Blair incision, modified Blair and extended Blair incisions
Reading File
Finding Sources
Finding Sources
Searching the Web
Blair incision modified Blair extended Blair parotid surgery anatomy
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Blair Incision, Modified Blair Incision, and Extended Blair Incision
All three are incisions used in parotid gland surgery (parotidectomy), each offering a different trade-off between exposure, extensibility, and cosmesis.
1. Blair Incision (Original)
The original Blair incision is the simplest of the three:
- A straight preauricular incision running vertically in front of the ear, curving slightly inferior to the ear lobule
- It provides direct access to the parotid gland but has limited exposure of the neck and is rarely used in its original form today
Bailey & Love's Short Practice of Surgery, 28th ed.
2. Modified Blair Incision (Bailey's Modification / "Lazy-S")
This is the workhorse incision for most parotid surgery - it is what surgeons mean when they say "Blair incision" in modern practice.
Bailey modified the inferior segment of the original Blair incision to redirect it towards the mastoid and along the anterior border of the sternocleidomastoid muscle (SCM). This evolved into the modern "lazy S" incision, which has three components:
| Component | Location |
|---|---|
| Vertical | Preauricular, close to the tragus in a skin crease |
| Communicating | Gently curves below the ear lobule |
| Horizontal | Along a natural skin crease, two finger-breadths from the angle of the mandible |
Modified Blair incision marking - Bailey & Love's, Fig. 54.12(a)
Cummings Otolaryngology describes the incision as starting "in a preauricular crease, extending superiorly to the level of the root of the helix, extending inferiorly around the lobule of the ear over the mastoid tip, then gently curving down along the SCM and slightly forward in a natural skin crease in the upper neck."
Flap elevation technique (Bailey & Love)
- The horizontal (cervical) component is incised first to identify the platysma, the external jugular vein, and the greater auricular nerve
- The vertical (preauricular) component is then incised and connected inferiorly
- A subplatysmal flap is raised - the platysma is divided, and the flap is elevated remaining below the SMAS (superficial musculoaponeurotic system), lifting subcutaneous fat off the parotid gland
- Flap elevation proceeds anteriorly over the parotid but not onto the masseteric fascia, to avoid damaging nerve branches exiting the gland
Right superficial parotidectomy - Cummings Otolaryngology, Fig. 84.25
Indications
- Superficial parotidectomy
- Total parotidectomy
- Combined parotidectomy + neck dissection (the cervical limb permits excellent neck access)
- First branchial cleft anomalies (Work type II) - allows identification of the facial nerve trunk
- Both benign and malignant parotid tumours
3. Extended Blair Incision
The extended Blair incision expands the surgical field further for cases requiring wider access, particularly for skull base and infratemporal fossa approaches.
Scott-Brown's Otorhinolaryngology describes it in the context of the subtemporal preauricular approach to the infratemporal fossa:
- An extended Blair incision is made to raise a cervicofacial flap
- It allows identification and preservation (or controlled sacrifice) of the facial nerve trunk and major branches
- Used when resection involves structures such as the nasopharynx/oropharynx, infratemporal fossa, petrous ICA, or cavernous sinus
Extended Blair incision for the subtemporal preauricular approach - Scott-Brown's Vol. 2, Fig. 109.6(a)
The figure above illustrates the key feature of the extended variant: it sweeps up into the temporal scalp (above the zygomatic arch and ear) and curves down into the neck, enabling a wide cervicofacial flap to be raised and the entire lateral skull base to be accessed.
Comparison Summary
| Feature | Blair (Original) | Modified Blair | Extended Blair |
|---|---|---|---|
| Preauricular component | Yes | Yes | Yes |
| Cervical extension | No | Yes (along SCM) | Yes (longer) |
| Temporal/scalp extension | No | No | Yes |
| Flap type | Preauricular skin flap | Subplatysmal cervicofacial flap | Wide cervicofacial flap |
| Primary use | Historic; basic parotid access | Standard parotidectomy | Skull base / infratemporal fossa surgery |
| Cosmesis | Poor neck concealment | Good (follows skin creases) | Scar extends into hairline |
| Extensibility | Limited | Good (neck dissection possible) | Excellent |
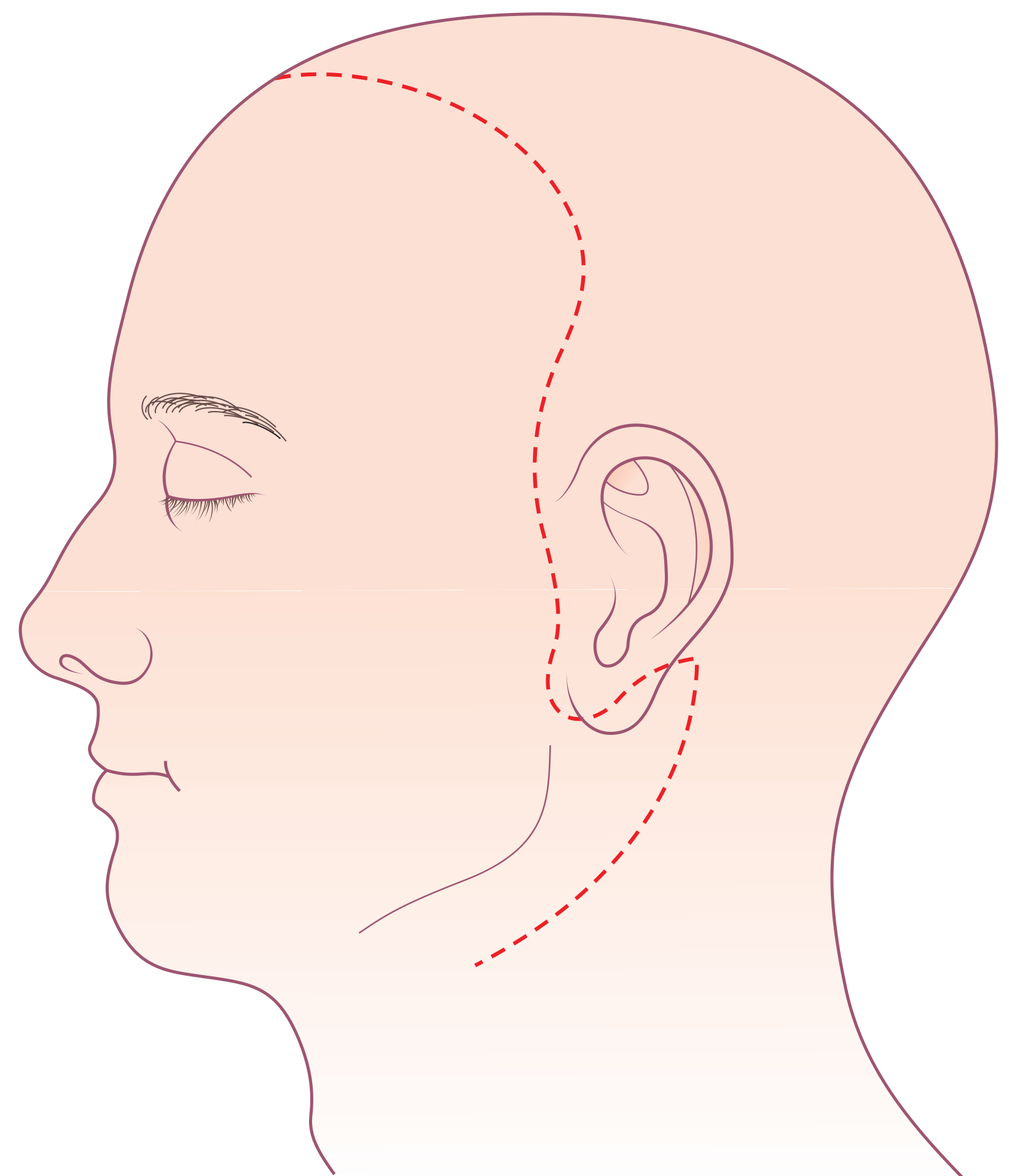
Alternatives: The Facelift Incision
For cosmetically-sensitive patients with benign tumours, the modified Blair incision is compared to the facelift (rhytidectomy) incision:
- The preauricular portion is similar to the modified Blair
- The posterior limb curves at right angles behind the ear, into the hairline, avoiding any visible neck incision
- It offers superior cosmesis but limited neck access - making it unsuitable when simultaneous neck dissection is needed
- A 2021 meta-analysis (PMC8677756) compared the two approaches
Sources: Bailey & Love's Short Practice of Surgery (28th ed.), Cummings Otolaryngology Head & Neck Surgery, Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, Mulholland & Greenfield's Surgery, Fischer's Mastery of Surgery (8th ed.)
Doubly modified Blair incision
Finding Sources
Finding Sources
Searching the Web
doubly modified Blair incision parotid surgery retroauricular
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all I need. Here is a comprehensive answer:
Doubly Modified Blair Incision
What it is
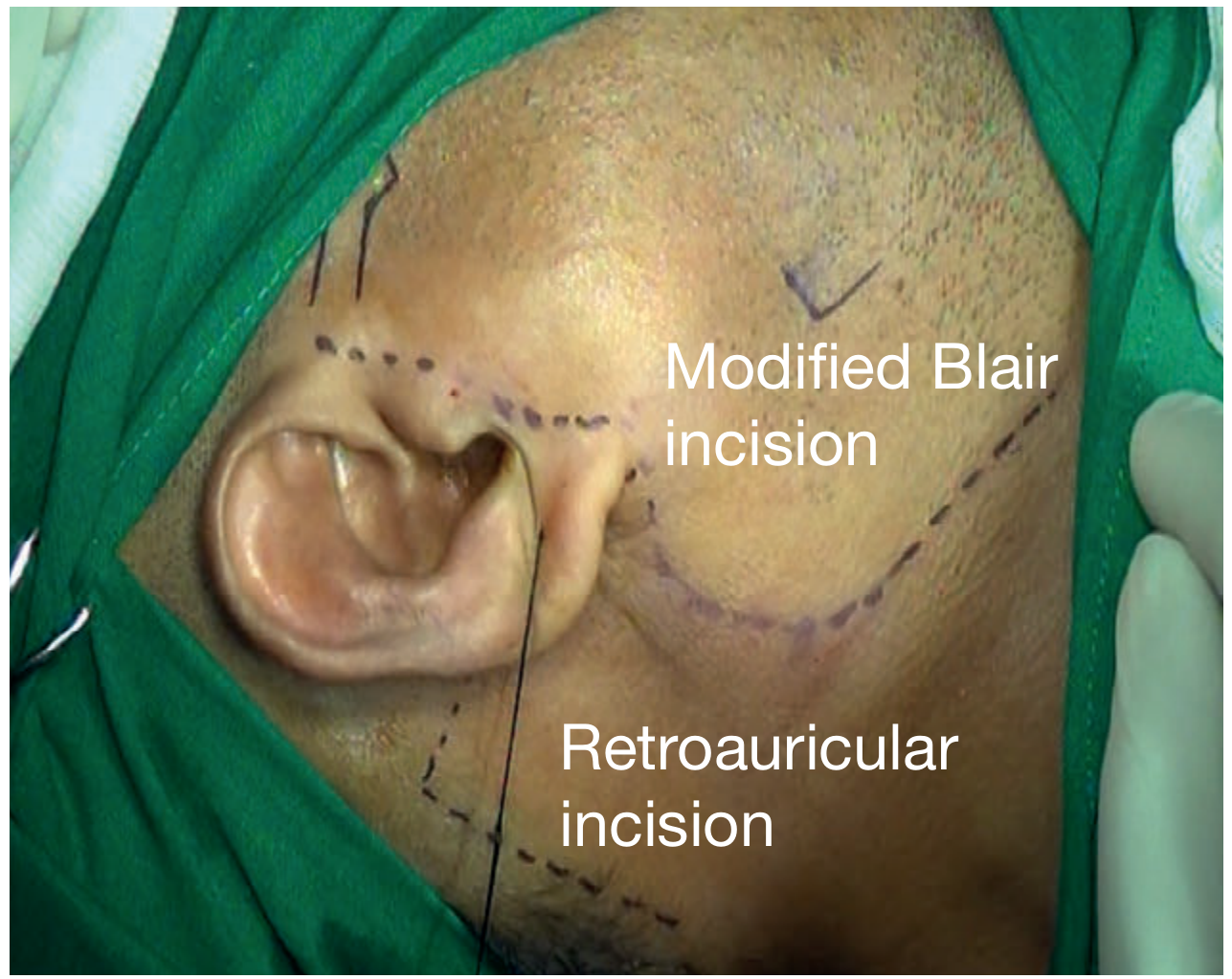
The "doubly modified Blair's incision" is the standard modified Blair incision (the preauricular-to-cervical "lazy S") with a second modification: addition of a retroauricular (post-auricular) limb that curves behind the ear into the mastoid/post-auricular sulcus region. As Bailey & Love's figure legend explicitly states, it involves "the modified Blair incision and the retroauricular incision" planned together (Fig. 54.12a).
Incision planning: the modified Blair incision (preauricular/cervical) + retroauricular extension - Bailey & Love's, Fig. 54.12(a)
The Two Modifications
| Modification | What it adds vs. original Blair |
|---|---|
| First modification (Bailey's / "lazy S") | Inferior cervical limb directed toward mastoid and along anterior border of SCM, following a natural skin crease in the neck |
| Second modification (retroauricular limb) | A post-auricular component curving behind the ear lobule and ascending along the post-auricular sulcus toward the mastoid, then optionally extending into the hairline |
The result is a compound incision with three zones of access: preauricular (anterior to the ear), cervical (below and forward into the neck), and retroauricular (behind the ear).
Purpose and Indications
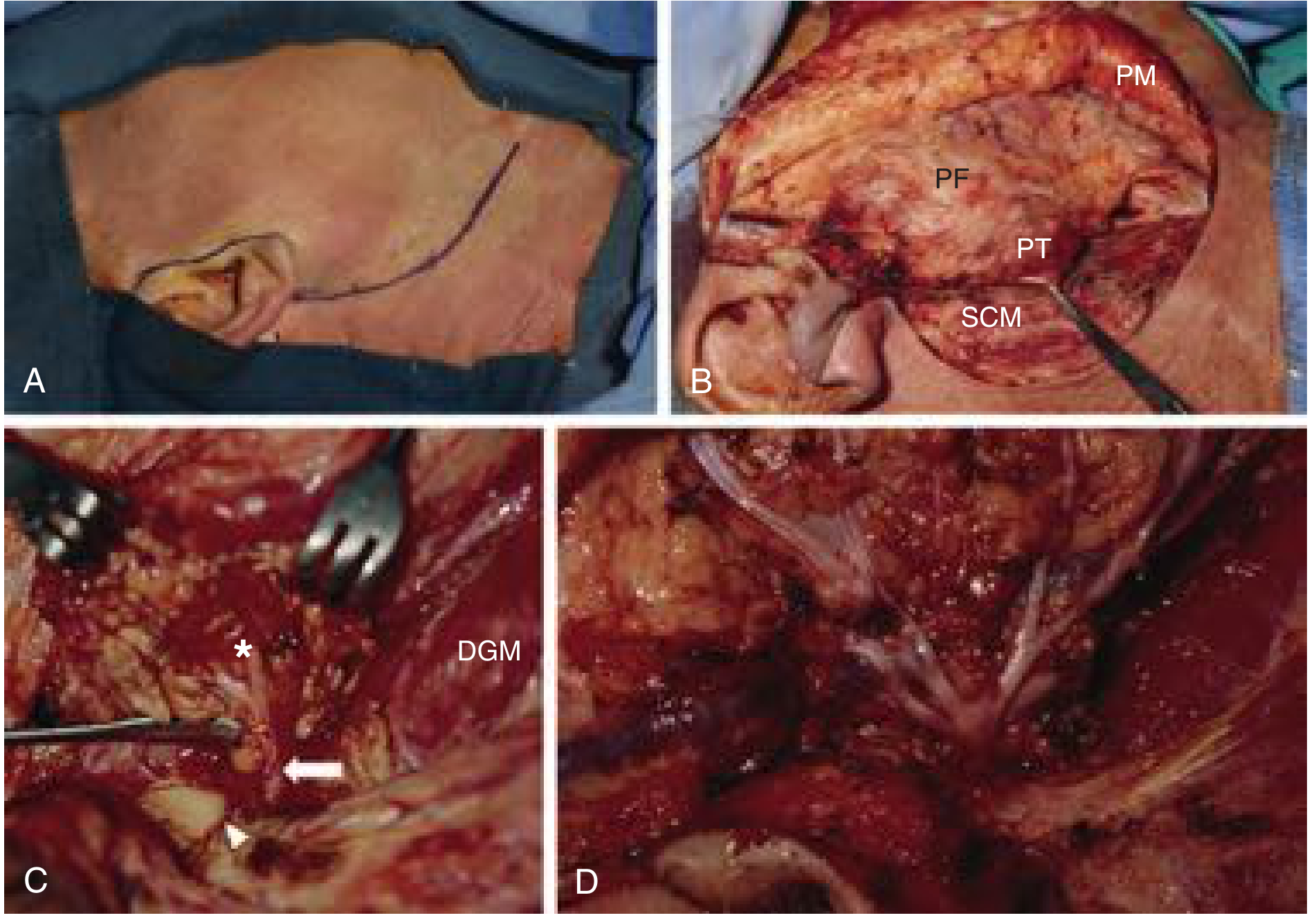
Scott-Brown's Otorhinolaryngology describes the doubly modified Blair's incision specifically in the context of the transcervical-transparotid approach to the parapharyngeal space:
"The operation is performed through a doubly modified Blair's incision as in a routine parotidectomy with a slight anterior extension of the cervical incision."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol. 1), Chapter 11 - Parapharyngeal space tumours
This approach is used in approximately 27% of parapharyngeal space cases and is well-suited for:
- Deep lobe parotid tumours extending into the parapharyngeal space (e.g., "dumbbell tumours" - pleomorphic adenoma with a deep lobe component passing through the stylomandibular tunnel)
- Vascular parapharyngeal tumours - the cervical limb gives access to the carotid artery and internal jugular vein for proximal control
- Malignant lesions of the parapharyngeal space requiring parotidectomy + neck dissection
- Cases where a standard parotidectomy is combined with wide posterior and inferior flap mobilisation

Transcervical-transparotid approach for a large "dumbbell" parapharyngeal pleomorphic adenoma performed through the doubly modified Blair's incision - Scott-Brown's, Fig. 11.9(b)
Why the Retroauricular Limb Matters
Adding the post-auricular component achieves several things:
- Posterior flap mobilisation - allows the skin/SMAS flap to be reflected further anteriorly without tension, improving access to the deep lobe and parapharyngeal space
- Mastoid and stylomastoid foramen access - facilitates retrograde facial nerve identification in difficult or revision cases
- Vascular pedicle protection - prevents flap ischaemia at the angle between the preauricular and cervical limbs by reducing tension at the curve behind the lobule
- Extensibility - can be extended superiorly into the temporal hairline if skull base access is required (merging with the extended Blair concept)
Progression of Blair Incision Variants
Original Blair (1918)
↓ + cervical limb toward mastoid/SCM
Modified Blair (Bailey, 1941) = "lazy S"
↓ + retroauricular limb behind the ear
Doubly Modified Blair
↓ + temporal scalp extension
Extended Blair (for skull base / infratemporal fossa)
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 (p. 208); Bailey & Love's Short Practice of Surgery 28th ed. (p. 868, Fig. 54.12a)
Benign tumours of parotid gland
Finding Sources
Finding Sources
Searching the Web
benign parotid gland tumours classification pleomorphic adenoma Warthin's 2024
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from all the major textbooks. Here is the full answer:
Benign Tumours of the Parotid Gland
Overview and Epidemiology
Approximately 80% of parotid tumours are benign. Salivary gland neoplasms as a whole account for fewer than 3% of all tumours. The parotid is the most commonly affected gland (about 80% of all salivary gland tumours), and of these, benign tumours predominate. Benign tumours are often present for months to years before coming to clinical attention due to their slow growth.
WHO Classification of Benign Epithelial Salivary Gland Tumours
| Tumour |
|---|
| Pleomorphic adenoma (most common) |
| Myoepithelioma |
| Basal cell adenoma |
| Warthin's tumour |
| Oncocytoma |
| Lymphadenoma |
| Cystadenoma |
| Sialadenoma papilliferum |
| Ductal papillomas |
| Sebaceous adenoma |
| Canalicular adenoma |
Scott-Brown's Otorhinolaryngology, Vol. 2 - Table 26.5
1. Pleomorphic Adenoma (Benign Mixed Tumour)
Epidemiology
- Most common salivary gland tumour overall - 50% of all salivary gland tumours, 65% of parotid tumours, 40% of minor salivary gland tumours
- Annual incidence: 2.4-3.05 per 100,000
- Peak age: 3rd-6th decade; average presentation age 45 years
- More frequent in women
- Predominantly in the superficial lobe of the parotid; a significant proportion arise in or involve the deep lobe
- Can also arise from accessory parotid tissue along the parotid duct, the submandibular gland, or minor salivary glands (e.g. soft palate)
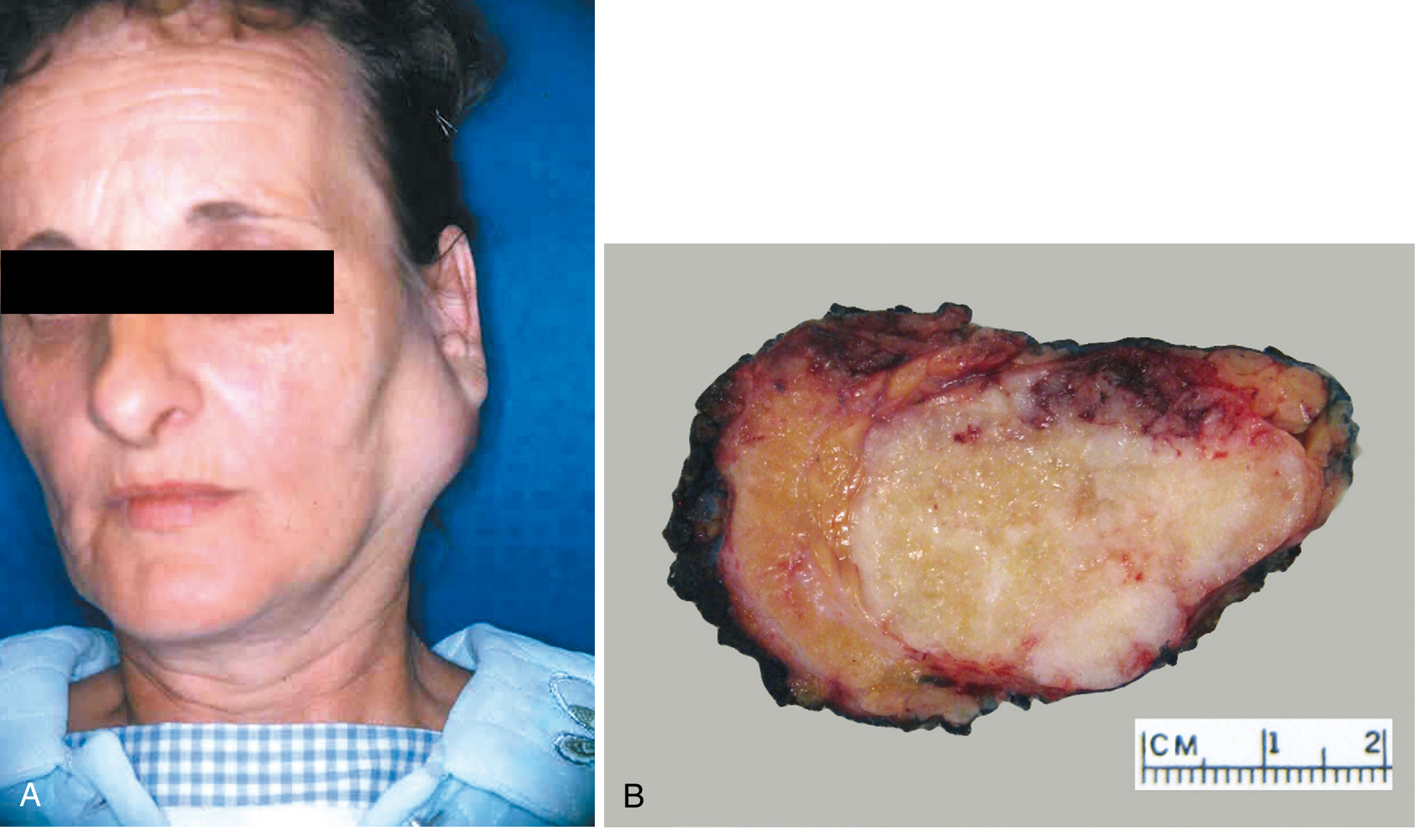
Clinical Features
- Painless, well-defined, solitary, mobile mass with gradual progression over many years
- Can reach enormous proportions if untreated
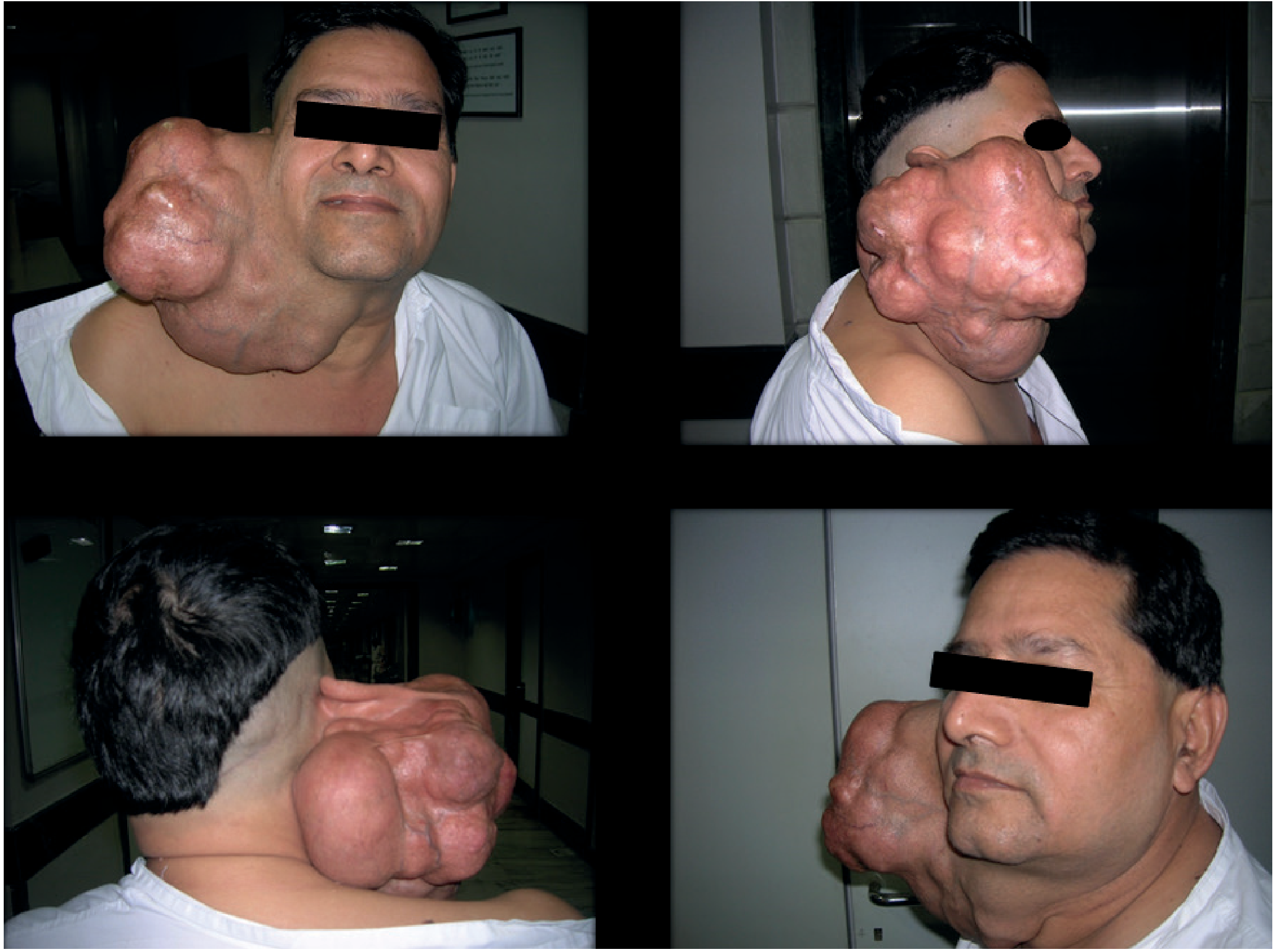
- Deep lobe tumours may present as a paratonsillar bulge
- Sudden increase in size or facial nerve palsy suggests malignant transformation
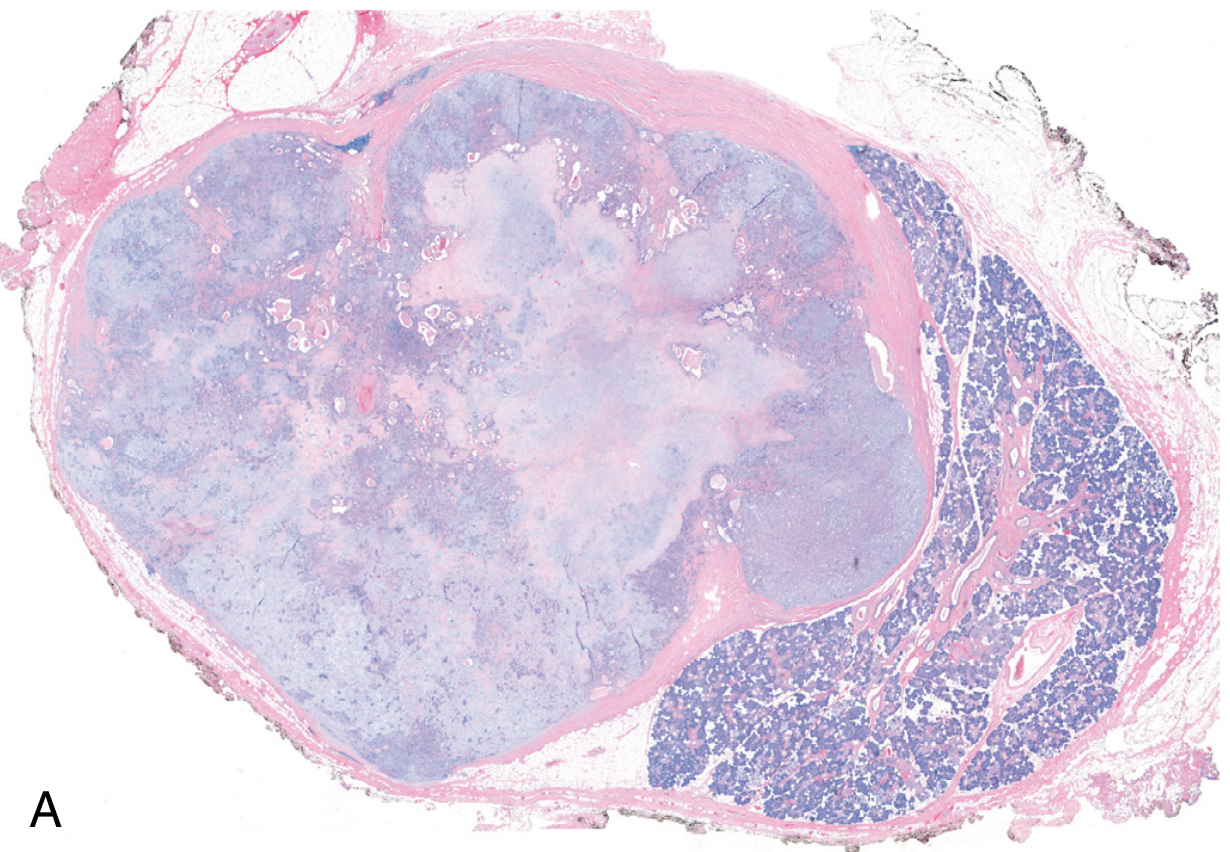
Pathology
Macroscopy: Well-demarcated, rounded, nodular mass with bosselations. Cut surface shows solid grey/white areas with blue translucent chondromyxoid stroma; cystic change in large tumours. Protuberant pericapsular nodules may be attached by a slender pedicle.
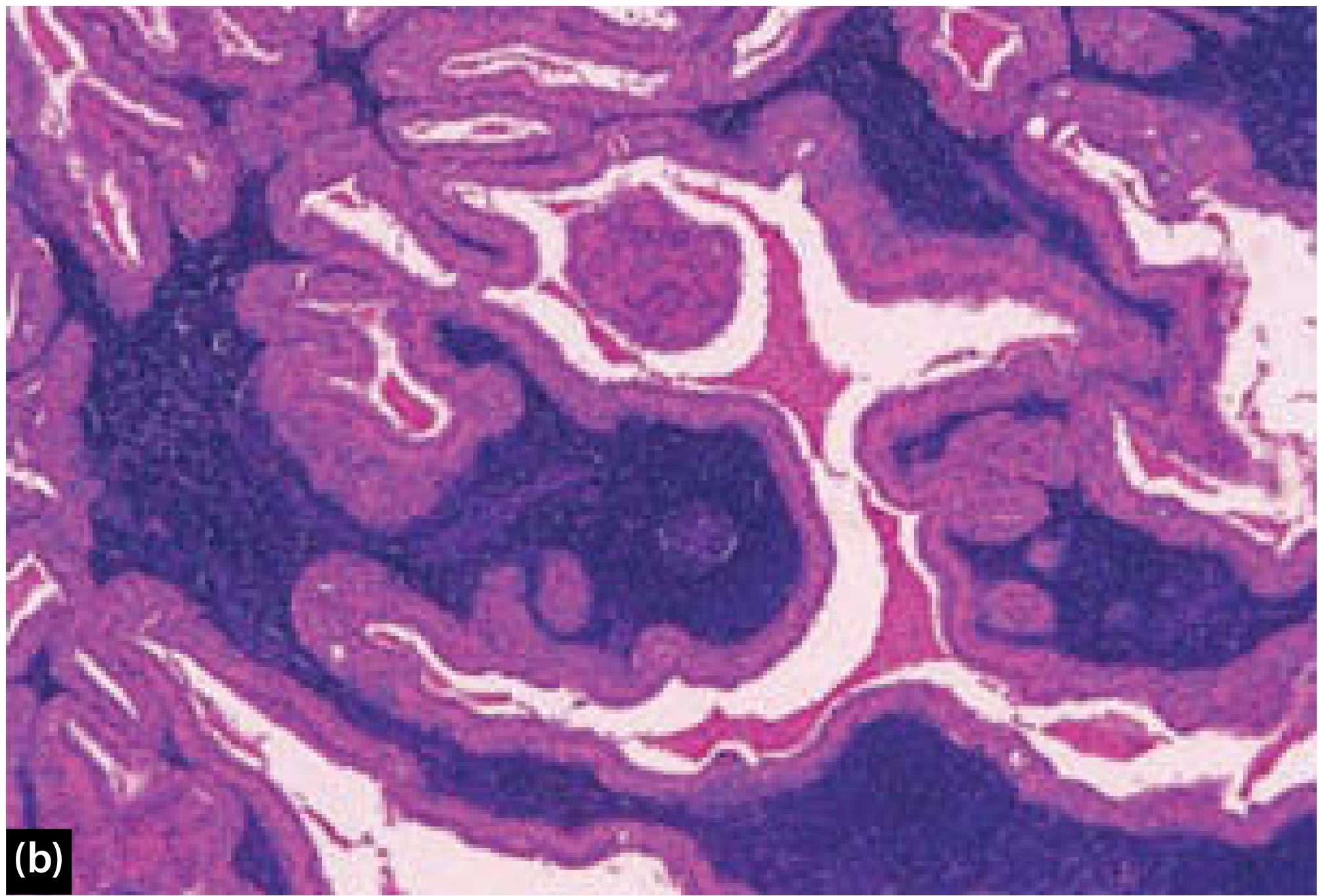
Microscopy: The hallmark is morphologic heterogeneity (not nuclear pleomorphism). Three components:
- Ductal (epithelial) cells - form ducts, acini, tubules, or sheets
- Myoepithelial cells - spindle, plasmacytoid, clear cell, or epithelioid morphology
- Chondromyxoid stroma - the most characteristic feature; may contain true cartilage, calcification, or even bone (the only salivary tumour to do so)
Squamous metaplasia with keratinization is common and does not imply malignancy. In IHC: luminal cells express CK7 (strong/diffuse); myoepithelial cells express p63, S-100, SOX10, SMA.
Molecular: Many cases have chromosomal rearrangements inducing overexpression of PLAG1 (a transcription factor promoting cell growth); others have HMGA2 gene mutations.
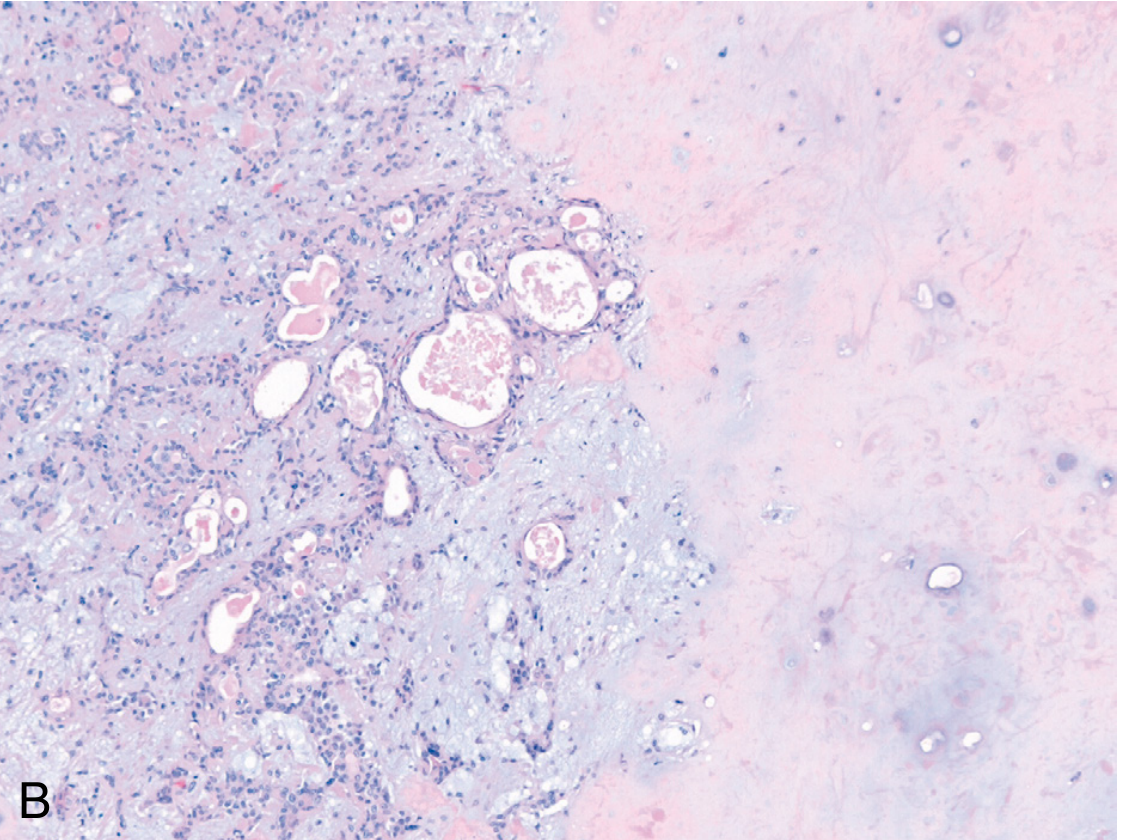
The Capsule - Critical Surgical Point
- The capsule is exceptionally thin (<20 microns) in at least one area in virtually all pleomorphic adenomas
- Incomplete in ~50%, especially the myxoid/mucoid type (most prone to operative rupture)
- Rupture during surgery seeds the operative field and significantly increases the risk of multifocal recurrence
- This is why enucleation is absolutely contraindicated - recurrence rate after simple enucleation approaches 25%, vs ~4% after formal parotidectomy
Risk of Malignant Transformation (Carcinoma Ex Pleomorphic Adenoma)
- Overall risk: ~6% (Scott-Brown's); correlates strongly with duration:
- <5 years: ~2%
-
15 years: ~10% (Robbins)
- Risk factors: older age, male sex, long duration, multiple recurrences, deep lobe location
- The resultant carcinoma is among the most aggressive of salivary gland malignancies: mortality 30-50% at 5 years
Treatment
- Partial superficial parotidectomy (tumour + cuff of normal tissue) - most common practice in UK
- Total superficial parotidectomy for larger tumours or where cuff cannot be achieved
- Deep lobe tumours: total parotidectomy, usually via a transcervical-transparotid approach
- Submandibular gland: excision of the entire gland (extracapsular)
- Minor salivary glands: wide local excision
- Enucleation must be avoided
2. Warthin's Tumour (Adenolymphoma / Papillary Cystadenoma Lymphomatosum)
Epidemiology
- Second most common benign parotid tumour (5-15% of benign parotid tumours; up to 20% by some series)
- Almost exclusively in the parotid gland - rare in the submandibular gland (which contains no lymphoid tissue)
- Peak incidence: 6th-7th decade
- Formerly quoted as strongly male-predominant (10:1); more recent series show male:female ratio of only ~1.6:1, suggesting sex distribution is becoming more equal
- Strong association with cigarette smoking (risk increased 8-fold) and secondly with radiation exposure
- Rare in Afro-Caribbeans/Black Africans; more common in Caucasians and Asians
- Multifocal in ~10%, bilateral in 4-10% of cases - the most commonly bilateral salivary gland tumour
- Can occur synchronously with pleomorphic adenoma
Clinical Features
- Slow-growing, soft, painless swelling at the lower pole of the parotid gland
- Facial palsy is rare
Pathology
Macroscopy: Circumscribed, thinly encapsulated, soft mass. Cut surface shows multiple cystic and papillary areas with white-to-brown colour; tan coagulated exudate in cystic spaces.
Microscopy: The two-component hallmark:
- Bilayered oncocytic epithelium - inner columnar + outer cuboidal cells; the term "oncocyte" refers to large cells with abundant granular eosinophilic cytoplasm packed with mitochondria; papillary projections lining cysts
- Reactive lymphoid stroma with germinal centres (explains the near-exclusive parotid location - the parotid uniquely contains intraparotid lymph nodes where ductal epithelial inclusions are thought to give rise to the tumour)
Histogenesis controversy: Polyclonal studies suggest a non-neoplastic/reactive origin (salivary duct inclusions in intraparotid lymph nodes); other work suggests clonal origin with a fusion oncogene.
Malignant Transformation
- Extremely rare (<1%) and may represent dual pathology rather than true transformation
- Can be carcinomatous (adenocarcinoma, SCC, or undifferentiated) or lymphomatous change
Treatment
- FNAC is often diagnostic
- Formal excision: partial superficial parotidectomy
- Given the very low malignant potential, the elderly age group, and the possibility of no growth, conservative observation alone is acceptable in selected patients
- Recurrence after excision: very rare (~2%), may represent multifocal disease
3. Other Benign Parotid Tumours (Less Common)
Oncocytoma
- Composed entirely of oncocytes (mitochondria-rich cells)
- Rare, <1% of salivary gland tumours
- Older patients; treated by surgical excision
Myoepithelioma
- Composed almost entirely of myoepithelial cells (no ductal differentiation, unlike pleomorphic adenoma)
- Most common in the parotid
- Treated by excision
Basal Cell Adenoma
- Uniform basaloid cells; no chondromyxoid stroma (distinguishes from pleomorphic adenoma)
- Most common in the parotid
- Low recurrence rate; treated by excision
Canalicular Adenoma
- Almost exclusively in minor salivary glands (especially upper lip)
- Rare in parotid
Benign Mesenchymal Tumours (within or adjacent to the parotid)
- Schwannoma/Neurilemmoma - benign encapsulated tumour from Schwann cells; may arise from the facial nerve or its branches within the parotid; NF2 gene inactivation in 67%
- Haemangioma - most common benign parotid tumour in children; may involute spontaneously
- Lipoma, fibroma, lymphangioma (rare)
Summary Comparison
| Feature | Pleomorphic Adenoma | Warthin's Tumour |
|---|---|---|
| Frequency | 65% of parotid tumours | 5-20% of benign parotid tumours |
| Age | 3rd-6th decade | 6th-7th decade |
| Sex | More in women | More in men (ratio narrowing) |
| Location | Any part of parotid; superficial lobe most common | Lower pole of parotid, almost exclusively |
| Bilateral | Rare | 4-10% |
| Smoking link | No | Strong (8x risk) |
| Consistency | Firm/hard (chondroid) to soft (myxoid) | Soft, cystic |
| Histology | Ductal + myoepithelial cells + chondromyxoid stroma | Bilayered oncocytic epithelium + lymphoid stroma |
| Calcification/bone | Can occur (pathognomonic) | Never |
| Malignant risk | ~6%, time-dependent | <1% (exceedingly rare) |
| Recurrence after surgery | ~4% (25% if enucleated) | ~2% |
| Treatment | Parotidectomy with cuff; enucleation forbidden | Partial parotidectomy; observation acceptable |
| Tc-99m scan | Cold | Hot (characteristic) |
Sources: Bailey & Love's Short Practice of Surgery (28th ed.); Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 & Vol. 2; Robbins & Cotran Pathologic Basis of Disease; Cummings Otolaryngology Head & Neck Surgery
Pleomorphic adenoma of parotid gland
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
pleomorphic adenoma parotid management extracapsular dissection recurrence 2024
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive multi-source content. Let me compile the full answer:
Pleomorphic Adenoma of the Parotid Gland
Definition and Nomenclature
Pleomorphic adenoma (PA) is also called benign mixed tumour - the term "pleomorphic" refers to its remarkable morphologic heterogeneity (diverse tissue components), not nuclear pleomorphism. It is the most common tumour of the salivary glands and the most common tumour of the parotid gland.
Epidemiology
- Annual incidence: 2.4-3.05 per 100,000
- Accounts for ~50% of all salivary gland tumours, 65% of parotid tumours, and 40% of intraoral minor salivary gland tumours
- Can occur at any age, but most commonly between the 3rd and 6th decade (average age of presentation: 45 years)
- More frequent in women
- Radiation exposure is the one established risk factor
Sites
- Parotid gland >80% - most commonly within the superficial lobe, but a significant proportion arise from or involve the deep lobe by direct growth
- Can also arise from accessory parotid tissue along the duct (only visible when mouth opens as coronoid pushes it anteriorly)
- Submandibular gland
- Hard palate and other minor salivary glands (most common minor salivary site: hard palate)
Clinical Features
- Painless, well-defined, solitary, mobile mass with slow, gradual progression over many years
- Can reach enormous size if untreated
- Deep lobe tumours: present as a paratonsillar bulge or oropharyngeal mass
- Sudden increase in size or facial nerve palsy = red flags for malignant transformation
- Occasional metachronous or synchronous tumours
- Deep lobe tumours may present with dysphagia or a "dumbbell" parapharyngeal mass
Pathology
Macroscopic Appearance
- Well-demarcated, rounded/ovoid with broad-based bosselations
- Variably encapsulated - capsule may be thick and fibrotic or attenuated and incomplete
- Cut surface: solid, homogeneous or variegated blue/grey hue from chondromyxoid matrix; may show cystic change, calcification, or cartilage

Pericapsular nodules: Protuberant nodules may be attached by a slender pedicle to the main tumour body - enucleation risks detaching these, leaving behind a nidus for recurrence.
Microscopic Appearance
The dominant feature is morphologic heterogeneity. Three basic components:
- Ductal (epithelial) elements - cuboidal to columnar cells forming ducts, acini, tubules, strands, or sheets
- Myoepithelial cells - arranged as spindle, plasmacytoid, epithelioid, or clear cells; form the outer layer of duct structures
- Chondromyxoid (mesenchymal) stroma - the most characteristic feature; loose myxoid tissue with islands of cartilage (though often called "pseudo-cartilage" it is true cartilage histologically), hyaline tissue, and rarely bone - calcification or bone formation is found only in pleomorphic adenoma among salivary gland tumours, making it pathognomonic
A wide range of other changes can occur: squamous metaplasia (common - does not imply malignancy), lipomatous, osseous, neuroid, angiomatoid metaplasia; cystic change; infarction; hyalinisation; elastosis.
Immunohistochemistry
| Cell type | Markers |
|---|---|
| Luminal (ductal) cells | CK7 (strong, diffuse) |
| Myoepithelial cells | p63, S-100, SOX10, SMA |
Molecular Genetics
- Many cases: chromosomal rearrangements causing overexpression of PLAG1 (transcription factor promoting growth factor receptor signalling genes)
- Cases lacking PLAG1 overexpression: HMGA2 gene mutations (encodes a DNA-binding protein)
- All tumour elements - including the apparently mesenchymal stroma - are thought to be of intercalated duct reserve cell (stem cell) and myoepithelial cell origin
The Capsule - The Central Surgical Problem
This is the most clinically important feature of pleomorphic adenoma:
- The capsule is exceptionally thin (<20 microns) in at least one area in virtually all pleomorphic adenomas
- Incomplete in approximately 50%, especially the myxoid/predominantly mucoid type
- Myxoid stroma can bulge into normal gland parenchyma without any capsule intervening
- The predominantly mucoid types are semi-fluid and fluctuant - highly prone to intraoperative capsular rupture and spillage, seeding the operative field
- Such recurrences are typically multifocal
Why enucleation is contraindicated:
- Recurrence rate after simple enucleation: ~25%
- After formal parotidectomy with cuff: ~4%
- Even with "standard" superficial parotidectomy: 81% had some degree of capsule exposure, and >50% of surface was exposed in 60% of cases - meaning a capsule-free margin is practically impossible to achieve consistently adjacent to the facial nerve
Investigations
FNAC (Fine Needle Aspiration Cytology)
- Standard first-line investigation
- Diagnostic or strongly suggestive in most cases
- Milan reporting system now used for salivary gland FNAC
Ultrasound
- First-line imaging; characterises the mass, guides FNAC
- Pleomorphic adenoma: well-defined, hypoechoic, lobulated mass
MRI (Gold Standard for Imaging)
- T1: intermediate signal; T2: high signal (due to chondromyxoid matrix)
- Lobulated heterogeneous mass, typically posterior to the retromandibular vein
- Recurrent pleomorphic adenoma: single or multiple T2 hyperintense masses within the parotidectomy bed
- Mandatory in recurrent disease to detect multifocal foci and assess residual parotid tissue
CT
- Useful to detect calcification; assesses bony involvement in deep lobe/skull base tumours
Surgical Management
Indications for Surgery
All patients should be offered surgery on three grounds:
- Definitive histology - imaging and FNAC cannot completely exclude malignancy
- Continued growth if left untreated
- Risk of malignant transformation
The Controversy: Extent of Parotidectomy
There is active debate between three approaches:
| Approach | Description | Recurrence rate |
|---|---|---|
| Enucleation | Capsule only; no cuff | ~25% - UNACCEPTABLE, never performed |
| Extracapsular Dissection (ECD) | Dissection along the tumour capsule, without formal nerve dissection | ~3.3% |
| Partial superficial parotidectomy (PSP) | Tumour + cuff of normal tissue; facial nerve identified | ~0.7% |
| Total superficial parotidectomy | Entire superficial lobe removed | <1% |
The most common practice in the UK is partial superficial parotidectomy. Key arguments for each approach are shown below (Table 9.3, Scott-Brown's):
| Arguments for ECD | Arguments for PSP/superficial parotidectomy |
|---|---|
| Recurrence rates comparable to superficial parotidectomy | Capsule is incomplete - a cuff achieves microscopic clearance |
| Less cosmetic deformity | If unexpected malignancy found, clearance may be adequate |
| Lower incidence of Frey's syndrome | - |
| A capsule-free margin adjacent to the facial nerve is impossible in most cases anyway | - |
| If revision required (e.g. malignancy), facial nerve tissue planes remain virginal | - |
Meta-analysis of 8 comparative studies (~1,492 patients) found no significant difference in recurrence rates between ECD and superficial parotidectomy, supporting the ECD approach for appropriately selected small-to-medium superficial lobe tumours.
Deep Lobe Tumours
- Generally require total conservative parotidectomy (facial nerve preserved)
- Smaller deep lobe tumours: limited superficial partial parotidectomy to gain access via inferior branches, then ECD of deep lobe tumour
- Parapharyngeal space extension: transcervical-transparotid approach (doubly modified Blair incision); transmandibulotomy if large and anterior; TORS as an emerging alternative
By Location
| Site | Operation |
|---|---|
| Superficial lobe parotid | Partial/superficial parotidectomy or ECD |
| Deep lobe parotid | Total conservative parotidectomy |
| Parapharyngeal extension | Transcervical-transparotid ± mandibulotomy |
| Submandibular gland | Excision of entire gland (extracapsular) - higher marginal mandibular nerve risk |
| Minor salivary glands (oral cavity) | Wide local excision |
Recurrence
- Overall recurrence rate: ~2-6.7% (depending on series; Dutch national database showed 6.7% over 20 years)
- Typically presents ~1 decade after original surgery
- Most recurrences are multicentric (multifocal seedling pattern)

Management of Recurrence
- MRI is mandatory - characterises recurrence(s), detects further foci, assesses residual parotid
- Repeat FNAC - do NOT rely on original histology
- Original histology reviewed by a head and neck pathologist
- The key principle: treat the first recurrence as the last good opportunity for cure with facial nerve preservation - all remaining parotid tissue should be resected with all recurrence foci
- Surgical skills needed: retrograde nerve branch dissection; facial nerve identification in mastoid; nerve repair/cabling by micro-anastomosis
- Post-operative radiotherapy considered after comprehensive resection - effective in reducing further recurrence
- Malignant change in recurrent tumours: ~3% (higher than in primary disease)
- Second recurrence after radiotherapy is challenging and may require temporal bone resection, mandibulectomy, and reconstruction
Malignant Transformation: Carcinoma Ex Pleomorphic Adenoma
- Overall risk: ~6% (Scott-Brown's); strongly time-dependent (Robbins):
- Present <5 years: 2%
- Present >15 years: 10%
- Risk factors: older age, male sex, long duration, multiple recurrences, deep lobe location
- Presents as a rapidly growing mass (within a longstanding swelling) + pain + facial palsy
- More common in women; presents a decade later than primary PA (6th decade)
- Histology: Variable proportions of pleomorphic adenoma + high-grade adenocarcinoma (salivary duct carcinoma or myoepithelial carcinoma)
- Subclassification:
- Non-invasive / intracapsular (confined within PA)
- Minimally invasive (breaching capsule)
- Widely invasive (into adjacent salivary gland and soft tissue)
- Molecular: TP53 mutations; HER2 amplification (in salivary duct carcinoma component)
- Prognosis: Among the most aggressive salivary malignancies - local and distant metastases in 70%; 5-year survival only 25-65%
- Treatment: Radical surgical excision ± adjuvant radiotherapy
Key Summary Points
| Feature | Detail |
|---|---|
| Frequency | Most common salivary gland tumour; 65% of parotid tumours |
| Age | 3rd-6th decade; peak ~45 yrs |
| Sex | F > M |
| Lobe | Superficial >80% |
| Consistency | Soft (myxoid) to hard (chondroid) |
| Hallmark histology | Ductal + myoepithelial cells in chondromyxoid stroma |
| Pathognomonic feature | Calcification / true cartilage / bone in a salivary mass |
| Capsule | Thin, incomplete in ~50%; never enucleate |
| Recurrence risk (parotidectomy) | ~2-4% |
| Recurrence risk (enucleation) | ~25% |
| Malignant transformation | ~6% overall; up to 10% if >15 years |
| Imaging | MRI: T2 hyperintense lobulated mass |
| Standard operation (UK) | Partial superficial parotidectomy |
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 & 2; Bailey & Love's Short Practice of Surgery (28th ed.); Robbins & Cotran Pathologic Basis of Disease; Cummings Otolaryngology Head & Neck Surgery; Frontiers in Surgery 2024 (ECD meta-analysis)
Warthins tumour of parotid gland
Reading File
Reading File
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.