Hydatid disease of lung definition etiology pathogenesis clinical features and diagnostic and treatment with drug dosage from fishman and Murray only
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed from both Fishman's and Murray & Nadel's. Let me compile the comprehensive answer.
Hydatid Disease of the Lung
Sources: Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (Chapter 136) and Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set (Chapter 58)
Definition
Hydatid disease (cystic echinococcosis, CE) is a zoonotic parasitic infection caused by the larval (metacestode) stage of the tapeworm Echinococcus granulosus, resulting in cyst formation in various organs - most commonly the liver and lungs. It is also called cystic echinococcosis or hydatidosis.
- Fishman's Pulmonary Diseases and Disorders, Ch. 136
Etiology
Causative organism: Echinococcus granulosus (the dog tapeworm) is responsible for the vast majority of pulmonary disease. Four species can infect humans: E. granulosus, E. multilocularis, E. vogeli, and E. oligarthus. E. granulosus has recently been recognized as a complex of 10 distinct genotypes.
Geographic distribution: Worldwide with endemic foci in:
- South America, Australia, eastern Europe
- North Africa, the Middle East, central Asia
- Western China
- Mediterranean basin (Italy, Spain, Albania, former Yugoslavia)
- Central America, sub-Saharan Africa, Russia, China, northern Japan
Life cycle:
- The definitive hosts (domestic dogs, foxes, wolves, and other canids) ingest the hydatid cyst form from infected viscera of intermediate hosts (sheep, pigs, cattle, goats)
- The cyst matures into the adult tapeworm in the canine intestine and sheds embryonated eggs in feces
- Humans are accidental intermediate hosts - infected by ingestion of eggs in contaminated food/water, or by close contact with dogs
- Released embryo oncospheres penetrate the intestinal wall, enter the bloodstream, and travel to the liver or other organs where they mature into metacestode cysts
- The lungs are the second most common site (20%) after the liver (80%)
- Fishman's, Ch. 136; Murray & Nadel's, Ch. 58
Pathogenesis
Cyst structure - three layers (Fig. 136-5):
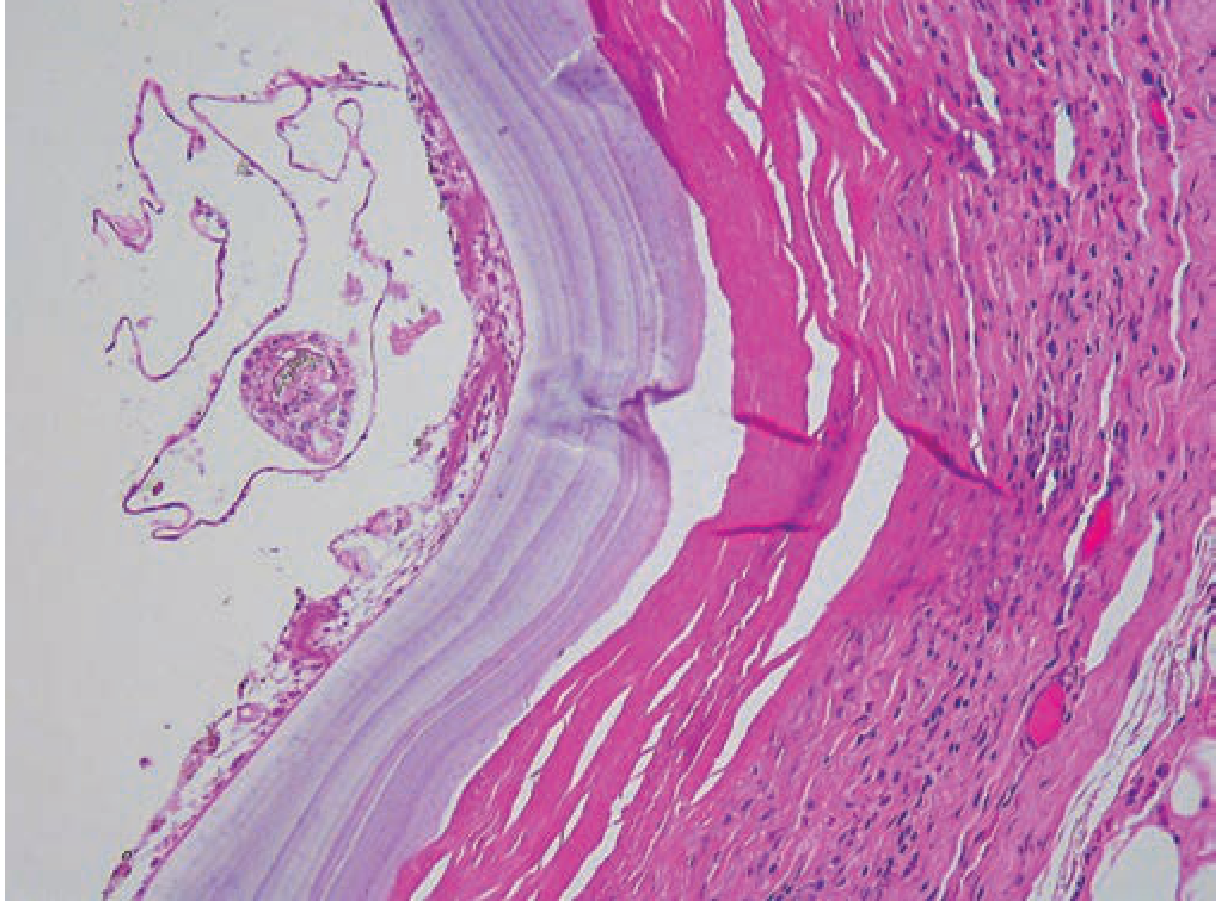
Figure 136-5 (Fishman's): Lung biopsy of hydatid cyst from E. granulosus demonstrating outer compressed host tissue, middle laminated layer, and a protoscolex arising from the inner germinal layer (H&E stain, 100x)
| Layer | Name | Composition |
|---|---|---|
| Outer | Pericyst | Host-derived compressed lung + granulomatous inflammation → fibrosis |
| Middle | Laminated layer | Acellular, parasite-derived |
| Inner | Endocyst / Germinal layer | Produces protoscolices, daughter cysts, and hydatid sand |
Growth and consequences:
-
Cysts grow slowly over years to decades, causing symptoms by mass effect
-
Eventually a cyst may degenerate into a calcified mass
-
A viable cyst may rupture:
- Into bronchial tree: expectoration of cyst material; can become secondarily infected (lung abscess)
- Into pleural space: pneumothorax, effusion, secondary seeding of daughter cysts, or empyema
- Rupture (spontaneous or iatrogenic): the cyst fluid is highly immunogenic, triggering acute hypersensitivity or anaphylactic reactions
-
In children: lung disease is more frequently detected than in adults because the lungs accommodate faster cyst growth due to greater lung elasticity and weaker immune responses
-
Fishman's, Ch. 136; Murray & Nadel's, Ch. 58
Clinical Features
Asymptomatic presentation: Pulmonary hydatid cysts are often asymptomatic and found incidentally on imaging. This is especially true in children, even with very large cysts.
Symptomatic - from cyst compression:
- Cough
- Chest pain
- Dyspnea
- Less often: hemoptysis
- Erosion into adjacent structures: bone pain, hemorrhage, or airway compression
Symptomatic - from cyst rupture (abrupt onset):
- Fever and cough (can have abrupt onset)
- Expectoration of macroscopic parasite fragments - sputum may contain cyst material ("salty water taste")
- Hemoptysis
- Urticaria, wheezing (hypersensitivity)
- Anaphylaxis (can develop, but rarely fatal)
Distribution: Cysts tend to be:
- Unilateral in 50-80% of cases
- Solitary in 60%
- Predilection for the lower lobes
- Up to 35% of individuals have concomitant hepatic involvement
Laboratory findings: Generally non-specific; peripheral eosinophilia is seen in less than 25% of cases.
- Fishman's, Ch. 136; Murray & Nadel's, Ch. 58
Diagnosis
Imaging
Chest radiograph:
- Uncomplicated (unruptured) cysts: well-defined, round or oval homogeneous masses, 1-20 cm in diameter, smooth borders, normal adjacent lung tissue
- If ruptured into a large airway: air-fluid level due to partial discharge of cyst contents
- "Water lily" sign (pathognomonic): Seen when a cyst fully or partially ruptures - air enters the cyst, the endocyst detaches from the pericyst and collapses to float on the remaining fluid - the endocyst appears like a water lily floating on a pond. This sign is rare but pathognomonic of a collapsed hydatid cyst.
- "Meniscus" sign: Crescent of air at the top of the cyst (air between pericyst and endocyst before the endocyst fully detaches)
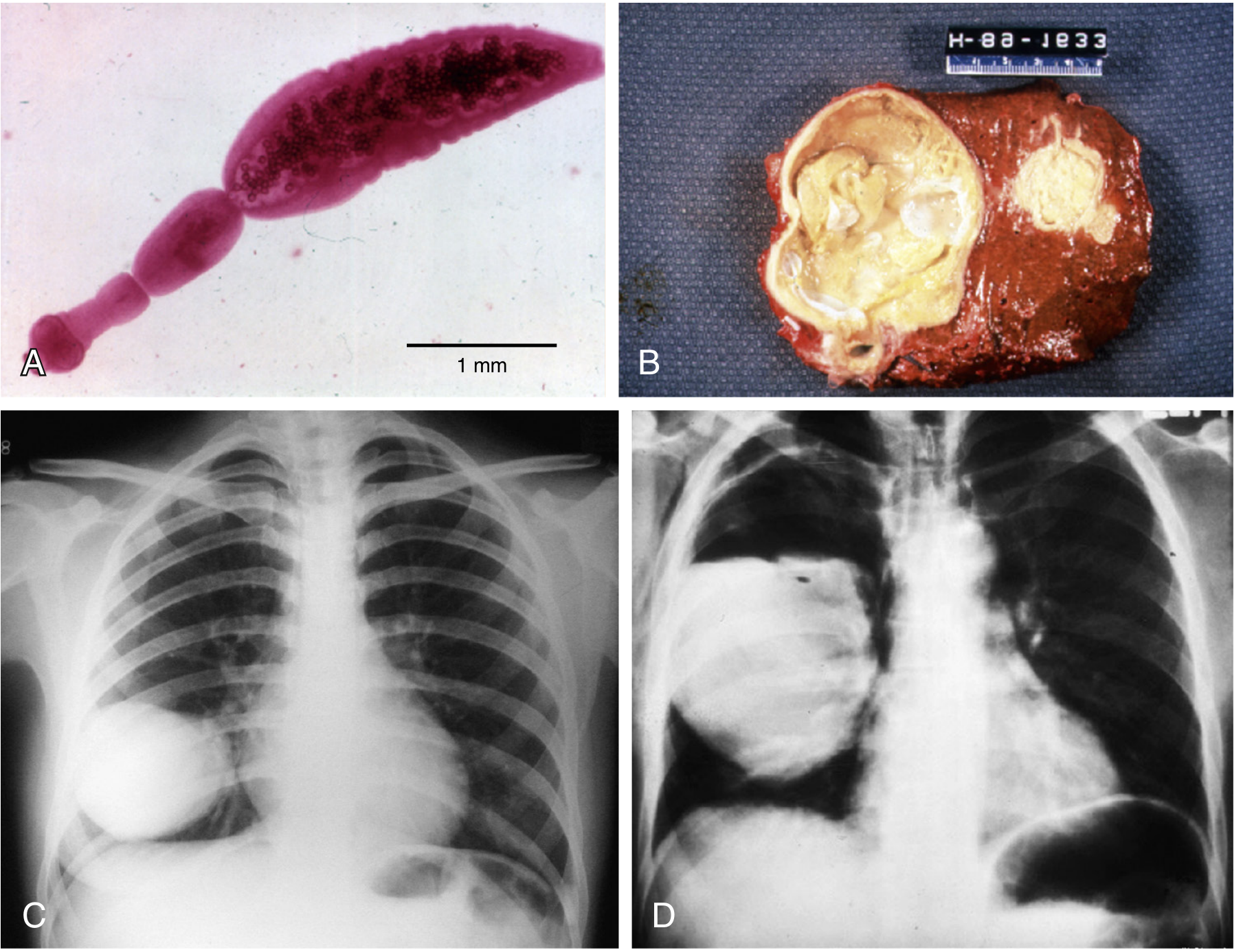
Figure 58.6 (Murray & Nadel's): (A) Adult E. granulosus; (B) Hepatic cyst; (C) Pulmonary echinococcal cyst on CXR; (D) Ruptured cyst with "water lily" sign
CT scan:
- More useful in complicated cysts
- Defines secondary infection (contrast enhancement around cyst wall)
- Shows communication with bronchial tree
- Reveals presence of daughter cysts within a larger cyst (helps distinguish from other pulmonary cysts)
- CT scan is the imaging of choice for detailed characterization
Ultrasound: Rarely used for pulmonary disease; reserved for pleural disease or cysts adjacent to the thoracic wall.
Serology
- ELISA, indirect hemagglutination, or latex agglutination can be adjunctive
- Sensitivity in pulmonary echinococcosis: only 50-60% (much lower than hepatic disease where sensitivity is 85-98%)
- Serology is therefore confirmatory rather than diagnostic in pulmonary disease
- Positive tests must be confirmed with Western blot for purified antigens (specificity limited by cross-reactivity with other helminth diseases, malignancies, and autoimmune disease)
- Cyst complications or multiorgan involvement are associated with higher seropositivity
Microscopy
- Cyst rupture: examine sputum or pleural fluid for protoscolices (rigid "mouthparts"/scolices) - diagnostic
- Aspirated cyst fluid or surgical histopathology: also diagnostic
- Direct microscopy demonstrating protoscolices or other parasite features is confirmatory
WHO expert consensus guidelines (last updated 2009) summarize key diagnostic and management recommendations.
- Fishman's, Ch. 136; Murray & Nadel's, Ch. 58
Treatment
1. Surgery (Mainstay of Treatment)
Surgery is the principal treatment for patients who can tolerate the procedure and remains the mainstay of therapy for pulmonary hydatid disease.
Goals:
- Remove as much of the cyst as possible while avoiding intraoperative spillage and dissemination
- Confirm the diagnosis
- Treat local complications
Surgical approaches (lung-parenchyma preserving, favored):
- Cyst enucleation
- Cystotomy (Fig. 136-7)
- Removal after aspiration
Recurrence rate with conservative surgery: Less than 2%.
More extensive resection (lobectomy etc.) is reserved for:
- Giant cysts
- Cysts complicated by secondary bacterial abscesses
Intraoperative precautions:
- Hypertonic saline-soaked surgical drapes to protect the operative field (scolicidal agent)
- Intraoperative instillation of hypertonic saline or 1% formaldehyde into the cyst lumen for 15 minutes or more before further manipulation (to minimize consequences of spillage)
- Cavity marsupialization or surgical drain placement after removal
Perioperative medications:
- Preoperative albendazole: reduces consequences of dissemination if intraoperative rupture occurs
- Praziquantel: added particularly if cyst has ruptured (scolicidal effect)
PAIR procedure (Percutaneous Aspiration, Injection, Re-aspiration): Not recommended for pulmonary cysts due to higher complication rates (used for hepatic cysts only).
2. Medical (Chemotherapy) - Benzimidazoles
Medical therapy is reserved for:
- Small, uncomplicated cysts
- When surgery is not feasible
- Perioperative use (pre- and post-operative)
Drug of choice: Albendazole (preferred over mebendazole due to improved bioavailability)
| Drug | Dose | Duration | Notes |
|---|---|---|---|
| Albendazole | 400 mg twice daily | 3 to 6 months | For small uncomplicated cysts; limited cure in pulmonary disease |
| Praziquantel | Added to albendazole | - | Especially if cyst ruptured; scolicidal effect; combination may have greater efficacy than either alone |
| Mebendazole | Previously used | - | Now superseded by albendazole |
Key side effects of albendazole:
- Hepatotoxicity
- Leukopenia
- Hair loss (alopecia)
- GI distress
Important notes:
- Albendazole is curative in only a minority of pulmonary cases when used alone
- Combination of albendazole + praziquantel shows promise of improved efficacy (mainly data in hepatic disease; limited pulmonary data)
- Serial serologic assays have been found to be without value for monitoring treatment response - use clinical findings and imaging instead
E. multilocularis (Alveolar Echinococcosis) - Special Note
(Murray & Nadel's, Ch. 58)
- Rare but potentially fatal
- Liver is the initial target; spreads to lung by metastatic dissemination or direct extension through the diaphragm
- The only cure is radical resection followed by long-term albendazole
- If not amenable to surgery: life-long albendazole may be beneficial
Summary Table
| Feature | Fishman's (Ch. 136) | Murray & Nadel's (Ch. 58) |
|---|---|---|
| Commonest species | E. granulosus | E. granulosus |
| Lung involvement | 20% | 20-40% |
| Cyst - unilateral | 50-80% | - |
| Cyst - solitary | 60% | Solitary, one organ in most |
| Eosinophilia | <25% | Not emphasized |
| CXR size | 1-20 cm | 1-20 cm |
| Serology sensitivity (lung) | 50-60% | ~50% |
| Albendazole dose | 400 mg BD x 3-6 months | Not explicitly dosed; prolonged course |
| Surgery recurrence | <2% | Low with proper technique |
| PAIR for lung | Not recommended | Not mentioned for lung |
References:
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set, Chapter 136 (Pulmonary Echinococcosis/Hydatid Disease), pp. 2424-2426
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set, Chapter 58 (Cestodes - Echinococcosis), pp. 1349-1351
This is a shared conversation. Sign in to Orris to start your own chat.