Addison's disease
Reading File
Finding Sources
Searching PubMed
"Addison disease" AND "primary adrenal insufficiency"
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Addison's Disease (Primary Adrenocortical Insufficiency)
Addison's disease is primary adrenal insufficiency - failure of the adrenal cortex to produce adequate cortisol, aldosterone, and adrenal androgens, despite high ACTH stimulation. Clinically evident disease occurs only when ≥90% of adrenal cortical tissue is destroyed.
Etiology
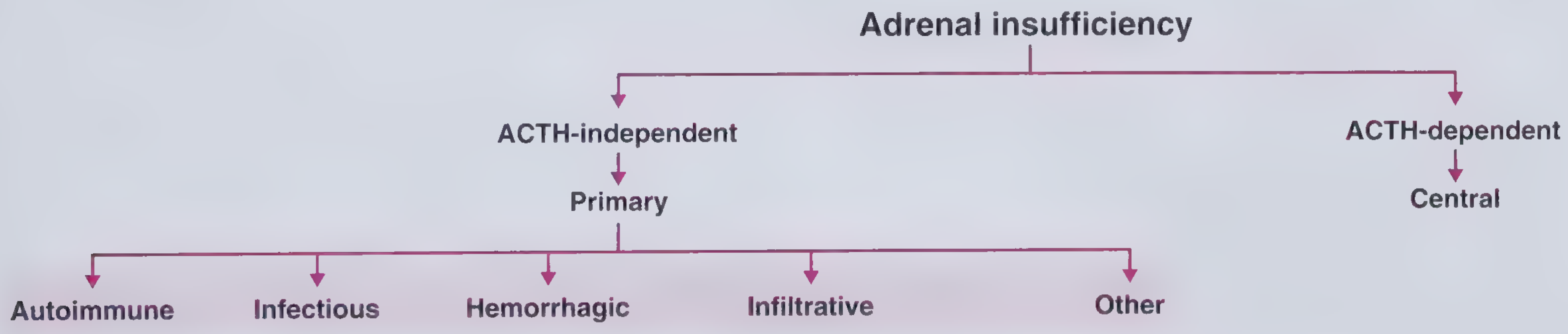
The causes fall into five major categories:
| Category | Key Examples |
|---|---|
| Autoimmune (most common in developed world, ~80%) | Isolated autoimmune adrenalitis; Polyglandular Autoimmune Syndrome type 1 (with hypoparathyroidism + candidiasis) and type 2 (with T1DM + autoimmune thyroid disease) |
| Infectious (~15% in developed world; up to 1/3 in developing countries) | TB (hematogenous spread); Histoplasmosis, Cryptococcosis, Coccidioidomycosis, Blastomycosis; CMV or MAC in AIDS |
| Hemorrhagic | Waterhouse-Friderichsen syndrome (meningococcemia); anticoagulation; antiphospholipid syndrome; adrenal vein thrombosis; critical illness; trauma |
| Infiltrative | Bilateral metastases (lung, breast, kidney, gut); lymphoma |
| Other | Adrenoleukodystrophy (X-linked, very long chain fatty acid accumulation); congenital adrenal hyperplasia; ACTH resistance |
Pathophysiology
The adrenal cortex normally produces three classes of hormones, and all are deficient in Addison's:
- Cortisol deficiency - hypoglycemia, anorexia, weight loss, nausea/vomiting, weakness, inability to mount stress response
- Aldosterone deficiency - sodium wasting, hypovolemia, hypotension, hyperkalemia, metabolic acidosis
- Adrenal androgen deficiency (DHEA, androstenedione) - decreased pubic/axillary hair and libido in women (men retain testicular androgens)
Because the adrenal cortex itself is failing, negative feedback on the anterior pituitary is lost, causing markedly elevated ACTH. The ACTH precursor (POMC) contains the alpha-MSH fragment, which stimulates melanocytes - this produces the characteristic hyperpigmentation of Addison's. The distribution is over sun-exposed areas, pressure points (elbows, knees), nail beds, nipples, areolae, and on new scars. Hyperpigmentation is a hallmark that distinguishes primary from secondary/central adrenal insufficiency.
Clinical Features
Chronic (insidious onset):
- Fatigue and weakness
- Weight loss, anorexia, nausea, vomiting
- Postural hypotension / dizziness
- Salt craving
- Hyperpigmentation of skin and mucous membranes
- Mood changes, depression
Adrenal Crisis (Addisonian Crisis - acute life-threatening):
- Profound hypotension / circulatory collapse
- Severe vomiting and diarrhoea
- Abdominal pain
- Confusion, coma
- Precipitated by infection, surgery, trauma, or any physical stress in a patient with unrecognized or undertreated Addison's
Laboratory findings:
- Hyponatremia
- Hyperkalemia
- Hypoglycemia
- Elevated plasma ACTH (>2x upper limit)
- Low/absent cortisol
- Metabolic acidosis
- Elevated plasma renin, low aldosterone
Diagnosis
Gold standard: Short Synacthen (ACTH stimulation) test
- Administer 250 mcg synthetic ACTH (tetracosactrin) IV/IM
- Measure serum cortisol at 0 and 30-60 minutes
- Normal response: peak cortisol >500 nmol/L (>18 mcg/dL) - failure to rise confirms adrenal insufficiency
Key discriminating tests (primary vs secondary):
- Plasma ACTH: elevated in primary (Addison's), low/normal in secondary
- Serum aldosterone: low + plasma renin high in primary; normal in secondary (RAAS not affected in secondary)
- Hyperkalemia: present in primary, absent in secondary
To identify the cause:
- Anti-21-hydroxylase antibodies - positive in ~80-90% of autoimmune cases
- If antibody-negative male: plasma very long-chain fatty acids (screen for adrenoleukodystrophy)
- CT abdomen: small adrenal glands in autoimmune; large/calcified in TB; bilateral hemorrhage/metastases on imaging
Treatment
Adrenal Crisis (emergency):
- IV access immediately - draw blood for cortisol before starting treatment
- Hydrocortisone 100 mg IV bolus (has both glucocorticoid and mineralocorticoid activity)
- IV normal saline (0.9%) 1 litre rapidly for volume expansion
- IV dextrose for hypoglycemia
- Treat the precipitating cause
Chronic replacement therapy:
- Glucocorticoid: Hydrocortisone 10-12 mg/m²/day in divided doses, mimicking the diurnal cortisol profile (larger morning dose, smaller afternoon dose). Alternatively, prednisone 4-7 mg/day (longer half-life, helpful for evening fatigue).
- Mineralocorticoid: Fludrocortisone (9-α-fluorohydrocortisone) 50-300 mcg/day orally. Dose titrated against blood pressure, serum Na/K, and plasma renin activity. Patients should be encouraged to maintain adequate salt intake.
- Sick-day rules: Patients must double or triple their hydrocortisone dose during illness, surgery, or physical stress ("sick day rules"). They should carry a steroid emergency card and injectable hydrocortisone kit.
- DHEA replacement: Evidence is insufficient to support routine use, though some patients with low DHEA report improved wellbeing.
Monitoring:
- Aim for normal plasma renin (for fludrocortisone dose)
- Avoid over-replacement (Cushingoid effects, osteoporosis, metabolic syndrome)
- Screen autoimmune Addison's patients for associated autoimmune conditions (thyroid, T1DM, B12 deficiency)
Summary Table (Addison's vs Cushing's vs Conn's)
| Feature | Addison's | Cushing's (Primary) | Conn's |
|---|---|---|---|
| Cortisol | Low | High | Normal |
| ACTH | High | Low | Normal |
| Aldosterone | Low | Normal | High |
| Renin | High | Normal | Low |
| BP | Low | High | High |
| K⁺ | High | Normal/low | Low |
| Na⁺ | Low | Normal/high | Normal/high |
| Skin | Hyperpigmentation | Striae, bruising | Normal |
Recent Evidence
Two recent systematic reviews are relevant:
- A 2025 meta-analysis (PMID 40966723) confirmed increased mortality in primary adrenal insufficiency, highlighting that despite hormone replacement, life expectancy remains reduced - particularly from cardiovascular and infectious causes.
- A 2024 meta-analysis (PMID 39277840) found increased adverse pregnancy outcomes in women with primary adrenal insufficiency, reinforcing the need for careful management during pregnancy and delivery.
Sources: Costanzo Physiology 7th Ed., Goldman-Cecil Medicine, Frameworks for Internal Medicine - all via the Medical Textbook Library
This is a shared conversation. Sign in to Orris to start your own chat.