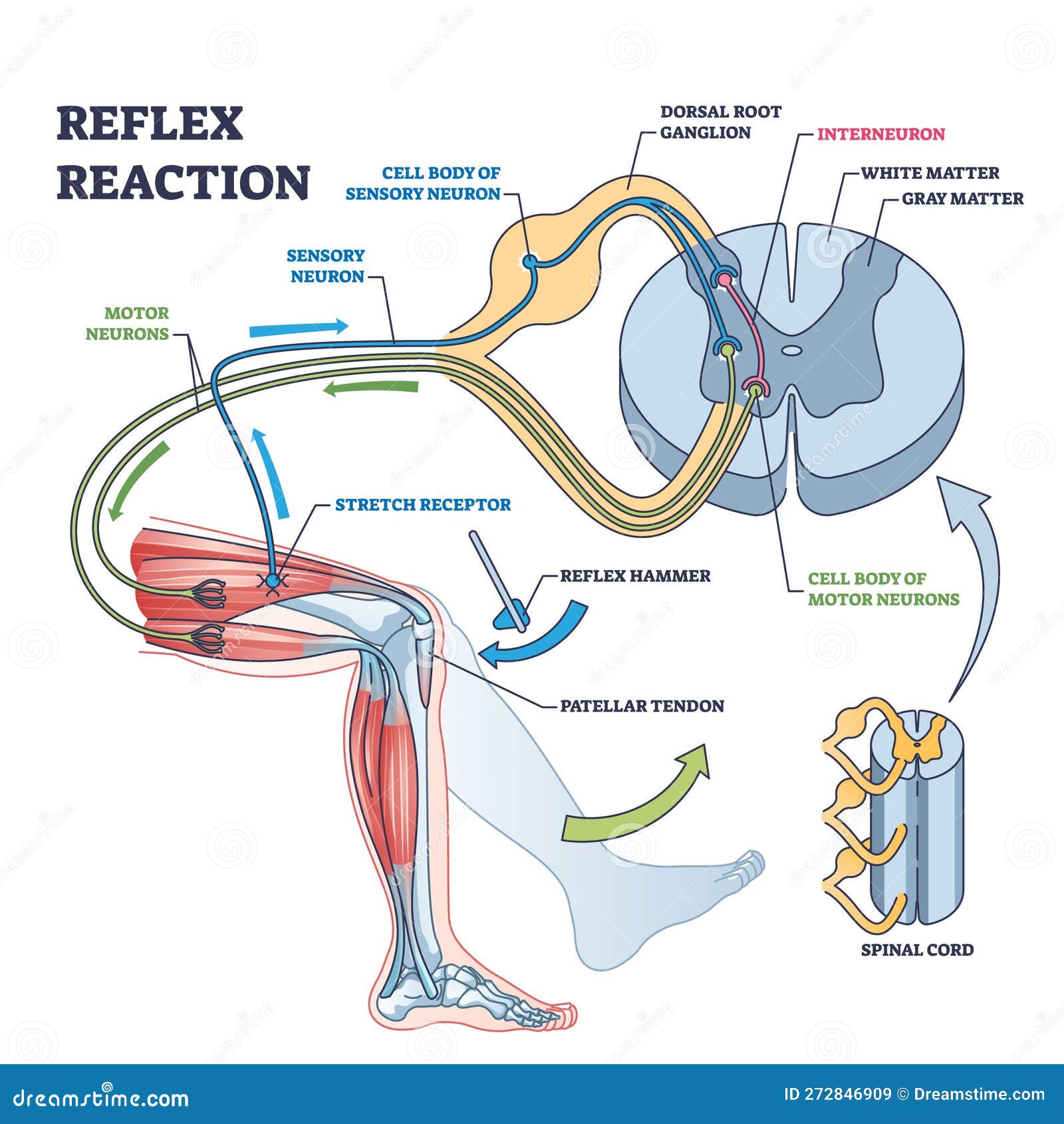
5. Special Mechanisms within the Reflex Arc
Stretch Reflex (Monosynaptic)
Muscle stretched
│
▼
Muscle spindle (intrafusal fiber) activated
│
▼
Type Ia afferent fires (fast, myelinated)
│
├──▶ Directly synapses on α motor neuron (EXCITATION)
│ │
│ ▼
│ Agonist muscle CONTRACTS (resists further stretch)
│
└──▶ Ia inhibitory interneuron (INHIBITION)
│
▼
Antagonist muscle RELAXES (reciprocal innervation)
Golgi Tendon Organ Reflex (Ib - Inverse Stretch / Autogenic Inhibition)
Excessive muscle TENSION detected by GTO
│
▼
Type Ib afferent fires
│
▼
Ib inhibitory interneuron → α motor neuron INHIBITED
│
▼
Muscle RELAXES (protective - prevents tendon rupture)
│
▼
Antagonist EXCITED (autogenic inhibition)
Withdrawal (Flexion) Reflex + Crossed Extension
Noxious stimulus (e.g., stepping on a tack)
│
▼
Nociceptors activated → Aδ/C fibers → dorsal horn
│
├──▶ IPSILATERAL flexor motor neurons EXCITED → limb WITHDRAWN
├──▶ IPSILATERAL extensor motor neurons INHIBITED
│
└──▶ Contralateral interneurons (via commissure)
├──▶ Contralateral EXTENSORS EXCITED (support body weight)
└──▶ Contralateral FLEXORS INHIBITED
6. Anatomy of the Reflex Arc in the Spinal Cord
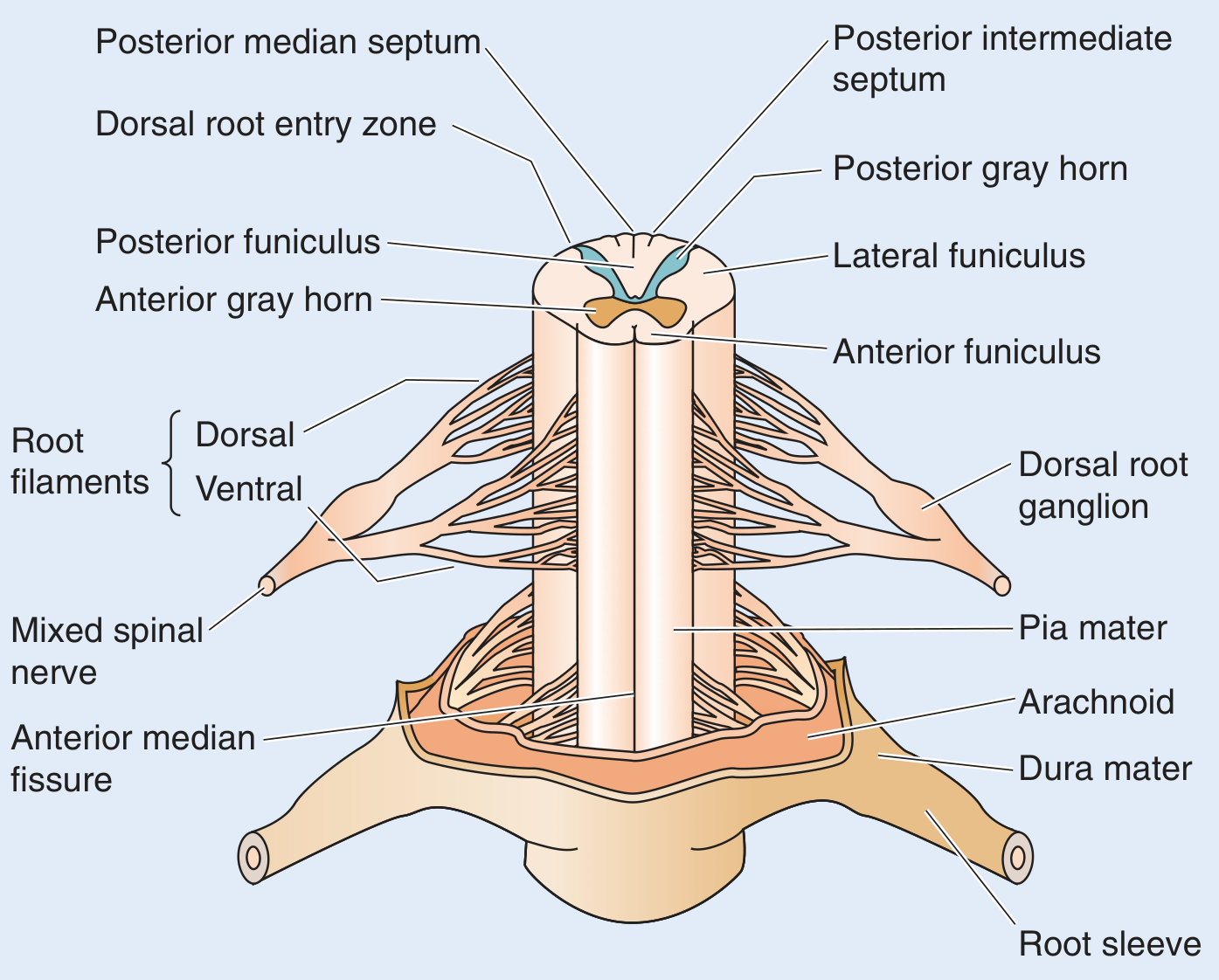
- Gray matter (H-shaped): contains neuronal cell bodies - dorsal horn (sensory processing), ventral horn (motor neurons), intermediate zone (interneurons and autonomic neurons)
- White matter (surrounding gray): contains myelinated axon tracts - ascending (sensory) and descending (motor)
- Dorsal root ganglion: houses sensory neuron cell bodies
- Ventral horn: contains α motor neuron cell bodies (the "final common pathway")
7. Problems with the Reflex Arc - Causes and Effects of Impairment
A. Site 1 - Receptor Damage
| Cause | Clinical Effect |
|---|---|
| Diabetic peripheral neuropathy | Loss of proprioception → sensory ataxia, Charcot joints |
| Vitamin B12 deficiency | Subacute combined degeneration, loss of deep tendon reflexes |
| Leprosy | Loss of pain receptors → repeated trauma, trophic ulcers |
| Tabes dorsalis (neurosyphilis) | Destruction of dorsal root ganglia → absent knee jerks, Romberg positive |
B. Site 2 - Afferent (Sensory) Neuron Damage (Peripheral Neuropathy)
| Cause | Clinical Effect |
|---|---|
| Guillain-Barré Syndrome (GBS) | Acute demyelinating neuropathy → ascending areflexia |
| Diabetic neuropathy | Absent ankle jerk (earliest sign) |
| Hypothyroid neuropathy | Delayed relaxation of reflexes ("hung-up reflex") |
| Trauma to dorsal roots | Segmental sensory loss + areflexia at that level |
| CIDP | Chronic progressive areflexia |
C. Site 3 - Interneuron Damage (Spinal Cord Gray Matter)
| Cause | Clinical Effect |
|---|---|
| Poliomyelitis | Destroys anterior horn cells (motor neurons) → flaccid paralysis |
| Syringomyelia | Cavity in central cord → loss of reflexes at level of cavity |
| Transverse myelitis | All reflex arcs below lesion disrupted |
D. Site 4 - Efferent (Motor) Neuron Damage = Lower Motor Neuron (LMN) Lesion
| Cause | Clinical Effect |
|---|---|
| Poliomyelitis | Flaccid paralysis, areflexia, atrophy, fasciculations |
| Peripheral nerve trauma | Loss of reflexes in that nerve's distribution |
| ALS (lower motor neuron component) | Atrophy, fasciculations, hyporeflexia |
| Cauda equina syndrome | Loss of patellar and Achilles jerks + sphincter dysfunction |
| Bell's palsy | Loss of corneal reflex (efferent = CN VII) |
↓ / Absent reflexes (areflexia / hyporeflexia)
Flaccid weakness (hypotonia)
Muscle wasting (atrophy)
Fasciculations
No pathological reflexes
E. Site 5 - Upper Motor Neuron (UMN) Pathway Damage (Descending Control)
| Cause | Clinical Effect |
|---|---|
| Stroke (CVA) | Contralateral spasticity, hyperreflexia, Babinski sign |
| Spinal cord injury | Spasticity below level, hyperreflexia, clonus |
| Multiple sclerosis | Variable hyperreflexia, Lhermitte's sign |
| Cerebral palsy | UMN pattern; scissors gait, hyperreflexia |
| ALS (upper motor neuron) | Hyperreflexia + spasticity despite wasting |
| Brain tumor (motor cortex) | Contralateral UMN signs |
↑ Reflexes (hyperreflexia)
Spasticity (velocity-dependent increase in tone)
Clonus (sustained rhythmic reflex beats)
Babinski sign (extensor plantar response)
Hoffmann's sign (finger flexion)
Loss of abdominal reflexes
Pseudobulbar palsy
No fasciculations / minimal atrophy
Temporal Pattern of Reflex Changes After Spinal Cord Injury
ACUTE PHASE (hours to days):
SPINAL SHOCK
└─ All reflexes ABSENT below lesion
└─ Flaccid paralysis
└─ Urinary retention / ileus
└─ Returns when bulbocavernosus reflex reappears (Rosen's EM)
↓ (days to months)
CHRONIC PHASE:
HYPERREFLEXIA
└─ Exaggerated tendon reflexes
└─ Clonus
└─ Spasticity
└─ Pathological reflexes (Babinski)
└─ Flexor / extensor spasms
└─ Autonomic dysreflexia (above T6 injuries)
8. Comparison: UMN vs LMN Lesion Effects on Reflex Arc
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Reflexes | Hyperreflexia, clonus | Areflexia / hyporeflexia |
| Muscle tone | Spasticity (hypertonia) | Flaccidity (hypotonia) |
| Muscle bulk | Minimal atrophy | Significant atrophy |
| Fasciculations | Absent | Present |
| Babinski sign | Present (positive) | Absent |
| Weakness | Whole limb ("pyramidal") | Focal (individual muscles) |
| Location of lesion | Brain / spinal cord (above anterior horn) | Anterior horn / ventral root / peripheral nerve |
| Examples | Stroke, SCI, MS, CP | Polio, GBS, peripheral nerve injury |
9. Clinical Testing of Reflex Arc Integrity
Grading (NINDS Scale):
0 = Absent (areflexia)
1+ = Diminished / trace
2+ = Normal
3+ = Brisk (borderline hyperreflexia)
4+ = Hyperactive with clonus (pathological)
Key Tests:
- Deep tendon reflexes (DTRs): Biceps, triceps, brachioradialis, patellar, Achilles
- Plantar response (Babinski): Stroke lateral sole heel-to-toe → normal = downgoing toe; abnormal (UMN) = upgoing great toe + fanning
- Abdominal reflexes: Lost in UMN lesions above T6-T12; preserved in LMN
- Bulbocavernosus reflex: Sacral arc (S3-S4) integrity; its return marks end of spinal shock (Rosen's Emergency Medicine)
- Sacral reflex arc assessment: Electrophysiological evaluation via pudendal nerve conduction studies and bulbocavernosus reflex latency (Bradley and Daroff's Neurology)
10. Rehabilitation of Reflex Arc Impairment
A. For LMN / Areflexic Patients (Peripheral Nerve / Anterior Horn)
| Goal | Intervention |
|---|---|
| Prevent muscle atrophy | Functional electrical stimulation (FES) directly stimulates muscle |
| Maintain joint mobility | Passive range of motion (PROM), splinting |
| Facilitate nerve regeneration | Neuromuscular re-education, biofeedback, electrotherapy |
| Strengthen recovering muscles | Progressive resistive exercises as reinnervation occurs |
| Sensory re-education | Graded tactile stimulation, mirror therapy |
| Orthoses | AFO (ankle foot orthosis) for foot drop |
B. For UMN / Spastic / Hyperreflexic Patients
| Approach | Method |
|---|---|
| Physical therapy | Stretching (inhibits stretch reflex), Bobath neurodevelopmental therapy, PNF, Task-oriented training |
| Spasticity management | Baclofen (GABA-B agonist) - inhibits excitatory synaptic input to motor neurons; Tizanidine (α2-agonist); Diazepam (GABA-A agonist) |
| Botulinum toxin | Blocks ACh release at NMJ → local reduction of spastic muscle overactivity |
| Intrathecal baclofen (ITB) | Pump delivers baclofen directly to CSF for severe spasticity |
| Constraint-induced movement therapy | Forces use of affected limb to drive cortical neuroplasticity |
| Neuromuscular electrical stimulation | FES for drop-foot, standing programs |
| Surgical | Selective dorsal rhizotomy (SDR) - cuts sensory roots to reduce stretch reflex input; tendon lengthening for contractures |
| Body-weight supported treadmill training | Activates spinal locomotor circuits (central pattern generators) |
| Robotic-assisted gait training | Exoskeletons guide normal gait pattern |
C. Neuroplasticity - Long-Term Changes in Reflex Pathways
- Training / operant conditioning - the H-reflex (electrical equivalent of tendon jerk) can be voluntarily upregulated or downregulated with training, demonstrating that spinal circuits are plastic
- After spinal cord injury - Ia axons release more transmitter; α motor neurons sprout dendrites (dendritic sprouting) and develop denervation hypersensitivity, contributing to spasticity
- Task-specific rehabilitation - repetitive practice activates spinal interneuron circuits and drives neuroplastic reorganization, even in chronically injured patients
- Pre-movement facilitation - Intention to move can facilitate reflex transmission 50 ms before actual movement, showing top-down modulation of spinal reflex circuits
Summary Flowchart: Reflex Arc and Its Impairments
┌──────────────────────────────┐
│ STIMULUS │
└──────────┬───────────────────┘
│
┌──────────▼───────────────────┐
│ RECEPTOR │◄── Diabetic neuropathy
│ (muscle spindle, GTO, │ Leprosy, Tabes dorsalis
│ nociceptors, tactile) │
└──────────┬───────────────────┘
│ (Action potential)
┌──────────▼───────────────────┐
│ AFFERENT (SENSORY) NEURON │◄── GBS, Peripheral neuropathy
│ (Dorsal root ganglion) │ Vitamin B12 def, CIDP
└──────────┬───────────────────┘
│ (Dorsal root entry)
┌─────────────────────▼────────────────────────┐
│ SPINAL CORD │
│ ┌─────────────────────────────────────┐ │◄── Spinal cord injury
│ │ INTERNEURON (Dorsal/Intermediate │ │ Syringomyelia
│ │ horn gray matter) │ │ Poliomyelitis
│ │ [absent in monosynaptic] │ │
│ └──────────────┬──────────────────────┘ │
│ │ │
│ ┌──────────────▼──────────────────────┐ │
│ │ ALPHA MOTOR NEURON (Ventral horn) │ │◄── Polio, ALS (LMN)
│ │ [Final common pathway] │ │ MND, motor neuropathy
│ └──────────────┬──────────────────────┘ │
└─────────────────┼────────────────────────────┘
│ (Ventral root exit)
┌──────▼───────────────────┐
│ PERIPHERAL MOTOR NERVE │◄── Peripheral nerve trauma
└──────────┬───────────────┘ Entrapment neuropathy
│ (ACh release)
┌──────────▼───────────────┐
│ EFFECTOR (Muscle) │◄── Myopathy (not arc itself)
└──────────┬───────────────┘
│
┌──────────▼───────────────┐
│ REFLEX RESPONSE │
└───────────────────────────┘
DESCENDING CONTROL (UMN - Corticospinal tract)
└──▶ Modulates interneuron and motor neuron excitability
└──▶ UMN lesion → removes inhibition → HYPERREFLEXIA, SPASTICITY
└──▶ Stroke, SCI, MS, CP, ALS (UMN component)
Key References (Textbook Sources)
- Medical Physiology (Boron & Boulpaep) - Spinal reflex arc anatomy and physiology, Box 16-1 Motor System Injury, Figure 10-11
- Eric Kandel Principles of Neural Science 6th Ed. - Reflex pathways, stretch reflex, spasticity, spinal shock, long-term changes
- Bradley and Daroff's Neurology in Clinical Practice - Box 97.2 UMN signs, Babinski sign, pseudobulbar palsy
- Rosen's Emergency Medicine - Spinal reflex examination table; bulbocavernosus reflex and spinal shock
- Harrison's Principles of Internal Medicine 22E (2025) - Distribution of weakness, UMN/LMN differentiation
- Goldman-Cecil Medicine - Upper motor neuron syndrome, spasticity
- Campbell-Walsh Urology - Reflex arc components; spinal shock and bladder areflexia
Gas gangrene etiology pathology and signs and symptoms and investigations and evaluation and treatment it's effects in view of orthopaedics explain in detail with appropriate illustrative diagrams and images
gas gangrene clostridial myonecrosis etiology pathology orthopaedic treatment signs symptoms 2024
gas gangrene X-ray radiograph soft tissue gas feathery appearance crepitus orthopaedic open fracture
Gas Gangrene (Clostridial Myonecrosis) - Complete Orthopaedic Review
1. Definition
2. Etiology
Causative Organisms
| Organism | Frequency | Special Features |
|---|---|---|
| C. perfringens | >80% | Lecithinase (α-toxin); nonmotile; major cause of traumatic gas gangrene |
| C. septicum | Common | Aerotolerant; associated with spontaneous gas gangrene + underlying malignancy (colon Ca) + neutropenia |
| C. novyi | Less common | Produces highly lethal delta-toxin |
| C. histolyticum | Less common | Aggressive connective tissue destruction |
| C. bifermentans | Less common | Traumatic wounds |
| C. sporogenes | Less common | Wound contamination |
| C. sordellii | Rare | Toxic shock syndrome; gynaecological wounds |
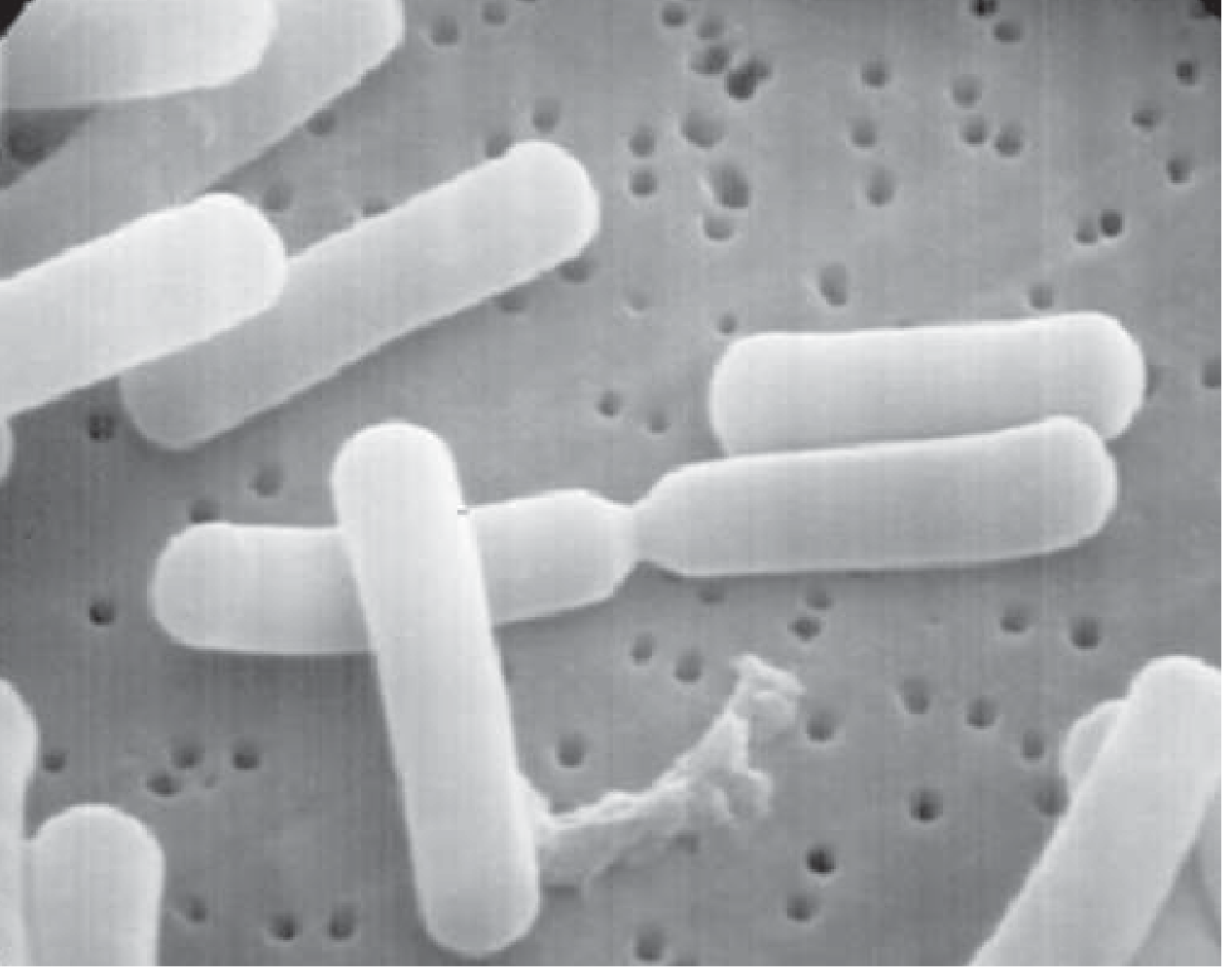
Microbiology of the Organism
- Gram-positive, pleomorphic rods, arranged singly or in short chains
- Spore-forming - spores survive in soil and can withstand 100°C for >1 hour
- Obligate anaerobe - flourishes in low-oxygen, low-redox-potential environments
- Nonmotile (C. perfringens)
- Stains gram-positive early; may appear gram-variable in late growth or infected tissue
- Produces more protein toxins than any other bacterial genus; >25 clostridial toxins lethal to mice identified (Harrison's 22E)
Predisposing Conditions
| Category | Conditions |
|---|---|
| Traumatic | Open/compound fractures, gunshot wounds, crush injuries, road traffic accidents (60% of cases) |
| Surgical | Bowel surgery, biliary surgery, amputations for peripheral vascular disease |
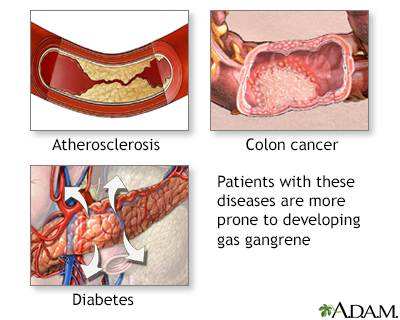
| Systemic | Diabetes mellitus, peripheral vascular disease, immunocompromised state, malignancy (especially colonic Ca - associated with C. septicum) |
| Drug-related | IV drug abuse (needle track infections) |
| Obstetric | Non-sterile abortion, retained products of conception |
| Military | High-velocity missile/shrapnel wounds with extensive devitalisation and soil contamination |
3. Pathology and Pathogenesis
The Vicious Cycle of Gas Gangrene
DEVITALISED / ISCHAEMIC TISSUE
(low O₂, low redox potential, necrotic muscle)
│
▼
C. perfringens SPORES GERMINATE
(from soil contamination / patient's own gut flora)
│
▼
VEGETATIVE BACTERIA MULTIPLY RAPIDLY
(doubling time: ~8 minutes under optimal conditions)
│
▼
EXOTOXIN PRODUCTION (especially α-toxin)
│
┌────┴────────────────────┐
▼ ▼
LOCAL EFFECTS SYSTEMIC EFFECTS
├── Muscle necrosis ├── Haemolysis
├── Vascular thrombosis ├── Haemoglobinaemia
├── Spreading oedema ├── Hypotension/shock
├── Gas production ├── AKI
└── Further ischaemia └── ARDS → Death
│
▼
MORE ANAEROBIC ENVIRONMENT
→ Further bacterial proliferation
→ Worsening necrosis (self-perpetuating cycle)
Key Toxins of C. perfringens
| Toxin | Type | Action | Effect |
|---|---|---|---|
| α-toxin (alpha) | Lecithinase (phospholipase C) | Destroys RBCs, WBCs, platelets, fibroblasts, muscle cells | Most important - causes haemolysis, muscle necrosis, shock |
| θ-toxin (theta) | Perfringolysin O (pore-forming) | Disrupts cell membranes | Oxygen deprivation; myocardial depression |
| φ-toxin (phi) | Cardiotoxin | Myocardial suppression | Cardiac failure |
| κ-toxin (kappa) | Collagenase | Destroys connective tissue and blood vessels | Spreading tissue destruction |
| µ-toxin (mu) | Hyaluronidase | Degrades hyaluronic acid | Facilitates spread |
| ν-toxin (nu) | DNase | DNA degradation | Cell destruction |
Histopathology
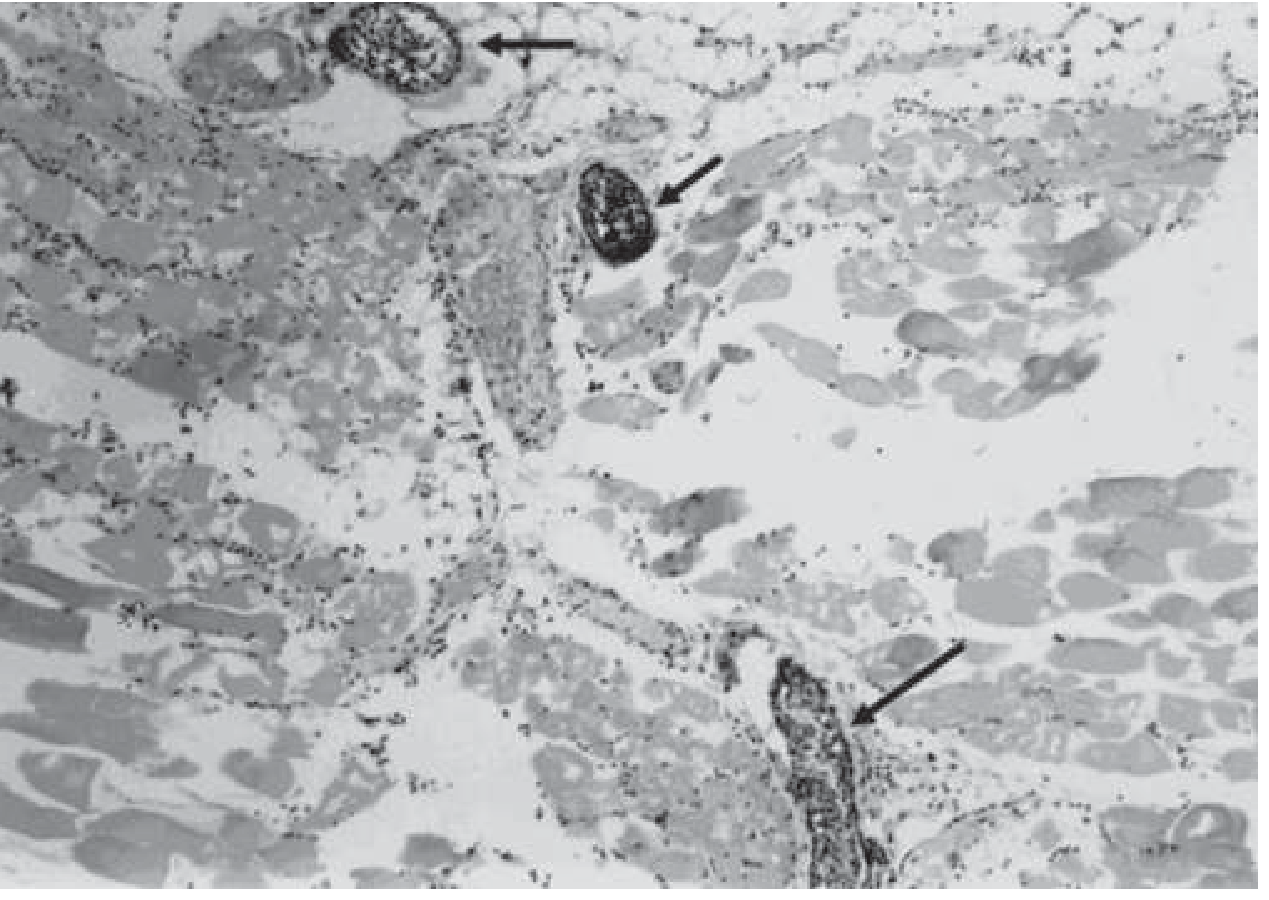
- Widespread muscle necrosis - coagulative and liquefactive
- Paucity of leukocytes in infected tissue - α and θ toxins destroy neutrophils before they can enter
- Leukocyte accumulation in adjacent blood vessels - the toxins prevent leukocyte migration into tissue
- Gas bubbles between muscle fibres (hydrogen, nitrogen, CO₂, H₂S)
- Gram-positive rods present in necrotic tissue (with or without spores)
- Vascular thrombosis - end arteries occluded → extending ischaemia
Gas Composition
4. Clinical Classification
A. Traumatic Gas Gangrene (60% of cases)
- Post-injury: RTA, gunshot, crush injuries, compound fractures
- C. perfringens predominates
- Incubation: usually <24 hours (range 1 hour to 6 weeks)
B. Post-operative Gas Gangrene
- Bowel/biliary surgery, amputations, abdominal wall procedures
- Contamination from patient's own gut flora
C. Spontaneous (Non-traumatic) Gas Gangrene
- No obvious wound
- C. septicum predominates
- Haematogenous spread from a bowel source
- Strongly associated with:
- Colorectal carcinoma (>50% have GI malignancy)
- Neutropenia / neutropenic enterocolitis
- Diabetes mellitus
- Severe atherosclerosis
5. Signs and Symptoms
Local Signs (Temporal Progression)


| Timeline | Signs |
|---|---|
| Earliest (1-4 hours) | Sudden, severe pain at wound site - disproportionate to wound appearance; "heaviness/pressure" in limb |
| Early (4-8 hours) | Oedema, pallor, serosanguineous exudate from wound; skin tense and shiny |
| Progressive (8-24 hours) | Skin turns bronze → brown → blue-black; haemorrhagic bullae; serosanguineous discharge |
| Established | Crepitus (soft tissue gas palpable); characteristic sickly-sweet or "mousy" odour; gas visible on X-ray |
| Advanced | Skin sloughing; frank gangrene; violent bronze/black discolouration |
Systemic Signs
| System | Signs |
|---|---|
| Cardiovascular | Tachycardia (disproportionate to fever - early sign), hypotension, shock |
| Neurological | Paradoxical mental clarity until late stages (patients remain remarkably alert) then confusion, coma |
| Renal | Oliguria → acute kidney injury (myoglobinuria, haemoglobinaemia) |
| Haematological | Intravascular haemolysis, jaundice, haemoglobinaemia, haemoglobinuria |
| Respiratory | Tachypnoea, ARDS |
| General | Pyrexia (low-grade initially), pallor from haemolysis, diaphoresis |
Classic Clinical Triad:
1. Severe pain out of proportion to wound appearance
2. Crepitus (gas in tissues) + sweet smell
3. Systemic toxicity (tachycardia > fever, altered sensorium)
6. Investigations and Evaluation
A. Laboratory Investigations
| Test | Finding | Significance |
|---|---|---|
| CBC | Anaemia (haemolytic), leukocytosis or paradoxical leukopenia | Haemolysis from α-toxin; leukopenia is ominous |
| Peripheral blood smear | Haemolysis, ghost cells, helmet cells | Confirms intravascular haemolysis |
| Gram stain of wound exudate | Large Gram-positive rods WITHOUT neutrophils | Pathognomonic finding |
| Blood cultures | Clostridium spp. (bacteraemia in severe cases) | Gram-positive rods |
| Anaerobic wound culture | C. perfringens on blood agar - double zone of haemolysis | Confirmatory but results too slow for acute management |
| Metabolic panel | Metabolic acidosis, elevated creatinine, elevated bilirubin | Organ dysfunction |
| Lactate | Elevated | Tissue hypoxia |
| Coagulation | DIC pattern (elevated PT, PTT; low fibrinogen) | Advanced disease |
| LFTs | Hyperbilirubinaemia | Haemolysis |
| CK | Markedly elevated | Myonecrosis |
| Urinalysis | Haemoglobinuria, myoglobinuria | Haemolysis + rhabdomyolysis |
B. Imaging
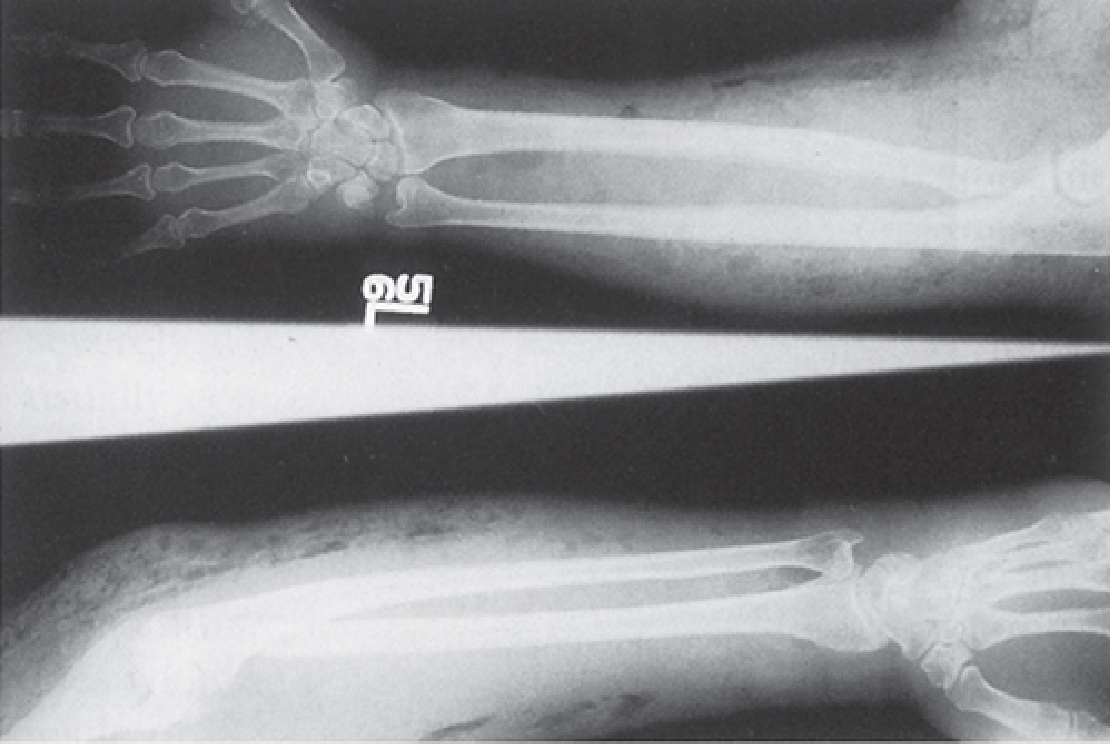
Plain Radiograph (X-ray)

| Modality | Finding | Use |
|---|---|---|
| X-ray | Feathery/streaky gas lucencies between muscle fibres (pathognomonic pattern); gas tracking along fascial planes | Fast, first-line; particularly useful for limbs, chest, abdomen |
| CT scan | Gas in soft tissues, muscle compartments, fascial planes; delineates extent; guides surgical planning | Best for deep/proximal infections (hip, pelvis, paraspinal, retroperitoneum) |
| MRI | Fluid/gas in muscle planes; muscle necrosis (T2 hyperintensity); spread along fascial planes | Most sensitive for extent of infection but time-consuming - should not delay surgery |
| Ultrasound | Gas in soft tissues (hyperechoic foci with dirty shadowing) | Bedside, fast, available |
C. Tissue Examination
- Needle aspiration or punch biopsy - provides etiologic diagnosis in at least 20% of cases (Harrison's)
- Intraoperative findings: grey/dead muscle that does NOT contract to electrocautery stimulation; absent bleeding (key sign); sweet/offensive smell; gas bubbles in tissue
LRINEC Score (Laboratory Risk Indicator for Necrotizing Fasciitis)
| Parameter | Cut-off | Points |
|---|---|---|
| CRP | ≥150 mg/L | 4 |
| WBC | 15-25 cells/µL | 1; >25 = 2 |
| Sodium | <135 mmol/L | 2 |
| Creatinine | >141 µmol/L | 2 |
| Glucose | >10 mmol/L | 1 |
| Haemoglobin | 11-13.5 g/dL | 1; <11 = 2 |
7. Treatment
Principle: Immediate, Multi-Modal, Aggressive Management
SUSPECTED GAS GANGRENE
│
▼
Resuscitate (IV access, fluids, O₂) + ICU admission
│
▼
URGENT SURGICAL EXPLORATION (SIMULTANEOUS WITH ANTIBIOTICS)
│
┌────┴────────────────────────────────┐
▼ ▼
DEBRIDEMENT of AMPUTATION
all devitalised tissue (if systemic toxicity
(back to bleeding, established; life-saving;
viable muscle) do not delay)
│
▼
Leave wound OPEN (no primary closure)
Pack with saline-soaked gauze
Return to OR in 24-48 hours for re-inspection
│
▼
ANTIBIOTICS (IV, high-dose)
│
▼
HYPERBARIC OXYGEN (if available)
│
▼
ICU monitoring: fluid balance, urine output,
haemodynamics, ventilation support, renal replacement
A. Surgical Treatment (Most Important Intervention)
- Emergent surgical debridement - most critical step; all devitalised tissue widely resected back to healthy, bleeding, contracting muscle (Harrison's 22E, p. 1260)
- Wound left open - no primary closure; traumatic wounds / compound fractures closed only after 5-6 days when infection-free
- Amputation - indicated for established gas gangrene with systemic toxicity; must not be delayed as it is life-saving (Bailey & Love's, p. 7388)
- Stump left open and packed with saline-soaked gauze
- No attempt at closure made acutely
- Re-exploration at 24-48 hours - repeat debridement as needed
- Fasciotomy - may be needed to decompress compartments
B. Antibiotic Treatment
| Condition | First-line | Penicillin Allergy |
|---|---|---|
| Gas gangrene (traumatic/spontaneous) | Penicillin G (3-4 MU IV q4h) + Clindamycin (600-900 mg IV q6-8h) × 10-14 days | Clindamycin alone |
| Polymicrobial with clostridia | Ampicillin + Clindamycin + Ciprofloxacin | Vancomycin + Metronidazole + Ciprofloxacin |
- Penicillin G - highly active against C. perfringens (virtually all strains susceptible); bactericidal
- Clindamycin - superior efficacy over penicillin alone because:
- Inhibits bacterial protein/toxin production (α-toxin synthesis blocked)
- Effective regardless of bacterial load or growth phase
- Modulates host immune response
- Achieves excellent tissue penetration
C. Hyperbaric Oxygen Therapy (HBO)
| Parameter | Effect |
|---|---|
| Stops α-toxin production | Prevents further myonecrosis |
| Inhibits bacterial growth | Bacteriostatic/bactericidal to obligate anaerobes |
| Restores host defence | Enables neutrophil phagocytic function |
| Demarcates viable tissue | Helps surgeon identify where to debride |
| Minimum sessions | 3-4 HBO treatments necessary |
D. Supportive ICU Care
- Aggressive IV fluid resuscitation (crystalloid/colloid)
- Urinary catheter - monitor urine output (target >0.5 mL/kg/hr)
- Vasopressors if persistent hypotension (noradrenaline)
- Blood transfusion for haemolytic anaemia
- Renal replacement therapy if AKI
- Ventilatory support for ARDS
- Management of DIC (FFP, platelets, cryoprecipitate)
- Parenteral nutrition (catabolic state)
E. Antitoxin
- Polyvalent clostridial antitoxin: not recommended by current guidelines due to lack of proven benefit and risk of anaphylaxis
8. Gas Gangrene in Orthopaedic Surgery
Primary Orthopaedic Associations
| Orthopaedic Scenario | Risk | Management |
|---|---|---|
| Open (compound) fractures | Highest risk - devitalised muscle + soil contamination + delayed treatment | Gustilo-Anderson classification guides management; emergent debridement is key |
| Crush injuries | Extensive devascularised muscle = ideal anaerobic environment | Early fasciotomy + debridement |
| High-velocity missile wounds | Tissue cavitation sucks foreign material (clothing, soil) into wound | Primary debridement in operating theatre; no primary wound closure |
| Amputations (peripheral vascular disease) | Proximal ischaemic/necrotic tissue; bowel flora contamination | Antibiotic prophylaxis mandatory; consider at high risk (Bailey & Love's, p. 4344) |
| Post-operative wound infection | Following bowel surgery, hip arthroplasty | Aggressive re-exploration |
| Compartment syndrome | Co-exists with gas gangrene; must be relieved | Fasciotomy + debridement |
Orthopaedic Principles for Open Fractures and Gas Gangrene Prevention
Type I - Clean wound <1 cm → Low risk
Type II - Wound 1-10 cm → Moderate risk
Type IIIA - Large wound, adequate coverage → High risk
Type IIIB - Extensive soft tissue loss → Very high risk (gas gangrene territory)
Type IIIC - Vascular injury → Highest risk
- Emergent debridement in operating theatre - excise all devitalised muscle, remove foreign bodies
- Wound irrigation - copious pulsatile lavage (3-6 litres of saline)
- No primary closure - leave wound open; pack with saline-gauze; plan for delayed closure at 5-6 days
- Temporary fracture stabilisation - external fixator preferred in contaminated open fractures (avoids implant burial in infected tissue)
- Serial debridement at 48-hour intervals until wound is clean
- Antibiotic prophylaxis - cefazolin ± metronidazole (IIIB/C: add gram-negative coverage)
- Wound vacuum assisted closure (VAC) - adjunct after initial debridement
- Delayed definitive fixation - only once infection is controlled
Effects of Gas Gangrene on Bone and Joints
| Effect | Mechanism | Consequence |
|---|---|---|
| Osteomyelitis | Haematogenous spread or direct extension | Chronic bone infection, sequestrum formation |
| Septic arthritis | Extension into adjacent joint | Cartilage destruction, joint stiffness |
| Fracture non-union | Periosteal stripping + ischaemia | Delayed/non-union requires secondary procedures |
| Limb loss / amputation | Uncontrolled infection, vascular compromise | Functional disability; phantom pain; need for prosthetics |
| Contractures | Muscle necrosis and scarring | Permanent functional deficit |
| Compartment syndrome | Oedema + gas pressure in closed fascial compartments | Volkmann's ischaemic contracture if missed |
9. Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Necrotising fasciitis | Fascia involved primarily; "dishwater" fluid; "wooden hard" feel; less gas; leukocytes present |
| Anaerobic cellulitis | Gas present but more prominent; pain/toxicity ABSENT; responds to antibiotics alone |
| Clostridial wound contamination | Positive culture WITHOUT tissue necrosis or systemic signs; no treatment needed beyond debridement |
| Fournier's gangrene | Scrotal/perineal gas gangrene; polymicrobial; same emergency principles |
| Crepitant cellulitis | Subcutaneous emphysema without deep infection; post-traumatic air |
10. Prognosis and Mortality
| Scenario | Mortality |
|---|---|
| Overall (treated) | 20-30% |
| With HBO therapy | 9-20% |
| Without HBO | 30-50% |
| Spontaneous gas gangrene (C. septicum) | 60-100% (associated with advanced malignancy) |
| Mortality correlates with | Time to surgery, extent of infection, comorbidities |
11. Prevention
- Early, aggressive wound debridement - most effective preventive measure
- Antibiotic prophylaxis for high-risk procedures - especially amputations for peripheral vascular disease with open/necrotic wounds (Bailey & Love's)
- No primary closure of contaminated or devitalised wounds
- Tetanus prophylaxis co-administered (wound contamination carries tetanus risk as well)
- Irrigation - copious lavage of contaminated wounds
Summary Flowchart
CONTAMINATED / DEVITALISED WOUND
(crush, open fracture, missile, surgery)
│
▼
C. perfringens SPORES GERMINATE
│
▼
ALPHA-TOXIN (lecithinase) + THETA-TOXIN released
│ │
▼ ▼
LOCAL NECROSIS SYSTEMIC ABSORPTION
RBC/WBC/muscle Haemolysis → Shock
destruction │
│ ▼
▼ Organ failure
SPREADING (AKI, ARDS, DIC)
GAS GANGRENE │
│ ▼
└──────► DEATH (if untreated)
TREATMENT:
├── EMERGENCY DEBRIDEMENT / AMPUTATION (most important)
├── Penicillin G + Clindamycin (IV)
├── Hyperbaric Oxygen (if available)
└── ICU resuscitation
Key References (Textbook Sources)
- Harrison's Principles of Internal Medicine 22E (2025) - Chapter 159: Gas Gangrene and Other Clostridial Infections (Bryant & Stevens) - Etiologic agent, pathogenesis, treatment table
- Bailey and Love's Short Practice of Surgery 28th Ed. - Gas gangrene and crush injury (pp. 7338-7396; Summary Box 5.9, pp. 4341-4360)
- Sherris & Ryan's Medical Microbiology 8th Ed. - Gas gangrene: epidemiology, pathogenesis, clinical manifestations (pp. 5030-5140)
- Miller's Review of Orthopaedics 9th Ed. - Gas gangrene: C. perfringens; orthopaedic management
- Goldman-Cecil Medicine - Necrotizing Clostridial Tissue Infection
- Andrews' Diseases of the Skin - Clostridial Myonecrosis