Elaborate me opd management for polyarthralgia with reference to all kind of arthritis from its diagnosis to management protocol
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
polyarthralgia differential diagnosis management
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have excellent, comprehensive data from multiple authoritative textbooks. Let me compile the full OPD management guide.
OPD Management of Polyarthralgia: A Comprehensive Reference Guide
Sources: Firestein & Kelley's Textbook of Rheumatology; ROSEN's Emergency Medicine; Rheumatology 2-Volume Set (Elsevier 2022); Goldman-Cecil Medicine
1. Definition and Initial Framing
Polyarthralgia = pain in 5 or more joints (without necessarily confirmed synovial inflammation). When objective synovitis is confirmed, the term becomes polyarthritis. The OPD approach to a patient presenting with multi-joint pain is one of the most challenging tasks in clinical medicine because the differential is wide, ranges from benign to life-threatening, and requires systematic narrowing.
Key distinction at the first encounter:
- Arthralgia only (pain, no swelling/warmth) vs. True arthritis (swelling + warmth + tenderness = synovitis)
- Articular vs. Periarticular (bursitis, tendinitis, enthesitis - these mimic joint disease but do not involve the synovium)
2. OPD Diagnostic Algorithm
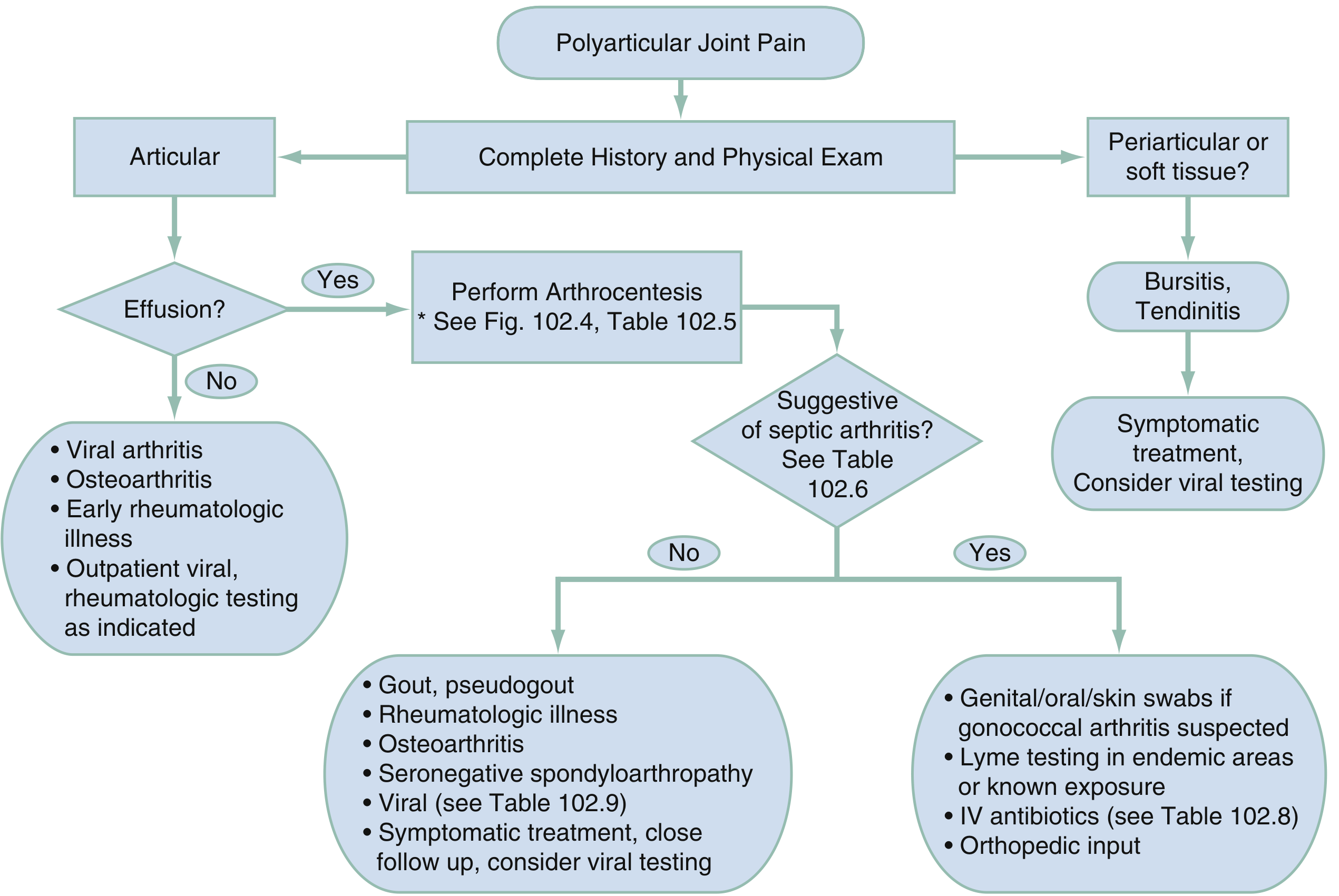
Fig. - Algorithm for Polyarticular Joint Pain (ROSEN's Emergency Medicine)
Step 1: Complete History and Physical Examination
- Articular? → proceed to effusion check → arthrocentesis if effusion present
- Periarticular/soft tissue? → Bursitis/Tendinitis → symptomatic treatment, consider viral testing
Step 2: If articular with effusion:
- Arthrocentesis → Is it suggestive of septic arthritis?
- Yes → cultures, IV antibiotics, orthopedic input
- No → workup for gout, pseudogout, rheumatologic illness, OA, seronegative spondyloarthropathy, viral causes
Step 3: If articular without effusion:
- Viral arthritis, OA, early rheumatologic illness → outpatient viral/rheumatologic testing as indicated
3. History Taking: The Seven Dimensions
A thorough history is the "sine qua non" of diagnosis in arthritis. Collect all seven dimensions:
| Dimension | Key Questions | Diagnostic Clue |
|---|---|---|
| Location | Which joints? Symmetric vs. asymmetric? | Symmetric MCP/PIP → RA; Asymmetric lower-limb → SpA; DIP dominant → OA or PsA |
| Quality | Aching? Burning? Stabbing? | Crystal arthritis = exquisite, severe pain |
| Duration/Timing | Acute (<6 weeks) or chronic (>6 weeks)? | Viral = acute; RA/SpA = chronic |
| Morning stiffness | Duration on waking | >1 hour → inflammatory (RA); <30 min → OA ("gel phenomenon") |
| Modifying factors | Better with movement or rest? | Movement improves inflammatory arthritis; worsens OA |
| Associated features | Rash, fever, GI symptoms, eye symptoms, oral ulcers, genital discharge, back pain | See red flags below |
| Context/Risk factors | Sexual history, travel, tick exposure, family history | Gonococcal, Lyme, SpA |
Systemic review red flags (ask specifically):
- Skin rash (psoriasis → PsA; butterfly rash → SLE; keratoderma blennorrhagica → reactive arthritis)
- Mucosal ulcers (SLE, Behçet's, reactive arthritis)
- Uveitis/iritis (SpA, JIA)
- Urogenital symptoms (reactive arthritis)
- GI symptoms / diarrhea (enteropathic arthritis, reactive arthritis)
- Fever + weight loss (septic arthritis, adult-onset Still's, malignancy-associated)
- Raynaud's, dry eyes/mouth (connective tissue disease, Sjögren's)
4. Physical Examination
Joint examination principles:
- Synovial swelling = soft, doughy, fluctuant around the joint line (finger sinks in)
- Bony swelling = hard, fixed (e.g., Heberden's nodes in OA)
- Redness/warmth = highly active inflammation (septic arthritis, gout, reactive arthritis)
- Use the "squeeze test" (lateral compression of MCP/MTP joints) as a screening sign for inflammatory arthritis
Standard joint counts:
- RA follow-up: DAS28 (28 joints: MCP 1-5, PIP 1-5 bilateral; wrists, elbows, shoulders, knees)
- Full initial exam: 66/68-joint count at first presentation
Pattern Recognition Table (Firestein & Kelley's Rheumatology)
| Feature | Rheumatoid Arthritis | Osteoarthritis | Psoriatic Arthritis | Gout / Pseudogout |
|---|---|---|---|---|
| Large joints | Knees, ankles, wrists - symmetric | Hips, knees, ankles | Knees, ankles, wrists - asymmetric | Knees, ankles; wrists in pseudogout |
| Small joints | MCP and PIP (symmetric) | DIP, PIP, 1st CMC; 1st MTP | DIP prominent + nail changes (asymmetric) | Podagra (1st MTP in gout); MCP in pseudogout |
| Spine | Cervical spine only | Cervical + lumbar | Lumbar + SI joints | Not involved |
| Morning stiffness | >1 hour | <30 minutes | Variable | Not typical between attacks |
| Onset speed | Weeks to months | Slow, over years | Variable | Acute, sudden |
| Systemic symptoms | Fatigue, low-grade fever, nodules | None | Skin/nail psoriasis | None (between attacks) |
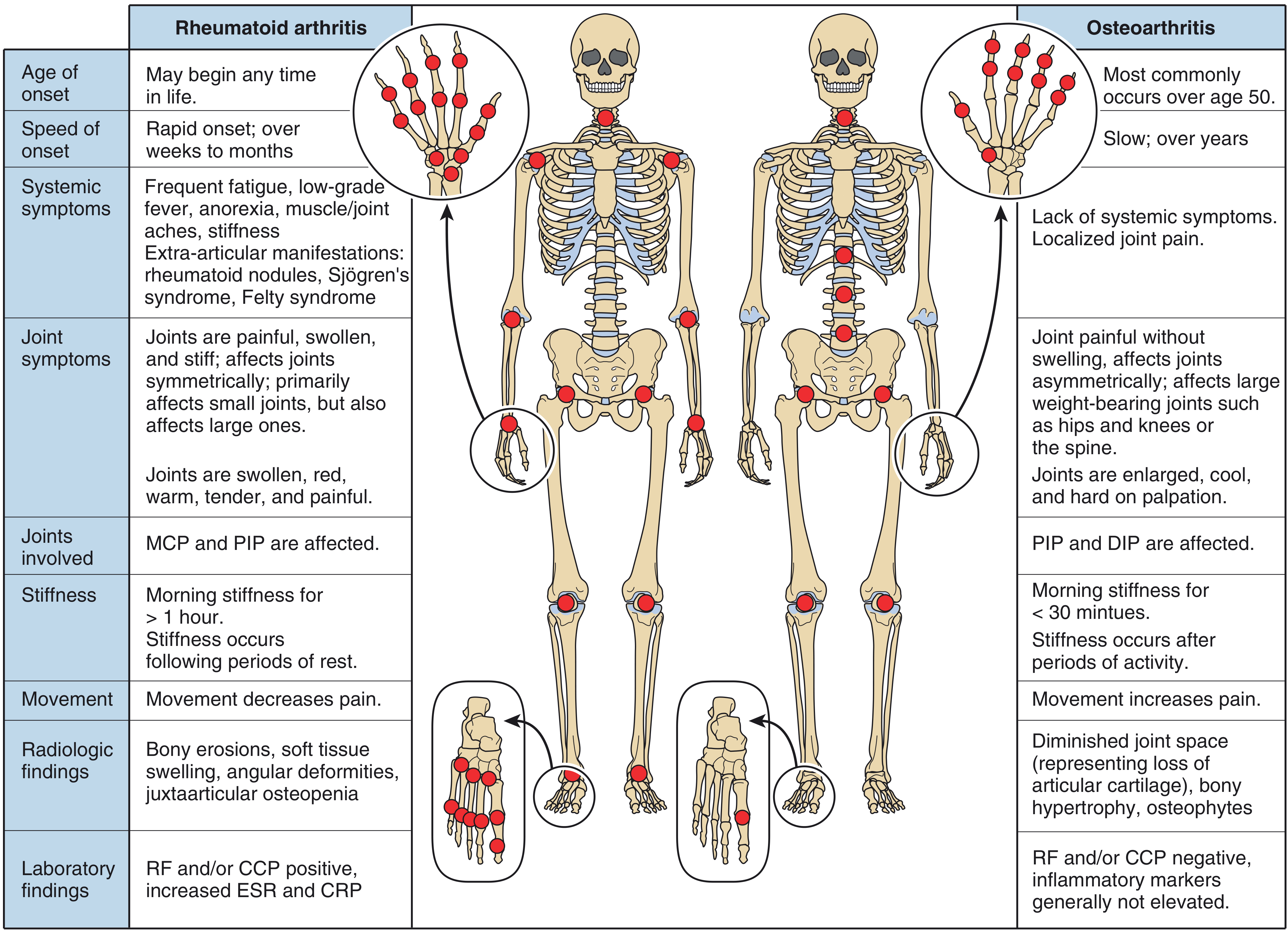
Fig. - RA vs OA: key distinguishing features (Firestein & Kelley's Textbook of Rheumatology)
Extra-articular findings on general examination:
- Skin: psoriasis, tophi (gout), nodules (RA), malar rash (SLE), keratoderma blennorrhagica (reactive)
- Eyes: uveitis/iritis (SpA, JIA), scleritis (RA)
- Lymphadenopathy: viral arthritis, lymphoma, Still's
- Salivary glands: Sjögren's
- Entheses: SpA (Achilles, plantar fascia, iliac crest)
- Dactylitis: "sausage digit" in PsA, reactive arthritis, rarely sarcoidosis
- Spine: restricted lumbar flexion, Schober's test (AS/axial SpA)
5. Investigations in OPD
Tier 1 - Order in ALL patients with polyarthralgia
| Test | Rationale |
|---|---|
| CBC with differential | Leukocytosis (infection/Still's); anemia of chronic disease (RA, SLE) |
| ESR + CRP | Elevated in inflammatory disease; normal argues against infectious cause but does not exclude rheumatologic diagnosis |
| RFT (Creatinine, urea) | Gout associated with renal insufficiency; relevant before NSAIDs/colchicine |
| Urine routine/microscopy | Proteinuria + red cell casts → SLE, vasculitis, SBE |
| Blood glucose | Metabolic syndrome links with gout |
| Uric acid | Raised in gout (but can be normal during an acute attack) |
| X-ray of affected joints | Baseline; erosions (RA), osteophytes/joint space narrowing (OA), chondrocalcinosis (pseudogout) |
Tier 2 - Targeted by clinical picture
| Test | When to order | Disease |
|---|---|---|
| RF (Rheumatoid Factor) | Suspected inflammatory polyarthritis | RA (60-70% sensitive, NOT specific - also positive in SLE, Sjögren's, SBE, Hep B/C, parvovirus) |
| Anti-CCP (ACPA) | Suspected RA | RA - equal sensitivity to RF but much MORE SPECIFIC; positive years before clinical onset; predicts erosive disease |
| ANA | Suspected SLE, MCTD, Sjögren's, scleroderma | Screen; if positive → anti-dsDNA, anti-Sm, anti-Ro/La, anti-Scl70, anti-centromere |
| HLA-B27 | Suspected axial SpA, reactive arthritis, PsA with spinal involvement | >90% in AS; 50-80% in other SpAs; cost-effective once-in-lifetime test |
| ASOT (Anti-streptolysin O) | Suspected rheumatic fever | Streptococcal-triggered arthritis |
| Blood cultures | Fever + acute joint disease | Septic arthritis, SBE |
| Hepatitis B/C serology | Suspected viral arthritis | HBV = migratory, symmetric; HCV = RA-like + positive RF |
| HIV | Risk factors present | HIV arthropathy (lower limb, monoarticular) |
| Parvovirus B19 IgM/IgG | Acute symmetric small joint arthritis in adults | RA-mimic, self-limited |
| Lyme serology (IgM/IgG) | Endemic area, tick exposure, large joint (knee) effusion | Lyme arthritis |
| Ferritin | High fever + rash + arthritis in young adult | Adult-onset Still's disease (ferritin >10,000 in AOSD) |
| ACE level | Periarthritis + hilar adenopathy | Sarcoidosis |
| Thyroid function (TSH) | Suspected pseudogout, unexplained arthralgia | Hypothyroidism → CPPD deposition |
| Urine culture | Elderly + gram-negative septic arthritis | Urinary tract source |
Tier 3 - Imaging beyond plain X-ray
| Modality | Best for |
|---|---|
| Ultrasound | Detect early synovitis and effusions not visible clinically; guide arthrocentesis; "double contour sign" in gout; tophi appear as "wet clumps of sugar" |
| MRI | Confirm sacroiliitis (axial SpA before X-ray changes); spinal disease in AS; enthesitis; early erosions |
| DECT (Dual Energy CT) | Definitive urate crystal detection in gout; useful when synovial fluid unavailable |
Synovial Fluid Analysis (Arthrocentesis) - Whenever a joint effusion is present
| Fluid Class | WCC (/mm³) | Appearance | Conditions |
|---|---|---|---|
| Normal | <200 | Clear, straw | - |
| Non-inflammatory | 200-2,000 | Yellow, clear | OA, trauma |
| Inflammatory | 2,000-50,000 | Turbid, yellow | RA, crystal arthritis, reactive, viral |
| Septic | >50,000 (often >100,000) | Cloudy/purulent | Bacterial arthritis - EMERGENCY |
- Crystals: Monosodium urate (gout) = negatively birefringent, needle-shaped; CPPD (pseudogout) = positively birefringent, rhomboid
- Gram stain + culture: mandatory if infection suspected (precede antibiotics)
- Glucose: low in septic arthritis (<60% of serum glucose)
- Lactate: rising evidence; point-of-care synovial lactate >10 mmol/L supports septic arthritis
6. Differential Diagnosis and Disease-Specific OPD Management
6.1 Rheumatoid Arthritis (RA)
Diagnostic Criteria (ACR/EULAR 2010 - score ≥6/10):
- Joint involvement (score 0-5)
- Serology: RF/anti-CCP positive (score 0-3)
- Acute phase reactants: abnormal CRP/ESR (score 0-1)
- Duration ≥6 weeks (score 0-1)
OPD Management Protocol:
- NSAIDs - short-term symptom relief in early disease; use lowest effective dose
- Low-dose corticosteroids (prednisolone ≤10 mg/day) - bridge therapy while waiting for DMARD effect; taper as DMARDs take hold
- DMARDs (start within 3 months of diagnosis - treat-to-target strategy):
- Methotrexate is the anchor DMARD (7.5-25 mg/week oral or SC); supplement with folic acid 5 mg/week
- Hydroxychloroquine (200-400 mg/day) - milder disease; requires annual ophthalmology review
- Sulfasalazine (500 mg titrated to 2-3 g/day)
- Leflunomide (10-20 mg/day) - alternative to MTX
- Biologic DMARDs (if inadequate response to 2 csDMARDs):
- TNF-alpha inhibitors (etanercept, adalimumab, infliximab)
- IL-6 inhibitors (tocilizumab, sarilumab)
- T-cell co-stimulation inhibitor (abatacept)
- Rituximab (anti-CD20)
- Treat-to-target: Target = remission or low disease activity by DAS28; reassess every 1-3 months
- OPD monitoring: CBC, LFT, RFT every 3 months on MTX; screen for TB before biologics
6.2 Osteoarthritis (OA)
OPD Management (ACR/AAOS Guidelines):
Non-pharmacological (first-line, always):
- Weight loss (if BMI >25) - most effective single intervention for knee OA
- Aerobic exercise + resistance training (does not worsen cartilage)
- Physiotherapy - range of motion + muscle strengthening
- Occupational therapy - joint protection, assistive devices
- Footwear modification, knee bracing for medial compartment OA
Pharmacological:
- Topical NSAIDs (diclofenac gel) - preferred over oral in patients >65 years (less systemic toxicity)
- Oral NSAIDs (ibuprofen, naproxen, celecoxib) - short courses; use with PPI if GI risk
- Paracetamol (acetaminophen) - limited benefit; useful in mild cases
- Intra-articular corticosteroids - acute exacerbations; no more than 3-4 injections/year per joint
- Intra-articular hyaluronic acid - modest evidence; considered if corticosteroids fail
- Duloxetine - evidence for central sensitization component; FDA approved for OA pain
Surgical (OPD referral criteria):
- Failed 6 months of optimal conservative treatment
- Significant functional impairment
- Unicompartmental (partial) or total knee/hip replacement
6.3 Crystal Arthropathies
Gout
Acute attack management (OPD):
- NSAIDs (indomethacin 50 mg TID or naproxen 500 mg BD for 5-7 days) - first choice if no contraindication
- Colchicine (1.2 mg loading dose, then 0.6 mg 1 hour later; then 0.6 mg BD) - effective if started within 36-48 hours of attack
- Corticosteroids (prednisolone 30-35 mg/day for 5 days, or intra-articular injection) - when NSAIDs and colchicine are contraindicated (renal failure, elderly)
- Do NOT stop existing allopurinol during an acute attack; do NOT start new urate-lowering therapy during an attack
Chronic/Prophylactic management:
- Allopurinol - start at 50-100 mg/day; titrate to serum uric acid <6 mg/dL (target <5 mg/dL in tophaceous gout)
- Febuxostat (80-120 mg/day) - alternative xanthine oxidase inhibitor; avoid in cardiovascular disease
- Probenecid - uricosuric; only if underexcretor with normal renal function
- Colchicine 0.6 mg/day prophylaxis for 6 months when starting urate-lowering therapy
- Dietary counseling: avoid organ meats, shellfish, beer, high-fructose corn syrup; increase hydration
- Address contributing medications: thiazides, cyclosporine, low-dose aspirin (if clinically safe to switch)
Pseudogout (CPPD)
- Acute: NSAIDs, colchicine, or intra-articular/systemic corticosteroids
- Asymptomatic CPPD (radiologic chondrocalcinosis without symptoms) - treat underlying cause (hyperparathyroidism, hemochromatosis, hypomagnesemia)
- No proven agents to dissolve CPPD crystals; promising but unproven: methotrexate, IL-1 inhibitors
6.4 Seronegative Spondyloarthropathies (SpA)
This group includes: Ankylosing Spondylitis (AS) / Axial SpA, Psoriatic Arthritis (PsA), Reactive Arthritis, Enteropathic Arthritis
Shared features (PEAR mnemonic):
- Psoriform skin/nail changes or GI/urogenital trigger
- Enthesitis
- Asymmetric peripheral arthritis (lower > upper limb)
- Radiation to sacroiliac joints; HLA-B27 positive
Ankylosing Spondylitis / Axial SpA
OPD Management:
- NSAIDs continuously (not on-demand) - cornerstone; reduce inflammation + slow radiographic progression
- Physiotherapy - daily spinal exercises mandatory; prevent ankylosis
- Biologic DMARDs if NSAIDs fail (ASsess by ASDAS/BASDAI):
- TNF inhibitors (etanercept, adalimumab, certolizumab, golimumab)
- IL-17A inhibitors (secukinumab, ixekizumab) - preferred if also IBD present (caution - may worsen IBD)
- csDMARDs (sulfasalazine) have NO role in pure axial disease; useful for peripheral SpA
- Monitor: spine X-ray every 2 years; DEXA for osteoporosis
Psoriatic Arthritis (PsA)
OPD Management:
- NSAIDs - first-line for mild peripheral arthritis
- Local corticosteroid injections - adjunct (avoid systemic steroids - rebound psoriasis flare risk)
- csDMARDs (initiated early):
- Methotrexate - particularly useful when skin psoriasis also needs treatment
- Sulfasalazine, leflunomide - alternatives
- Biologic DMARDs (TNF inhibitors, IL-17 inhibitors, IL-23 inhibitors such as guselkumab for skin-predominant) if csDMARDs fail
- Nail disease: topical treatments; biologic agents treat both nail and joint
- Referral to dermatology for skin management coordination
Reactive Arthritis (Reiter's Syndrome)
- Triggered by: Chlamydia trachomatis (urogenital), Salmonella, Shigella, Campylobacter, Yersinia (enteric)
- Classic triad: arthritis + urethritis + conjunctivitis ("can't see, can't pee, can't climb a tree")
- NSAIDs are first-line and usually sufficient
- Antibiotics: doxycycline for Chlamydia-triggered (does not alter arthritis course in post-dysenteric)
- DMARDs if refractory: sulfasalazine, methotrexate
- Most resolve within 3-6 months; 20-30% develop chronic arthritis
Enteropathic Arthritis (IBD-associated)
- Affects up to 40% of IBD patients; arthritis often mirrors GI flares
- NSAIDs - first-line for joint pain but may exacerbate IBD (use with caution)
- Sulfasalazine - treats both bowel and joint disease
- Intra-articular corticosteroids - avoid systemic steroids long-term
- Control of underlying IBD (biologics: TNF inhibitors, vedolizumab) - often resolves peripheral arthritis
6.5 Infectious Arthritis
Septic Arthritis (Bacterial)
- EMERGENCY - irreversible joint destruction possible within 24-48 hours
- OPD role: identify and immediately refer to inpatient management
- Signs: fever + single (usually) hot, swollen joint + WCC in synovial fluid >50,000/mm³
- Treatment: empirical IV antibiotics (cover Staph aureus: oxacillin/nafcillin or vancomycin if MRSA risk) + repeated joint drainage
Gonococcal Arthritis
- Most common septic arthritis in young sexually active adults
- Presents as migratory polyarthralgia + tenosynovitis + skin lesions (pustules) → then settles in 1-4 joints
- Cultures often negative; PCR preferred; test all mucosal sites
- Treatment: ceftriaxone 2g IV/IM daily; transition to oral (cefixime) after improvement; add azithromycin 1g once for Chlamydia co-treatment
Lyme Arthritis
- Borrelia burgdorferi (Ixodes tick); endemic areas (northeast USA, parts of Europe)
- Late-stage: asymmetric large joint (knee) effusion
- Treatment: doxycycline 100 mg BD for 28 days (oral); amoxicillin or cefuroxime alternatives
- Prophylaxis after tick bite >24-36 hours: single dose doxycycline 200 mg PO
Viral Arthritis
| Virus | Presentation | Duration | Treatment |
|---|---|---|---|
| Hepatitis B | Symmetric, migratory, urticarial rash | Resolves with onset of jaundice | Supportive |
| Hepatitis C | RA-like symmetric polyarthritis; RF positive | Variable, intermittent | Supportive; HCQ, low-dose MTX |
| HIV | Monoarthritis (feet/ankles), Reiter's-like | Variable | Treat HIV; supportive for joints |
| Parvovirus B19 | Adults: acute symmetric small joints mimicking RA; may have rash | Self-limited 4-6 weeks | Supportive; NSAIDs |
| Chikungunya / Ross River | Epidemic, mosquito-borne; severe polyarthritis/arthralgia | Weeks to months/years | Supportive; corticosteroids in refractory |
| Rubella / vaccine | Symmetric small joints; follows vaccination by 1-2 weeks | Self-limited | Supportive |
| Dengue / Zika | Acute bone and joint pain + high fever | Acute | Supportive |
6.6 Connective Tissue Diseases with Polyarthralgia
Systemic Lupus Erythematosus (SLE)
- Arthritis/arthralgia in >90% - typically symmetric, non-erosive, affecting small joints
- Non-deforming Jaccoud's arthropathy may occur
- Key investigations: ANA (screen), anti-dsDNA, anti-Sm, complement (C3/C4 low), urine for casts
- OPD management of arthritis: hydroxychloroquine (200-400 mg/day) - backbone therapy for all SLE; NSAIDs; low-dose steroids; methotrexate for refractory
Sjögren's Syndrome
- Non-erosive polyarthritis + sicca symptoms (dry eyes, dry mouth)
- Anti-Ro (SS-A) and anti-La (SS-B) antibodies
- Treatment: hydroxychloroquine, pilocarpine (sicca); NSAIDs for arthralgia
Systemic Sclerosis
- Arthralgia, morning stiffness; tenosynovitis; rarely true synovitis
- Raynaud's phenomenon is the dominant feature
- NSAIDs; calcium channel blockers for Raynaud's
6.7 Other Important Causes
Polymyalgia Rheumatica (PMR)
- Age >50 years (almost exclusively); bilateral shoulder/hip girdle stiffness + pain
- ESR consistently >50 mm/hr; CRP elevated
- Dramatic response to prednisolone 15 mg/day (diagnostic + therapeutic)
- Exclude GCA (giant cell arteritis) - temporal artery involvement in 20% of PMR
- Taper steroids very slowly over 12-18 months; DMARDs (tocilizumab, MTX) as steroid-sparing
Adult-Onset Still's Disease (AOSD)
- Classic triad: quotidian fever (spikes to 39°C, resolves within hours) + evanescent salmon-pink rash + polyarthritis
- Ferritin >10,000 ng/mL (highly suggestive); leukocytosis (WCC >15,000)
- Treatment: NSAIDs, systemic corticosteroids, methotrexate; biologics (tocilizumab, anakinra) for refractory
Rheumatic Fever
- Post-streptococcal; migratory large joint polyarthritis; carditis; Sydenham's chorea; subcutaneous nodules; erythema marginatum
- Diagnose by Jones criteria (2 major or 1 major + 2 minor) + evidence of preceding strep infection (positive ASOT)
- Treatment: penicillin (eradicate strep) + aspirin/NSAIDs; steroids for carditis; long-term benzathine penicillin prophylaxis
Fibromyalgia
- Widespread musculoskeletal pain + fatigue + sleep disturbance + cognitive symptoms
- No true arthritis; normal inflammatory markers and imaging
- OPD management: education, aerobic exercise, cognitive behavioral therapy; duloxetine, pregabalin, low-dose amitriptyline
Malignancy-Associated Arthritis (Carcinomatous Polyarthritis)
- Sudden-onset symmetric seronegative polyarthritis in older adults
- Asymmetric large joint involvement, lower limb predominant
- Red flags: no family history, no typical pattern, no response to standard therapy; age >50 with new-onset polyarthritis
- Workup: CT chest/abdomen/pelvis; PSA; mammography; colonoscopy
7. OPD Referral Criteria
| Refer to Rheumatology when: | Refer to Orthopedics when: | Admit urgently when: |
|---|---|---|
| Suspected RA, SpA, SLE, PsA, AOSD, vasculitis | Suspected OA requiring surgical evaluation | Hot single joint (rule out septic arthritis) |
| Polyarthritis undiagnosed after initial workup | Mechanical derangement | Suspected septic arthritis |
| Positive anti-CCP or ANA with arthritis | Failed conservative OA management | Gonococcal arthritis |
| Suspected seronegative SpA | Joint replacement consultation | SLE with nephritis/cerebritis |
| Failure to respond to NSAIDs within 4-6 weeks | High fever + polyarthritis |
8. OPD Monitoring Protocol Summary
| Diagnosis | Frequency | What to monitor |
|---|---|---|
| RA on MTX | Every 3 months | CBC, LFT, RFT, DAS28 |
| RA on biologics | Every 3-6 months | CBC, LFT, screen for infections; TB annually |
| Gout on allopurinol | Every 6 months | Serum uric acid (target <6 mg/dL), RFT |
| OA | Annual | Functional status, X-ray if change in symptoms |
| SLE | Every 1-3 months depending on activity | CBC, complement, anti-dsDNA, urinalysis |
| PMR | Every 4-6 weeks during steroid taper | ESR/CRP, glucose, BP, bone density |
| SpA on biologics | Every 6 months | ASDAS/BASDAI, screen for TB, DEXA |
9. Quick Reference: Key Autoantibodies and Their Disease Associations
| Antibody | Sensitivity | Disease Association |
|---|---|---|
| RF | 60-70% | RA (also Sjögren's, SBE, viral hepatitis, scleroderma) |
| Anti-CCP/ACPA | 60-70% but high specificity | RA (predicts erosive disease) |
| ANA | 95-99% | SLE screening (low specificity) |
| Anti-dsDNA | 70% | SLE (specific; correlates with disease activity) |
| Anti-Sm | 25-30% | SLE (highly specific) |
| Anti-Ro/SSA, Anti-La/SSB | 60-70% | Sjögren's, SLE, neonatal lupus |
| Anti-Scl-70 | 30-40% | Diffuse systemic sclerosis |
| Anti-centromere | 80-90% | Limited systemic sclerosis (CREST) |
| HLA-B27 | >90% | Ankylosing spondylitis |
| Anti-Jo1 | 20-30% | Polymyositis/dermatomyositis |
10. Practical OPD Prescribing Pearls
- NSAIDs: always prescribe with gastroprotection (PPI) in patients >60 years, history of peptic ulcer, or on anticoagulants
- Colchicine: narrow therapeutic window; reduce dose in renal impairment; interactions with statins (myopathy risk)
- Methotrexate: always co-prescribe folic acid 5 mg/week (not on the same day as MTX); check CBC + LFT before each prescription increase
- Hydroxychloroquine: safe in pregnancy; annual ophthalmology review (retinal toxicity at cumulative dose >5 mg/kg/day)
- Biologics: screen for latent TB (IGRA or Mantoux + CXR) before starting; withhold during active infection; live vaccines contraindicated
- Corticosteroids: always counsel on bone protection (calcium + vitamin D); use bisphosphonate if >3 months treatment anticipated
- Allopurinol: start LOW (50-100 mg/day), titrate slowly (risk of drug reaction with eosinophilia and systemic symptoms - DRESS if escalated rapidly); HLA-B*58:01 screening before starting in Han Chinese, Thai, Korean populations
Sources: Firestein & Kelley's Textbook of Rheumatology (2-Volume Set), p. 809-812 | ROSEN's Emergency Medicine, p. 2336-2342 | Rheumatology 2-Volume Set, Elsevier 2022, p. 7113-7160 | Goldman-Cecil Medicine International Edition
This is a shared conversation. Sign in to Orris to start your own chat.