Heart' failure management
Reading File
Finding Sources
Searching PubMed
"heart failure" AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Here is the full evidence-based overview:
Heart Failure Management
Staging Framework (2022 ACC/AHA)
The ACC/AHA uses a 4-stage classification that drives management strategy:
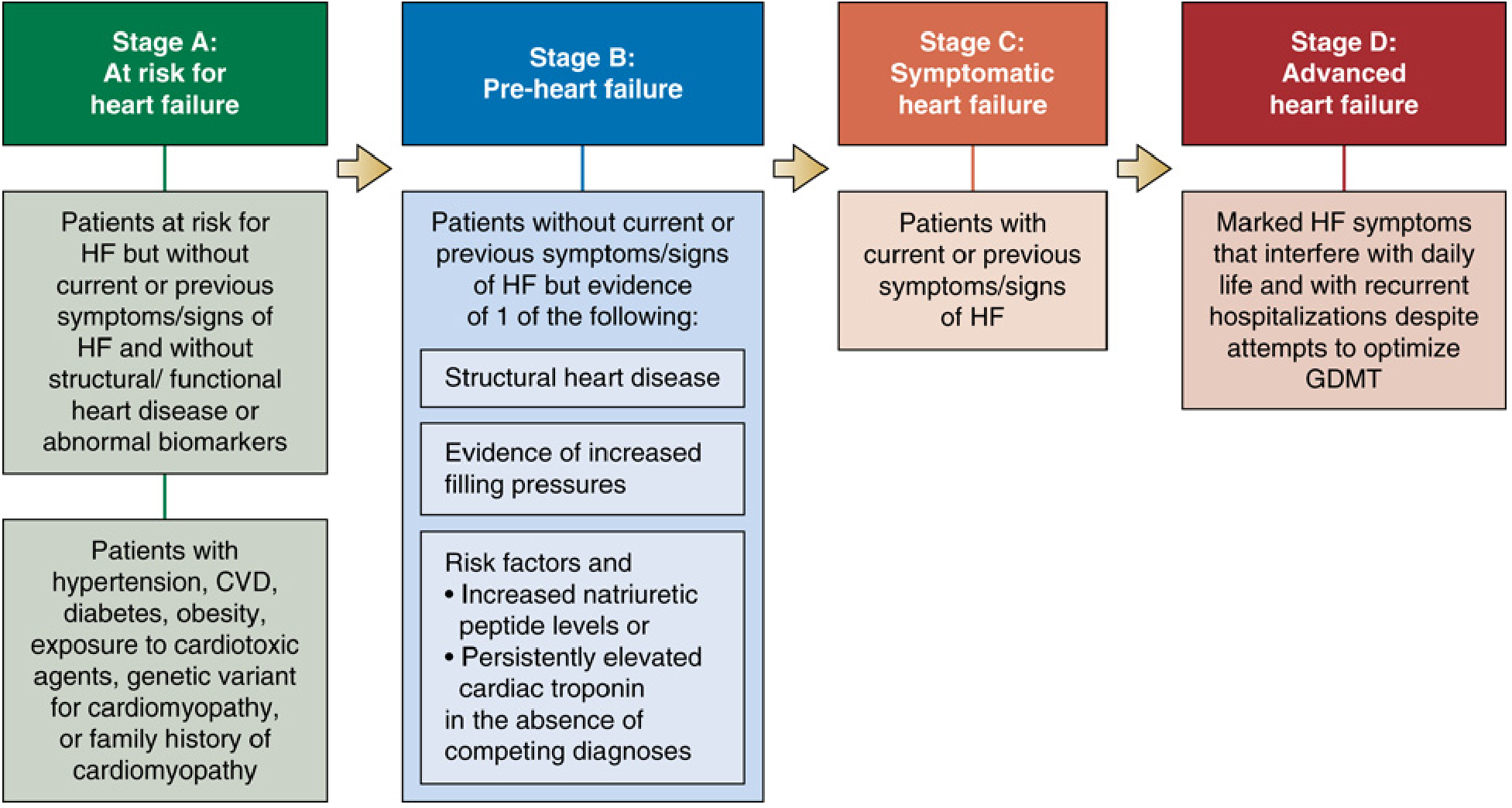
- Stage A - At risk (hypertension, diabetes, obesity, family history of cardiomyopathy, cardiotoxin exposure) but no structural disease or symptoms
- Stage B - Pre-HF: structural heart disease, elevated filling pressures, or elevated natriuretic peptides - but no symptoms yet
- Stage C - Symptomatic HF (current or prior symptoms with structural heart disease)
- Stage D - Advanced HF: marked symptoms interfering with daily life, recurrent hospitalizations despite optimized GDMT
Therapies of Proven Benefit (Goldman-Cecil Medicine, Table 46-1)
| Category | Therapies |
|---|---|
| Neurohormonal blockers | ACE inhibitors, ARBs, Beta-blockers, MRAs, Sacubitril-valsartan |
| Novel | SGLT2 inhibitors, Ivabradine, Vericiguat |
| Vasodilators | Hydralazine + isosorbide dinitrate |
| Symptom control | Diuretics, Digoxin |
| Device therapy | CRT, ICD, Ventricular assist device |
| Definitive | Heart transplantation |
| Lifestyle | Exercise training |
Chronic HFrEF (EF < 40%) - Quadruple GDMT
Per Miller's Anesthesia (citing 2022 ACC/AHA) and Katzung, patients with LVEF < 40% in Stage C or D should receive quadruple guideline-directed medical therapy (GDMT):
1. Diuretics
- Loop diuretics (furosemide, torsemide, bumetanide) are the cornerstone for congestive symptoms
- Thiazides for mild failure; loop agents required for moderate-severe disease
- Sodium removal by dietary salt restriction + diuretics remains the foundational symptomatic approach
- Torsemide and bumetanide have superior oral bioavailability compared to furosemide
- Add spironolactone/eplerenone to counter potassium loss and gain mortality benefit
- SGLT2 inhibitors also exert natriuresis and partly work via this mechanism
2. ACE Inhibitors / ARBs
- First drug for patients with LV dysfunction but no edema
- Multiple large RCTs confirm ACEIs are superior to placebo and to vasodilators alone
- ARBs (losartan, valsartan, candesartan) are reserved for ACEI-intolerant patients (usually cough)
- Benefits include reduced mortality and HF hospitalization
- Monitor potassium, renal function, and blood pressure closely - especially in older patients
3. ARNI: Sacubitril-Valsartan (Entresto)
- Recommended over ACEI in patients who can tolerate it (PARADIGM-HF trial)
- PARADIGM-HF (2014, n=8,442): reduced total mortality by 16%, CV death by 20%, HF hospitalization by 21% vs. enalapril
- Benefits were consistent across age groups including patients > 75 years
- Do not co-administer with an ACEI (risk of angioedema); washout period of 36 hours required when switching
4. Beta-Blockers
- Not a class effect - only carvedilol, bisoprolol, and metoprolol succinate (extended release) have RCT evidence for mortality reduction
- Nebivolol and bucindolol also shown to reduce mortality but are not approved for HF in the US
- Must be started at low doses; several months may be needed before symptomatic improvement
- Mechanism: counter the adverse effects of chronically elevated catecholamines and cardiac remodeling
- Carvedilol preferred in hypertensive HFrEF patients due to its vasodilating properties
5. Mineralocorticoid Receptor Antagonists (MRA)
- Spironolactone and eplerenone reduce morbidity and mortality in moderate-severe HFrEF
- Should be considered in all patients with moderate-to-severe HF
- Careful monitoring of potassium and renal function required - especially in elderly patients
- Starting doses: spironolactone 12.5-25 mg/day; eplerenone 25 mg/day
6. SGLT2 Inhibitors (Dapagliflozin, Empagliflozin)
- Now first-line therapy for both HFrEF and HFpEF
- Reduce all-cause mortality and HF hospitalizations - benefit appears independent of glycemic control
- A 2025 meta-analysis (PMID 40884036, DAPA ACT HF-TIMI 68, Circulation) confirmed benefit of dapagliflozin even in patients hospitalized for HF, regardless of ejection fraction
- Mechanism in HF not fully elucidated but includes natriuresis, reduced preload/afterload, metabolic and direct cardiorenal effects
Additional Pharmacotherapy
Ivabradine
- I(f) channel blocker that slows heart rate without affecting contractility
- Indicated in sinus rhythm with resting HR ≥ 70 bpm, on maximally tolerated beta-blocker
- Reduces HF hospitalizations; may be useful in diastolic HF to improve filling time
Hydralazine + Isosorbide Dinitrate (BiDil)
- Fixed combination (arteriolar + venous dilation)
- Specifically recommended for Black patients with HFrEF who cannot tolerate ACEI/ARB
- Used in patients with high filling pressures (nitrates) or low output (hydralazine) predominantly
Vericiguat
- Soluble guanylate cyclase stimulator
- Approved for high-risk, worsening chronic HFrEF (recent decompensation); reduces CV death and HF hospitalization
Digoxin
- Indicated mainly when HF coexists with atrial fibrillation
- Used when diuretics and ACEIs have failed to control symptoms
- Target plasma level ≤ 1 ng/mL to minimize toxicity
- Reduces hospitalizations and progressive HF deaths but at the expense of increased sudden cardiac death; net mortality effect is neutral
Diastolic HF / HFpEF (EF ≥ 50%)
- SGLT2 inhibitors are now first-line for HFpEF (Katzung 16e)
- Control of hypertension is particularly important
- ACEIs/ARBs: may help reduce LVH and are used adjunctively
- Rate control for atrial fibrillation is critical - tachycardia severely limits diastolic filling time
- Bradycardic agents (ivabradine) may help maintain adequate filling time even in sinus rhythm
- Treat hyperlipidemia and consider revascularization if CAD is present
- Diuretics should be used with caution - these patients are preload-dependent
| Feature | HFrEF | HFpEF |
|---|---|---|
| Ejection fraction | Reduced (< 40%) | Preserved (≥ 50%) |
| Diuretics | First-line for symptoms | Use cautiously |
| SGLT2 inhibitors | Reduce mortality | First-line |
| ARNI | Reduces mortality | Reduces NT-proBNP/symptoms |
| Beta-blockers | Reduce mortality | Useful for HR/BP control |
| CCBs | No/little benefit | Useful for HR/BP (non-DHP) |
| Digoxin | May reduce symptoms | Little or no role |
(Katzung Basic & Clinical Pharmacology 16e, Table 13-4)
Acute / Decompensated Heart Failure
- IV therapy is standard
- Furosemide IV at high dose is the workhorse diuretic; adding acetazolamide to high-dose furosemide shows important additive benefit
- Dopamine or dobutamine for acute failure with severe hypotension (positive inotropes, short-acting)
- Levosimendan: approved in Europe; non-inferior to dobutamine in trials
- IV vasodilators: nitroprusside (arteriolar + venous), nitroglycerin (venous), nesiritide (BNP analog) - reduce afterload and pulmonary congestion
- Conivaptan / Tolvaptan (vasopressin antagonists): for HF with dilutional hyponatremia; do not reduce mortality but correct hyponatremia
Acute precipitants to address:
- Non-adherence to medications or diet
- Acute myocardial infarction (emergency revascularization with PCI or thrombolytics)
- Infection/fever, anemia, arrhythmias (AF)
- Uncontrolled hypertension
Device Therapy
Implantable Cardioverter-Defibrillator (ICD)
- LVEF < 40%, Stage B: post-MI > 40 days with expected survival > 1 year
- LVEF < 35%, Stage C with expected survival > 1 year
Cardiac Resynchronization Therapy (CRT)
- For patients with LVEF ≤ 35%, LBBB, QRS ≥ 150 ms, NYHA Class II-IV on optimal GDMT
- Improves symptoms, reduces hospitalization, and reduces mortality
Ventricular Assist Devices (VAD)
- Bridge to transplantation or destination therapy in Stage D
- Left ventricular assist devices (LVADs) improve survival in advanced HF
Heart Transplantation
- Definitive therapy for Stage D HF refractory to all other measures
- 1-year survival > 85%; median survival ~12-13 years
Non-Pharmacological / Lifestyle Measures
- Sodium restriction: dietary salt restriction is foundational alongside diuretics
- Exercise training: proven benefit (Goldman-Cecil, Table 46-1); improves functional capacity and quality of life
- Fluid restriction in advanced HF with hyponatremia
- Monitor daily weight: early detection of fluid retention
- Vaccinations: influenza, pneumococcal (prevent HF exacerbations)
- Avoid NSAIDs, non-DHP calcium channel blockers (in HFrEF), and thiazolidinediones
Stages A & B - Prevention Focus
- Treat hypertension aggressively
- SGLT2 inhibitors for all Type 2 diabetes patients with CVD risk
- Control hyperlipidemia (statins)
- Correct arrhythmias, especially atrial fibrillation
- ACEIs/ARBs for patients with LVEF < 40% even before symptoms develop (Stage B)
- ICD implantation for eligible Stage B post-MI patients
Sources: Goldman-Cecil Medicine (Chapter 46), Miller's Anesthesia 10e (Chapter 50), Katzung Basic & Clinical Pharmacology 16e (Chapter 13), Braunwald's Heart Disease (Chapter 50/Geriatric HF). Recent evidence: DAPA ACT HF-TIMI 68 meta-analysis (PMID 40884036, Circulation 2025) confirms SGLT2 inhibitor benefit in hospitalized HF across all EF ranges.
This is a shared conversation. Sign in to Orris to start your own chat.