Tropical pulmonary eosinophilia for md exam answer 10 marks from fishman and Murray only with hrct signs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive content from both Fishman's and Murray's. Let me compose the complete 10-mark MD exam answer.
Tropical Pulmonary Eosinophilia (TPE)
10-Mark MD Examination Answer
(Sources: Fishman's Pulmonary Diseases and Disorders, 5th Ed. & Murray & Nadel's Textbook of Respiratory Medicine)
Definition
Tropical pulmonary eosinophilia (TPE) is a distinct hypersensitivity syndrome resulting from an intense immune response to microfilariae of the lymphatic filarial nematodes Wuchereria bancrofti and Brugia malayi that are trapped in the pulmonary vasculature. It represents a rare manifestation (< 1% of those infected) of human filarial infection.
(Fishman's, Ch. 71; Murray & Nadel, Ch. 58)
Epidemiology
- Endemic in tropical and subtropical regions: India, Pakistan, Sri Lanka, Southeast Asia, parts of Africa, Brazil, and Guyana
- Seen in non-endemic regions in immigrants and travelers
- Male predominance - approximately 4:1 (Murray: 80% in men); predominantly middle age (25-40 years)
- No known seasonal or genetic propensity (Fishman's; Murray & Nadel)
Pathogenesis
Mosquito-transmitted third-stage larvae develop into adult worms residing in the lymphatics for up to 20 years. Pregnant female worms release microfilariae into the circulation; these are trapped in the pulmonary vasculature. The release of antigens from degenerating microfilariae triggers an intense pulmonary and systemic inflammatory response characterized by:
- Parasite-specific IgE and IgG antibodies
- Peripheral blood and pulmonary eosinophilia
- Polyclonal B-cell activation (hypergammaglobulinemia)
- Eosinophil degranulation with cytotoxic granule protein release causing tissue destruction
Note: Microfilaremia is absent in TPE - the immune response clears the blood of parasites.
(Fishman's; Murray & Nadel)
Clinical Features
| Feature | Description |
|---|---|
| Cough | Paroxysmal, dry, worse at night (most characteristic symptom) |
| Dyspnea & wheezing | Can be severe, mimics status asthmaticus |
| Fever, malaise | Low-grade, constitutional |
| Weight loss & anorexia | Common |
| Lymphadenopathy | Generalized; more prominent in children |
| Hepatosplenomegaly | Less common in adults |
| Chest examination | Coarse rales, rhonchi, wheezing; normal in ~20% |
| Rare manifestations | Chest pain, pericarditis, CNS involvement, musculoskeletal |
Spontaneous resolution over several weeks may occur but recurrence is common.
(Fishman's; Murray & Nadel)
Laboratory Findings
- Peripheral blood eosinophilia - often > 3000/mm³ (3 × 10⁹/L); may exceed 30,000/mm³ in severe disease
- Total serum IgE - markedly elevated, typically > 1000 U/mL (Murray: > 4200 IU/mL; normal < 100 IU/mL)
- Filarial-specific IgE and IgG (ELISA for W. bancrofti, B. malayi) - markedly elevated
- Eosinophils and Charcot-Leyden crystals in sputum and BAL
- Microfilariae - NOT detectable in blood, sputum, stool, or urine (key diagnostic point)
- Microfilariae may be found in lung and lymph node tissue biopsies
- Elevated BAL and pleural fluid IgE, IgM, IgG, and filarial-specific IgE
- Reduced serum α1-antitrypsin (returns to normal with treatment)
- Leukocytosis; hypergammaglobulinemia
(Fishman's; Murray & Nadel)
Pulmonary Function Tests
- Early/acute (< 1 month): Obstructive ventilatory defect in up to 30%
- Long-standing disease: Restrictive ventilatory defect with reduced DLCO ± concomitant obstruction
- Mild arterial hypoxemia may be present (Fishman's)
Radiology
Chest Radiograph (CXR)
- Normal in up to 20% of patients at presentation
- Diffuse, ill-defined reticulonodular infiltrates, primarily affecting mid to lower lung fields
- Prominent bronchovascular markings
- Bilateral patchy opacities and small nodules
- Hilar adenopathy (occasional)
- Pleural effusion (occasional)
- Cavitation and bronchiectasis are uncommon
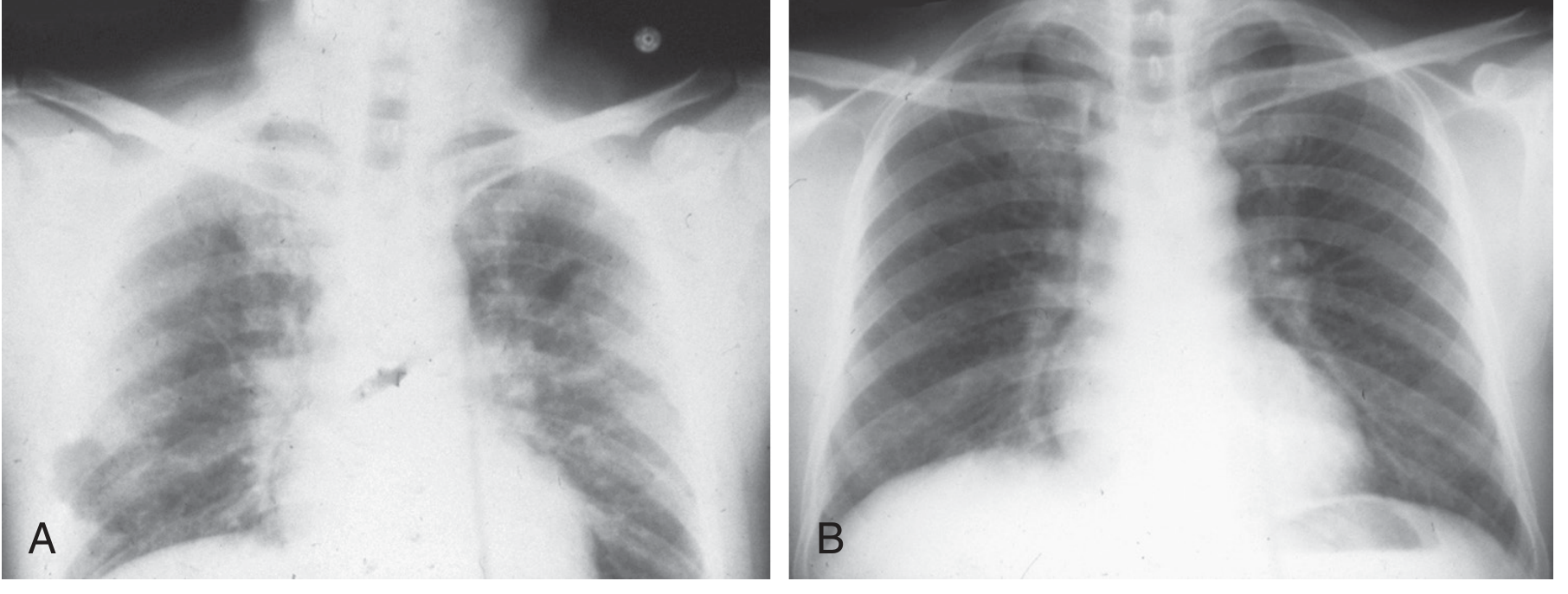
Figure 58.2 (Murray & Nadel): (A) CXR showing subpleural right lung consolidation, subpleural left mid-lung opacity, and bilateral perihilar interstitial thickening. (B) Same patient after DEC treatment - note resolution of opacities.
HRCT Signs (Fishman's, Ch. 71)
HRCT/CT findings in TPE include:
| HRCT Sign | Description |
|---|---|
| Ill-defined bronchocentric nodules | Widespread, small nodules distributed around bronchi and bronchioles; most characteristic CT pattern |
| Ground-glass opacification | Bilateral, diffuse, representing eosinophilic alveolitis |
| Reticulonodular pattern | Diffuse interstitial thickening with nodules, predominantly mid-lower zones |
| Mediastinal/hilar adenopathy | Enlarged mediastinal lymph nodes |
| Bronchiectasis | Traction or cylindrical bronchiectasis, more prominent in chronic/long-standing disease |
| Areas of calcification | Seen in chronic cases |
| Consolidation | Patchy, bilateral, subpleural or perihilar |
| Interstitial fibrosis | Irregular lines, architectural distortion in untreated long-standing disease (>5 years) |
(Fishman's: "CT scans often show widespread, ill-defined bronchocentric nodules, mediastinal adenopathy, bronchiectasis, and areas of calcification.")
(Murray & Nadel: patchy bilateral opacities, small nodules, bilateral perihilar interstitial thickening)
Pathology (Stage-Based)
| Stage | Histology |
|---|---|
| 0-2 weeks | Histiocytic inflammation in alveolar, interstitial, peribronchial, perivascular spaces; preserved lung architecture; tiny palpable nodules |
| 1-3 months | Eosinophilic bronchopneumonia; eosinophilic microabscesses; degenerating microfilariae within abscess centers; bronchial wall edema and epithelial disruption |
| Long-standing (>5 years) | Chronic mixed-cell inflammation (histiocytes, eosinophils, lymphocytes) in nodular pattern; pulmonary fibrosis; foreign body-type granulomas |
Lymph node biopsy may show degenerating microfilariae or adult worms surrounded by eosinophils, granule products, and giant cells.
(Fishman's)
Diagnostic Criteria (Fishman's Table 71-3)
| Criterion |
|---|
| Relevant exposure history in endemic area |
| Paroxysmal nocturnal cough and dyspnea |
| Infiltrate on chest radiograph |
| Leukocytosis with eosinophilia |
| Elevated serum IgE |
| Elevated serum antifilarial IgE and IgG (W. bancrofti, B. malayi) |
| Clinical and hematologic response to diethylcarbamazine (DEC) |
- Lung biopsy is generally not required
- Scalene lymph node biopsy may assist in some cases
Differential Diagnosis
- Bronchial asthma (most common misdiagnosis)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Chronic eosinophilic pneumonia (CEP)
- Loeffler syndrome
- Drug-induced eosinophilic pneumonia
- Hypereosinophilic syndrome (HES)
- Eosinophilic granulomatosis with polyangiitis (EGPA)
- Sarcoidosis, tuberculosis, atypical pneumonia, lymphangitic carcinomatosis
Treatment and Prognosis
Drug of choice: Diethylcarbamazine (DEC)
- Dose: 6 mg/kg/day in 3 divided doses for 14-21 days (Fishman's)
- Murray & Nadel recommends 3 weeks as the standard course
- Acts by direct microfilaricidal and macrofilaricidal mechanisms, and indirectly via immune modulation
Response to treatment:
- Clinical improvement within 7-14 days
- Resolution of eosinophil count, IgE levels, BAL eosinophilia, pulmonary function, and radiographic changes within 1-4 weeks
- Return of serum α1-antitrypsin to normal
Prognosis:
- Curative in most patients with 3 weeks of DEC
- Relapse in up to 20% (due to reinfection or release of microfilariae from persistent adult worms); retreated with higher-dose DEC (2-4 mg/kg TID for 21-30 days)
- Persistent symptoms in up to 13% over 2-5 years
- If untreated: chronic interstitial lung disease, persistent eosinophilia, pulmonary fibrosis
Additional agents:
- Ivermectin (alone or with DEC): some benefit, but limited effect on adult filariae
- Doxycycline: eliminates Wolbachia endosymbiont of W. bancrofti; validated alternative but no head-to-head trials with DEC
- Caution with corticosteroids: can worsen strongyloidiasis (similar presentation)
(Fishman's; Murray & Nadel)
Key Exam Points - Summary
- TPE = hypersensitivity to W. bancrofti / B. malayi microfilariae trapped in pulmonary vasculature
- Characteristic triad: nocturnal cough + marked eosinophilia (>3000/mm³) + markedly elevated IgE (>1000 U/mL)
- Microfilaremia is ABSENT (key differentiating point)
- CXR: reticulonodular infiltrates in mid-lower zones
- HRCT: ill-defined bronchocentric nodules + mediastinal adenopathy + bronchiectasis + calcification (Fishman's)
- PFTs: obstructive early, restrictive later
- Diagnostic criteria include antifilarial serology + response to DEC
- Treatment: DEC 6 mg/kg/day × 14-21 days; relapse rate 20%
- Untreated: fibrosis; avoid steroids alone (may unmask strongyloidiasis)
- Wolbachia endosymbiont targeted by doxycycline as an alternative strategy
This is a shared conversation. Sign in to Orris to start your own chat.