Hashimoto thyroiditis
Reading File
Finding Sources
Searching PubMed
"Hashimoto thyroiditis"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Searching PubMed
"Hashimoto thyroiditis"[MeSH Terms] AND "thyroid peroxidase antibodies"
I have excellent content from multiple authoritative sources. Let me now compile the comprehensive answer.
Hashimoto Thyroiditis
Hashimoto thyroiditis (chronic autoimmune/lymphocytic thyroiditis) is the most common cause of hypothyroidism in iodine-sufficient regions and the most prevalent autoimmune disease in the United States. It was first described by Hakaru Hashimoto in 1912.
Epidemiology
-
Prevalence of hypothyroidism in iodine-replete populations: 1-2%; Hashimoto accounts for ~85% of those cases
-
Mean annual incidence: up to 4 per 1000 women, 1 per 1000 men
-
Female:male ratio = 10:1 to 20:1
-
Peak presentation: 30-65 years of age (mean diagnosis age ~60 years)
-
Subclinical hypothyroidism found in 6-8% of women (10% over age 60) and 3% of men
-
Annual risk of progressing to overt hypothyroidism is ~4% when subclinical hypothyroidism is combined with positive TPO antibodies
-
Robbins & Kumar Basic Pathology, p. 731; Harrison's Principles of Internal Medicine 22E, p. 3072
Types
- Goitrous (classic) form - diffuse thyroid enlargement
- Atrophic form - minimal residual thyroid tissue, represents the end stage with extensive fibrosis
- Fibrosing variant - marked fibrosis with IgG4-positive plasma cell infiltration; can mimic Riedel thyroiditis
- Hashitoxicosis - transient thyrotoxicosis from follicular disruption at disease onset
- Current Surgical Therapy 14e, p. 885
Pathogenesis
The disease results from a breakdown of immune self-tolerance to thyroid autoantigens, leading to progressive autoimmune destruction of thyrocytes:
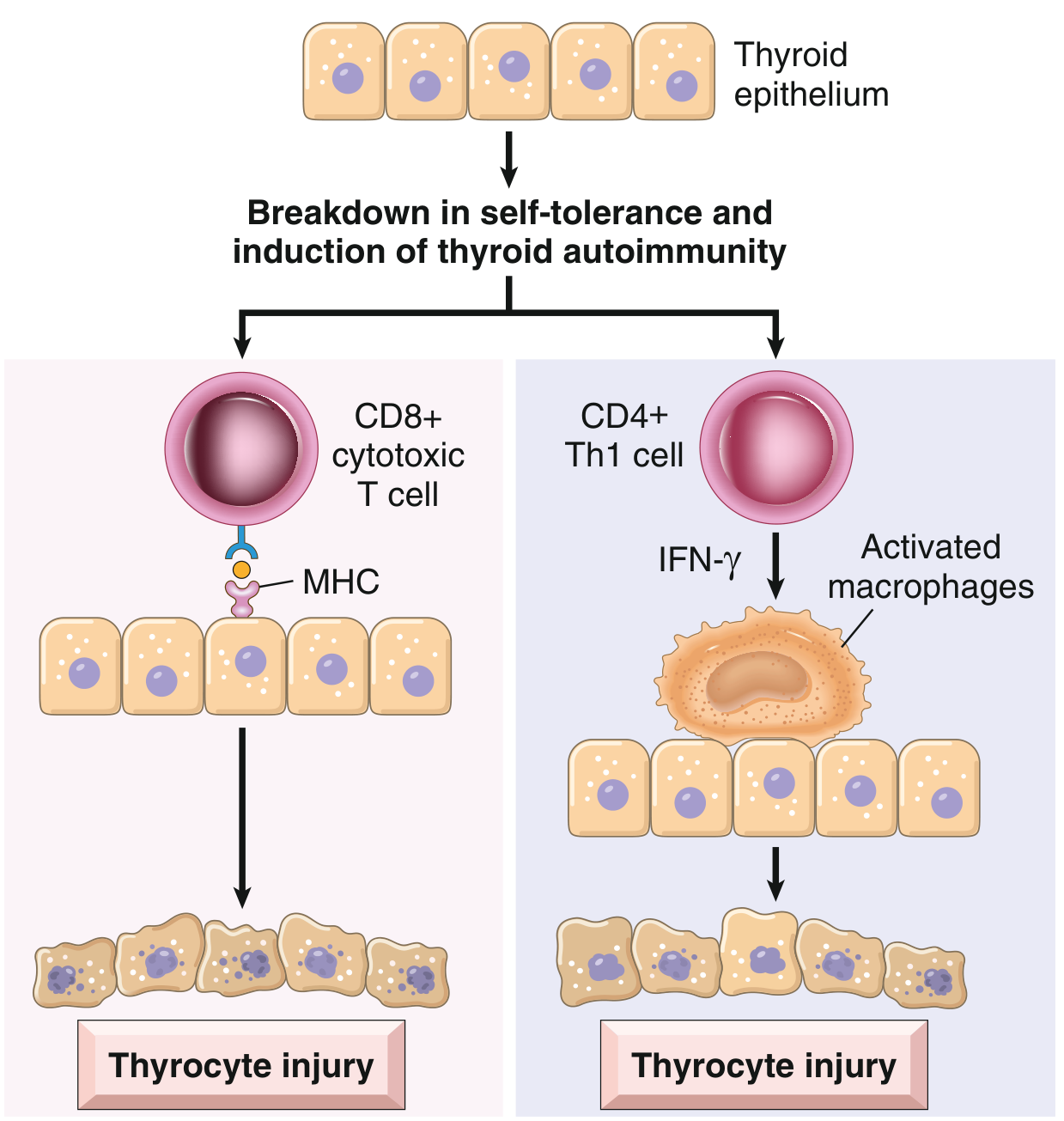
Three major immune mechanisms operate:
- CD8+ cytotoxic T cells - directly kill thyroid epithelial cells via MHC class I recognition
- CD4+ Th1 cytokines - secretion of IFN-γ recruits and activates macrophages, which destroy follicles; TNF-α and IL-1 are also implicated
- Autoantibodies - anti-TPO (antimicrosomal) and antithyroglobulin antibodies are present in nearly all patients and may cause damage via antibody-dependent cell-mediated cytotoxicity (ADCC) or complement activation; though whether these are cause or consequence of injury remains debated
Genetic factors:
- ~40% concordance in monozygotic twins
- ~50% of asymptomatic siblings have antithyroid antibodies
- HLA-DR3, DR4, DR5 (Caucasians) are the strongest genetic risk factors
- Polymorphisms in CTLA-4 (T-cell inhibitor) and PTPN22 increase susceptibility
- Associated with Down syndrome (chromosome 21 gene) and Turner syndrome
- Shared genetic risk with type 1 DM, Addison's disease, pernicious anemia, vitiligo
Environmental factors: High iodine intake, low selenium, reduced childhood microbial exposure, and smoking cessation transiently increase risk. Alcohol use appears protective.
- Robbins & Kumar Basic Pathology, p. 731-732; Harrison's 22E, p. 3072-3073
Morphology / Histology
Gross: Thyroid is usually diffusely and symmetrically enlarged, firm. In atrophic thyroiditis, the gland is small and scarred.

Microscopic (key features):
-
Widespread lymphocytic infiltrate with lymphocytes, plasma cells, macrophages
-
Well-developed germinal centers (lymphoid follicle formation)
-
Atrophic thyroid follicles with scant colloid
-
Hürthle (oxyphil) cell metaplasia - follicular epithelium replaced by cells with abundant eosinophilic granular cytoplasm packed with mitochondria (a metaplastic response to injury)
-
Increased interstitial fibrosis
-
Robbins & Kumar Basic Pathology, p. 732; Harrison's 22E, p. 3072
Clinical Features
Presentation:
- Painless, diffuse, firm thyroid enlargement (goiter) - most common presentation
- Symptoms of hypothyroidism (weight gain, fatigue, cold intolerance, constipation, dry skin, bradycardia, delayed reflexes)
- Less commonly, transient thyrotoxicosis (Hashitoxicosis) at disease onset due to follicular disruption releasing preformed hormone
- Globus sensation, profound fatigue, muscle/joint pain, poor sleep, dry mouth/eyes - these may persist even with adequate thyroid hormone replacement (thought to be autoimmune-related)
- Compressive symptoms in large goiters: dyspnea, dysphagia, cough, hoarseness
Thyroid status progression:
- Euthyroid phase (compensation: TSH rises, T4 normal = subclinical hypothyroidism)
- Overt hypothyroidism (TSH typically >10 mIU/L, free T4 falls)
- Atrophic end stage
Associated conditions: Graves' disease (can coexist or evolve), other autoimmune diseases (DM type 1, Addison's, pernicious anemia, vitiligo), Down syndrome, Turner syndrome
Malignancy risk:
-
Higher incidence of thyroid lymphoma (primary thyroid lymphoma almost always arises in a background of Hashimoto thyroiditis)
-
Increased incidence of papillary thyroid carcinoma (disputed; may cause false-positive FNAB results)
-
Current Surgical Therapy 14e, p. 885-886; Harrison's 22E, p. 3072
Diagnosis
| Test | Finding |
|---|---|
| TSH | Elevated (subclinical or overt hypothyroidism) |
| Free T4 | Low (in overt hypothyroidism); normal (subclinical) |
| Anti-TPO antibodies | Elevated in nearly all patients (most sensitive) |
| Antithyroglobulin antibodies | Elevated in many patients |
| Ultrasound | Diffusely heterogeneous, hypoechoic gland; may show nodules |
| FNAB | Indicated for nodules; shows follicular cells, colloid, lymphocytes, Hürthle cells (Bethesda II = benign) |
-
Positive TPO antibodies + elevated TSH usually clinch the diagnosis without biopsy
-
FNAB findings: Bethesda III (AUS), IV (Hürthle cell neoplasm), or V (suspicious for PTC) may occur due to Hürthle cell changes causing false-positive results
-
Schwartz's Principles of Surgery 11e; Current Surgical Therapy 14e
Treatment
Medical
- Euthyroid, asymptomatic patients: no treatment required; monitor TSH
- Hypothyroidism: levothyroxine (LT4) replacement
- Starting dose: 1.6 mcg/kg/day (weight-based)
- Titrate to normalize TSH
- Subclinical hypothyroidism: treat if TSH >10 mIU/L, or if symptomatic, pregnant, or TPO antibody-positive with progressive rise in TSH
- Hashitoxicosis: beta-blockers for symptom control; antithyroid drugs generally not needed (transient)
- Persistent symptoms despite adequate LT4 replacement (fatigue, pain, cognitive symptoms) do not routinely improve with additional thyroid hormone; thought to be autoimmune-mediated
Surgical
Surgery is rarely necessary but indicated for:
- Thyroid nodule with indeterminate or malignant FNAB (Bethesda III-VI)
- Unilateral or bilateral thyromegaly with mass effect/compressive symptoms (tracheal compression, dysphagia, hoarseness)
- Persistent symptoms despite adequate thyroid hormone replacement (emerging evidence)
Procedure choice:
- Disease limited to one lobe: lobectomy + isthmusectomy
- Most patients: total thyroidectomy
Evidence for surgery in persistent symptoms: The Norwegian Trial on Surgery for Hashimoto Disease (prospective RCT) showed total thyroidectomy vs. hormone therapy alone improved health-related quality of life, fatigue scores, and normalized anti-TPO titers in histologically verified Hashimoto patients.
Surgical note: The firm, inflamed gland can be difficult to retract; traction on the recurrent laryngeal nerve (RLN) is a risk. Intraoperative nerve monitoring is recommended. Enlarged reactive central neck lymph nodes can mimic thyroid cancer - frozen section can differentiate.
- Current Surgical Therapy 14e, p. 886; Harrison's 22E
Hashimoto Variants & Related Conditions
| Condition | Relationship |
|---|---|
| Atrophic thyroiditis | End stage of Hashimoto; extensive fibrosis, near-total follicle loss |
| Painless (silent) thyroiditis | Variant of Hashimoto; autoimmune follicular destruction causing transient hyperthyroidism |
| Postpartum thyroiditis | Specific type of painless thyroiditis; occurs within 1 year of delivery/abortion; up to 10% of pregnancies |
| Fibrosing variant | Rare; marked IgG4+ plasma cell infiltrate; mimics Riedel thyroiditis |
| Hashitoxicosis | Transient thyrotoxicosis from Hashimoto follicular rupture |
Key Associations & Complications
- Primary thyroid lymphoma (MALT type) - nearly always in Hashimoto background; suspect with rapid gland enlargement
- Papillary thyroid carcinoma - possible increased risk (TSH-driven); Hashimoto can cause false-positive FNAB
- Hashimoto encephalopathy - rare steroid-responsive encephalopathy with high antithyroid antibodies, often euthyroid
- Polyglandular autoimmune syndromes (Type 2 includes Hashimoto + Addison's + T1DM)
- Increased prevalence in iodine-replete populations; iodine excess can accelerate thyroid autoimmunity
Sources: Robbins & Kumar Basic Pathology (p. 731-732), Harrison's Principles of Internal Medicine 22E (p. 3072-3074), Current Surgical Therapy 14e (p. 885-886), Schwartz's Principles of Surgery 11e
This is a shared conversation. Sign in to Orris to start your own chat.