
c92c777a-1d26-4c3c-9133-12aac36913ee.jpg
A 55 year male , came with complains of fever since 5-6 days Shortness of breath and cough He came from amarnath yatra and symptoms developed after that What could be the diagnosis
analyse_media
Reading File
Searching the Web
miliary tuberculosis Amarnath yatra pilgrimage high altitude fever cough diagnosis
Finding Sources
Finding Sources
Searching PubMed
"miliary tuberculosis" CT diagnosis immunocompetent
Reading File
Finding Sources
Reading File
Reading File
Loading Image
This is a textbook match. Here is the complete clinical analysis:
Diagnosis: Miliary Tuberculosis (Disseminated TB)
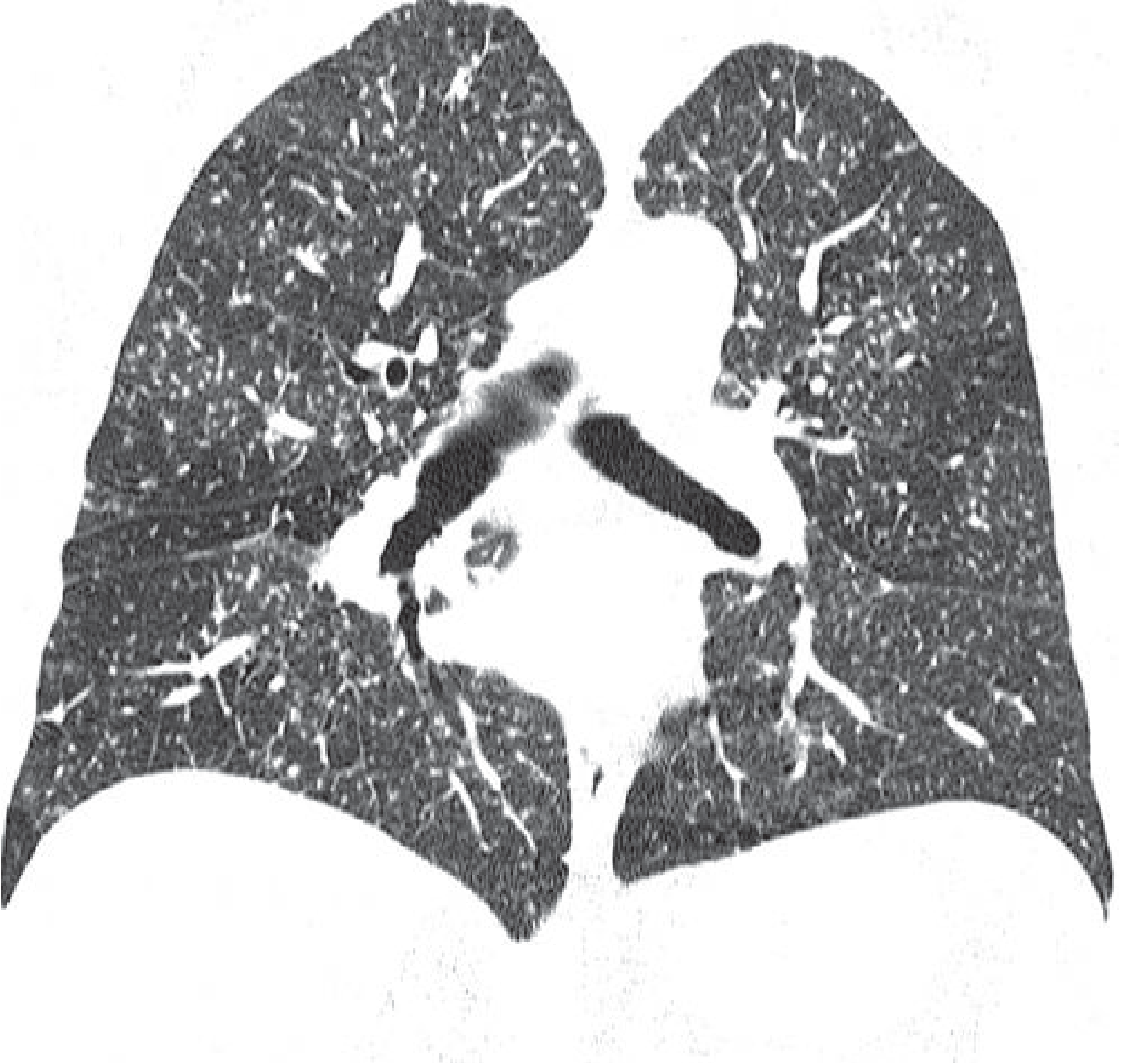
CT Chest Findings (Patient's Scan)
The CT shows the classic miliary pattern - countless tiny (1-3 mm), uniformly distributed micronodules scattered diffusely and symmetrically throughout both lungs from apex to base, with a random distribution relative to the secondary pulmonary lobule (not centrilobular, not perilymphatic). Mild background ground-glass haziness is also present. No cavitation, no pleural effusion, no tree-in-bud pattern.
This is virtually identical to the textbook appearance below:
Why the Amarnath Yatra Connection Matters
Amarnath Yatra is a high-altitude pilgrimage (cave at >13,000 ft / ~4,000 m). Pilgrims congregate in large numbers in crowded conditions - tents, base camps, shared transport - creating an ideal environment for airborne TB transmission. The patient likely:
- Was exposed to M. tuberculosis during the yatra in a crowded high-altitude setting
- Had a primary or reactivation event followed by hematogenous dissemination producing the miliary pattern
- Symptoms developed over 5-6 days post-exposure/reactivation, consistent with acute miliary TB
High-altitude conditions can also suppress immune responses transiently, lowering the threshold for reactivation of latent TB.
Clinical Picture - Why Miliary TB Fits
| Feature | This Patient |
|---|---|
| Fever (5-6 days) | Classic presenting symptom |
| Shortness of breath | Bilateral pulmonary involvement |
| Cough | Pulmonary miliary disease |
| Age 55M | Higher risk of reactivation |
| Congregation exposure (pilgrimage) | TB transmission environment |
| CT: diffuse bilateral micronodules, random pattern | Pathognomonic miliary pattern |
Differential Diagnoses to Rule Out
- Disseminated fungal infection (Histoplasmosis, Cryptococcosis) - less common in India; no endemic exposure history
- Miliary metastases - from thyroid, lung, renal, breast primary; no known malignancy - needs exclusion
- Sarcoidosis - typically perilymphatic distribution, not purely random; usually bilateral hilar adenopathy prominent
- HAPE (High Altitude Pulmonary Edema) - can occur with Amarnath Yatra but typically shows bilateral ground-glass/consolidation, NOT miliary nodules
Recommended Workup
- Sputum for AFB smear x3 (sensitivity ~30-40% in miliary TB - often negative)
- Sputum CBNAAT/GeneXpert (faster, more sensitive)
- Mycobacterial blood cultures (positive in ~40-50% of miliary TB)
- TST / IGRA - note: may be falsely negative in miliary TB due to immune dysregulation; a negative IGRA does not exclude diagnosis per Harrison's Principles
- Liver biopsy / bone marrow biopsy - liver biopsy has the highest diagnostic yield for miliary TB (granulomas on AFB smear/culture/PCR)
- Bronchoscopy with BAL - diagnostic yield ~70% in miliary TB where sputum is negative (Fishman's Pulmonary Diseases)
- LFTs, CBC, serum ADA
- HIV testing (immune status)
- Fundoscopy - look for choroidal tubercles (pathognomonic when present)
Treatment
Standard 4-drug anti-TB regimen (2HRZE/4HR):
- Intensive phase (2 months): Isoniazid + Rifampicin + Pyrazinamide + Ethambutol
- Continuation phase (4 months): Isoniazid + Rifampicin
- Total duration: 6-9 months for miliary TB (some guidelines recommend 9-12 months)
- Steroids (Prednisolone) may be added if there is meningeal involvement or severe hypoxia
Key point: Miliary TB can be rapidly fatal if untreated. If clinical suspicion is high (as it is here, given the CT and history), empirical anti-TB treatment should not be delayed while awaiting culture confirmation, especially if the patient is deteriorating. Per Harrison's: "If fever does not respond after 6 weeks of empirical antituberculous treatment, another diagnosis should be considered."
- Grainger & Allison's Diagnostic Radiology, Fig. 5.29
- Harrison's Principles of Internal Medicine 22E - Fever of Unknown Origin & Miliary TB
- Fishman's Pulmonary Diseases - Mycobacterial Infections, bronchoscopy in miliary TB
This is a shared conversation. Sign in to Orris to start your own chat.