RBF OF RENAL PHYSIOLOGY WITH DETAILED EXPLANATION with flowcharts
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compose the complete, detailed answer with flowcharts using text-based diagrams.
Renal Blood Flow (RBF) - Complete Physiology Guide
1. Overview and Normal Values
The kidneys receive a disproportionately large fraction of cardiac output relative to their size:
| Parameter | Value |
|---|---|
| RBF (combined both kidneys) | ~1100-1200 mL/min (~22-25% of cardiac output) |
| Renal Plasma Flow (RPF) | ~634 mL/min (combined) |
| RBF in Men | ~1166 mL/min |
| RBF in Women | ~940 mL/min |
| Kidney weight | ~0.4% of total body weight |
| Renal O₂ consumption | 2x brain per gram weight |
The two kidneys make up only 0.4% of body weight yet receive 22-25% of cardiac output. This high flow is NOT merely to meet metabolic needs - it exists to supply enough plasma for the high rates of glomerular filtration needed for precise regulation of body fluid volume and solute concentration. - Guyton and Hall Textbook of Medical Physiology, p.340
2. The Fundamental Formula
Renal Artery Pressure - Renal Vein Pressure
RBF = ─────────────────────────────────────────────
Total Renal Vascular Resistance
- Renal artery pressure ≈ systemic arterial pressure (~100 mm Hg)
- Renal vein pressure ≈ 3-4 mm Hg
- Therefore: driving pressure ≈ 96-97 mm Hg
3. Renal Vascular Resistance - Segmental Distribution
The resistance is distributed across multiple segments. Most resistance resides in three key areas:
| Vessel | Pressure (Start) | Pressure (End) | % of Total Resistance |
|---|---|---|---|
| Renal artery | 100 mm Hg | 100 mm Hg | ~0% |
| Interlobar, arcuate, interlobular arteries | ~100 mm Hg | 85 mm Hg | ~16% |
| Afferent arteriole | 85 mm Hg | 60 mm Hg | ~26% |
| Glomerular capillaries | 60 mm Hg | 59 mm Hg | ~1% |
| Efferent arteriole | 59 mm Hg | 18 mm Hg | ~43% |
| Peritubular capillaries | 18 mm Hg | 8 mm Hg | ~10% |
| Interlobar/arcuate/interlobular veins | 8 mm Hg | 4 mm Hg | ~4% |
| Renal vein | 4 mm Hg | ~4 mm Hg | ~0% |
Source: Guyton and Hall Textbook of Medical Physiology, Table 27.3
The efferent arteriole provides the highest resistance (~43%) followed by the afferent arteriole (~26%). This two-arteriole arrangement is unique to the kidney and is the primary mechanism for regulating both RBF and GFR independently.
4. How to Calculate RBF - The PAH Clearance Method
Step 1: Calculate Renal Plasma Flow (RPF) using PAH clearance
PAH (para-aminohippuric acid) is filtered AND actively secreted by proximal tubules - 80-90% is extracted in a single pass.
U_PAH × V
C_PAH = ─────────── = Effective RPF
P_PAH
Where:
U_PAH = urine concentration of PAH
V = urine flow rate (mL/min)
P_PAH = plasma concentration of PAH
Step 2: Convert RPF to RBF using hematocrit
RPF
RBF = ─────────
1 - Hct
Where:
Hct = hematocrit (fraction)
1 - Hct = plasma fraction of blood
Example: If RPF = 600 mL/min, Hct = 0.45:
RBF = 600 / (1 - 0.45) = 600 / 0.55 ≈ 1091 mL/min
Costanzo Physiology 7th Edition, p.264
Filtration Fraction (FF)
GFR ~125 mL/min
FF = ───── = ────────────── ≈ 0.20 (normal ~19-20%)
RPF ~625 mL/min
Normally about 20% of the renal plasma that enters the glomerulus is filtered. - Brenner and Rector's The Kidney, Table 3.1
5. Regional Distribution of Blood Flow
RENAL BLOOD FLOW DISTRIBUTION
───────────────────────────────
Total RBF: ~1100 mL/min
│
├─── Renal CORTEX (~98-99%)
│ High flow → active tubular secretion/reabsorption
│ Glomeruli + proximal tubules
│
└─── Renal MEDULLA (~1-2%)
Supplied by VASA RECTA
Low flow → preserves medullary osmotic gradient
Runs parallel with loops of Henle
Critical for urine concentration
The deliberately low medullary flow is physiologically important - if medullary blood flow were high, it would wash away the osmotic gradient required for concentrated urine formation. - Guyton and Hall
6. RBF and Oxygen Consumption
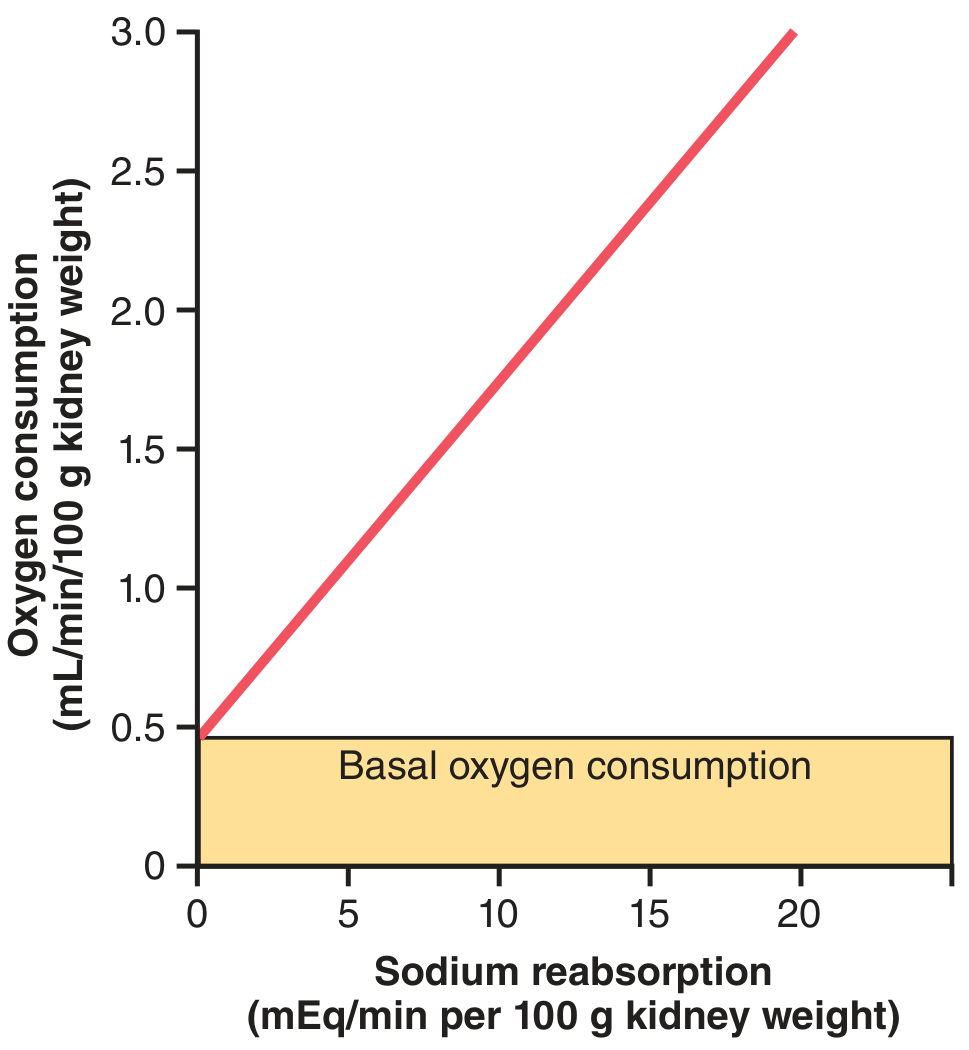
- Kidneys consume oxygen at 2x the rate of the brain per gram weight
- Yet they receive 7x the blood flow of the brain - so A-V O₂ extraction is LOW
- The majority of renal O₂ consumption is driven by active Na⁺ reabsorption (Na⁺/K⁺-ATPase)
- If GFR falls → less Na⁺ filtered → less reabsorption needed → O₂ consumption falls
- If GFR ceases completely → renal O₂ consumption drops to ~1/4 of normal (basal metabolic needs only)
7. Regulation of RBF - Vasoconstrictors and Vasodilators
The kidney has two sets of arterioles (unique!). Changing resistance at either one affects RBF and GFR differently.
REGULATION OF RBF
─────────────────────────────────────────────────────────
VASOCONSTRICTORS │ VASODILATORS
────────────────── │ ─────────────────
• Sympathetic nerves │ • PGE₂ (prostaglandin E₂)
(catecholamines, α₁-R) │ • PGI₂ (prostacyclin)
• Angiotensin II │ • Nitric oxide (NO)
• Endothelin │ • Bradykinin
│ • Dopamine
│ • Atrial natriuretic peptide (ANP)
Source: Costanzo Physiology 7th Edition, Table 6.5
7a. Sympathetic Nervous System
↑ Sympathetic activity (e.g., hemorrhage)
│
▼
Activation of α₁ receptors on afferent (primarily) and efferent arterioles
│
▼
VASOCONSTRICTION (afferent > efferent due to more α₁ receptors)
│
▼
↑ Afferent resistance → ↓ RBF and ↓ GFR
Purpose: During hemorrhage, the body sacrifices renal perfusion to maintain systemic blood pressure via the baroreceptor reflex. - Costanzo Physiology 7th Edition, p.263
7b. Angiotensin II
Low Ang II levels:
→ Preferential constriction of EFFERENT arteriole
→ ↓ RBF but ↑ GFR (increased filtration fraction)
High Ang II levels:
→ Constricts BOTH afferent AND efferent arterioles
→ ↓ RBF AND ↓ GFR
Efferent arterioles are MORE sensitive to Ang II than afferent arterioles. This differential sensitivity is why low-dose Ang II (e.g., mild volume depletion) can maintain GFR even when RBF falls.
7c. Prostaglandins (PGE₂, PGI₂)
- Released locally under stress (volume depletion, surgery)
- Dilate afferent arterioles → oppose excessive vasoconstriction
- Clinical relevance: NSAIDs (e.g., aspirin, ibuprofen) block prostaglandin synthesis → significant ↓ GFR in volume-depleted patients or post-surgery - Guyton and Hall, p.342
7d. Nitric Oxide (NO)
- Produced by vascular endothelium
- Tonically dilates both arterioles
- Major vasodilator counterbalancing Ang II
8. Autoregulation of RBF
The Core Concept
Despite wide fluctuations in mean arterial pressure (MAP), RBF and GFR remain remarkably constant:
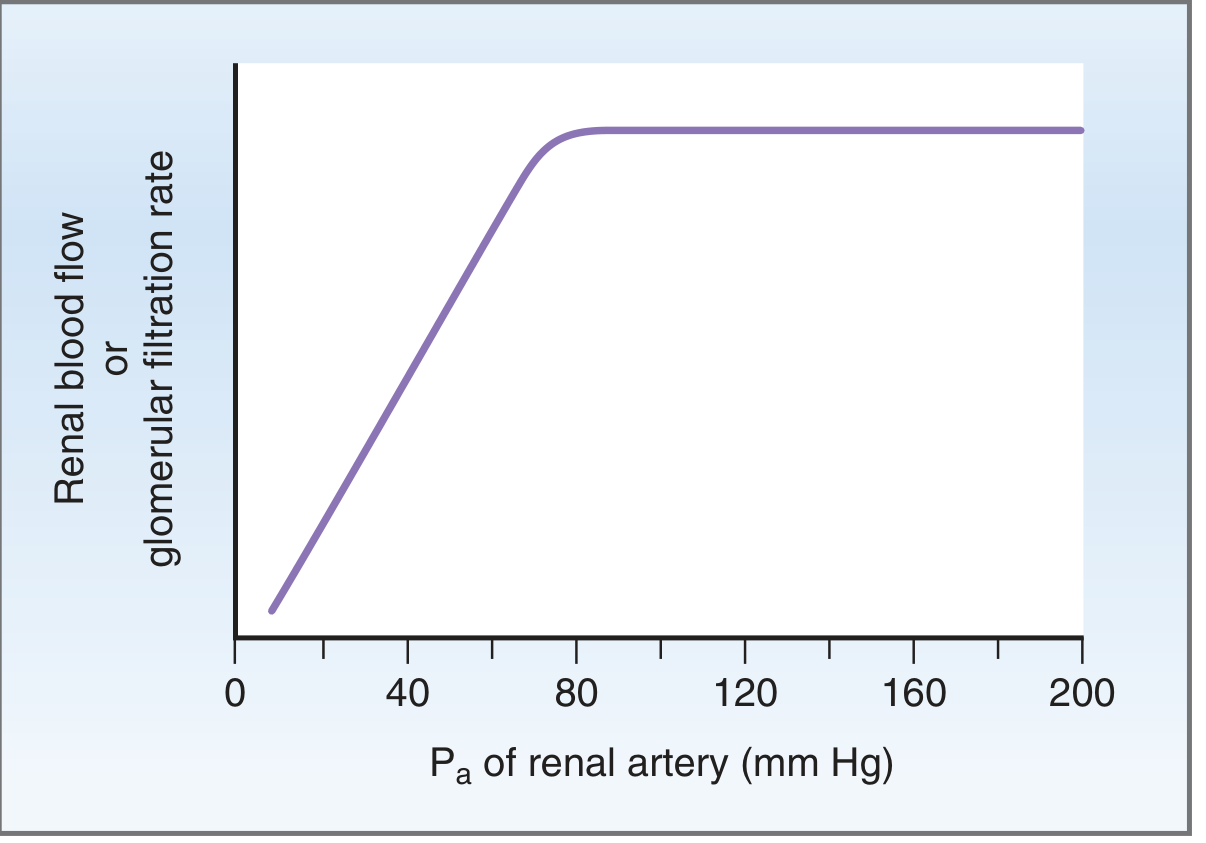
Autoregulation range: MAP 80-170 mm Hg (Guyton) / 80-200 mm Hg (Costanzo)
- Below 80 mm Hg → RBF falls proportionately
- Above 170-200 mm Hg → autoregulation overwhelmed
- GFR changes < 10% across this range
Key feature: Autoregulation persists in a denervated (transplanted) kidney - it is intrinsic to the kidney, not dependent on the autonomic nervous system.
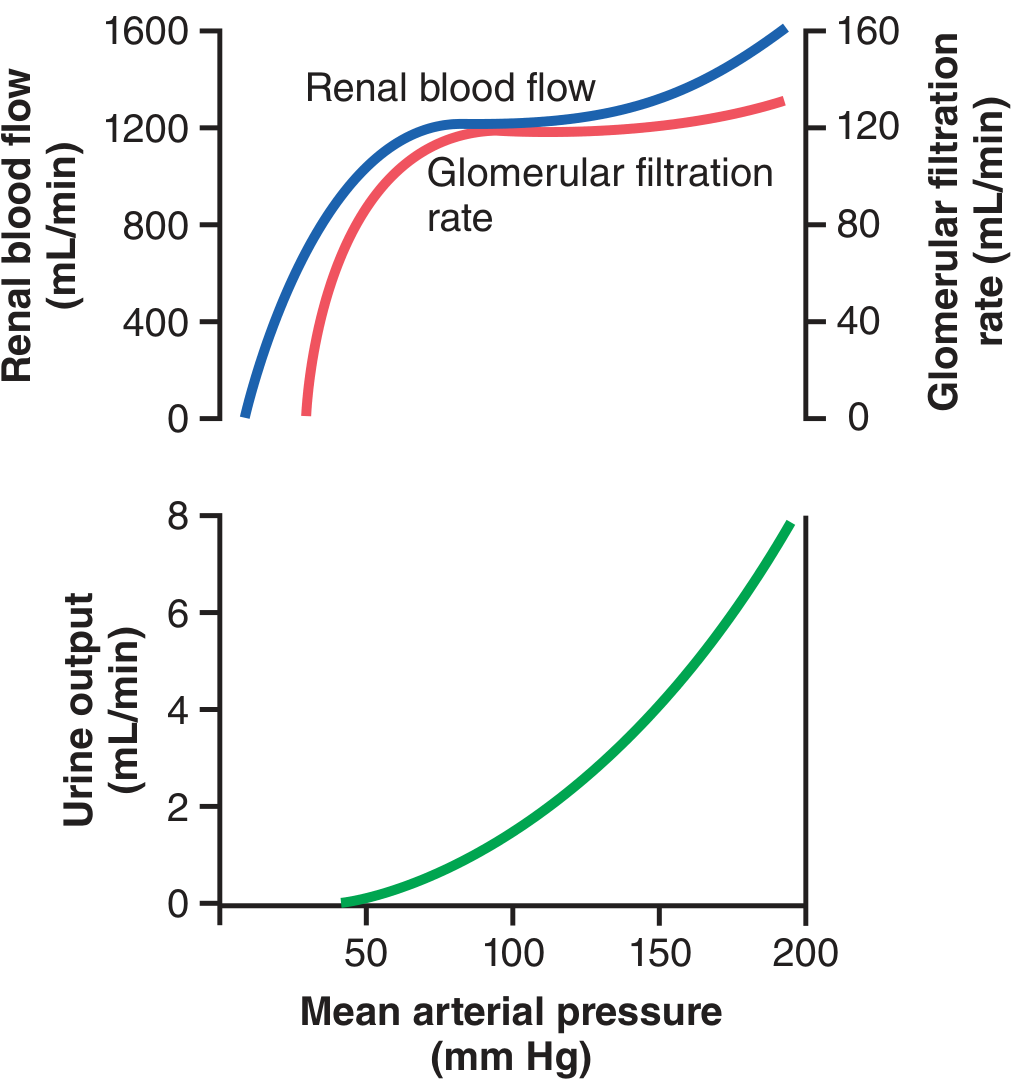
Why Autoregulation Matters
Without autoregulation, a 25% rise in blood pressure (100→125 mm Hg) would increase GFR from 180 to 225 L/day. With tubular reabsorption fixed at ~178.5 L/day, urine output would rise from 1.5 to 46.5 L/day - a 30-fold increase that would rapidly deplete plasma volume (~3L total). - Guyton and Hall, p.343
9. Mechanisms of Autoregulation
Mechanism 1: Myogenic Response
↑ Renal arterial pressure
│
▼
Stretching of afferent arteriole wall
│
▼
Stretch-activated Ca²⁺ channels OPEN
│
▼
Ca²⁺ influx into vascular smooth muscle
│
▼
Smooth muscle contraction
│
▼
↑ Afferent arteriolar resistance
│
▼
↓ Blood flow entering glomerulus → RBF restored to normal
This is a rapid (within seconds) intrinsic response of smooth muscle. - Costanzo Physiology 7th Edition, p.264
Mechanism 2: Tubuloglomerular Feedback (TGF)
This is the more sophisticated feedback loop, mediated by the juxtaglomerular apparatus (JGA).
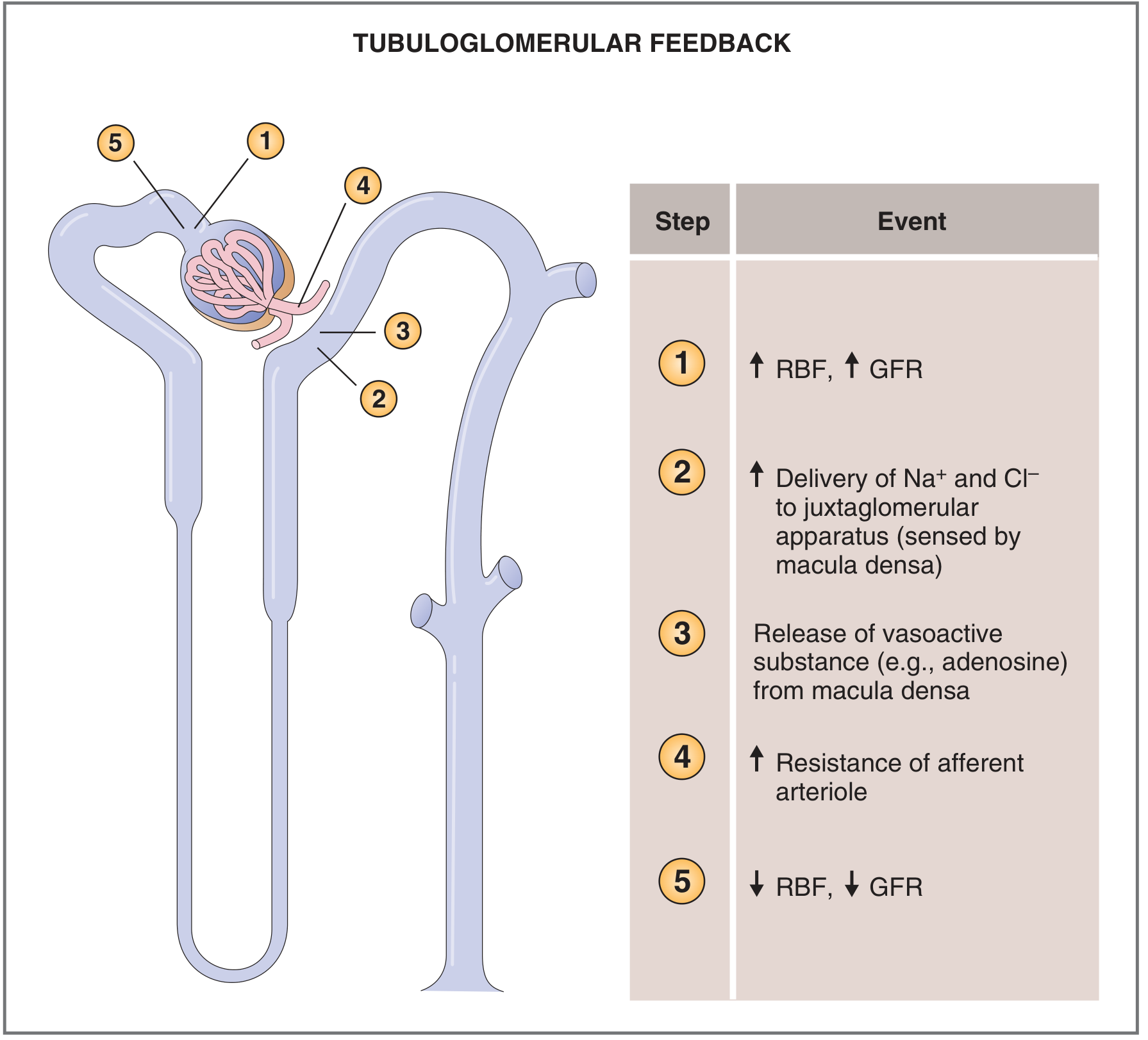
FLOWCHART - TGF when RBF/GFR increases:
↑ MAP → ↑ RBF → ↑ GFR
│
▼
↑ Tubular flow rate → ↑ NaCl delivery to MACULA DENSA
(early distal tubule / juxtaglomerular apparatus)
│
▼
Macula densa senses ↑ NaCl via Na⁺-K⁺-2Cl⁻ cotransporter
│
▼
Cell depolarization → ATP release → converted to ADENOSINE
│
▼
Adenosine constricts AFFERENT arteriole (paracrine)
│
▼
↑ Afferent resistance → ↓ glomerular hydrostatic pressure
│
▼
↓ RBF and ↓ GFR → restored toward normal ✓
FLOWCHART - TGF when RBF/GFR decreases:
↓ MAP → ↓ RBF → ↓ GFR
│
▼
↓ NaCl delivery to macula densa
│
▼
Reduced NaCl sensing → less adenosine released
│
▼
↓ Afferent arteriolar tone → afferent DILATES
│
▼
Also: Renin release ↑ from JG cells → ↑ Ang II → efferent constricts
│
▼
Glomerular hydrostatic pressure maintained → GFR preserved
Modulators of TGF sensitivity:
- Angiotensin II → enhances TGF sensitivity (efferent feedback component)
- Nitric oxide → decreases TGF sensitivity (blunts feedback)
- Prostaglandins → decrease TGF sensitivity
10. Master Flowchart - Complete RBF Regulation Overview
BLOOD PRESSURE CHANGES
│
┌────────────┴────────────┐
↑ MAP ↓ MAP
│ │
┌─────────▼──────────┐ ┌──────────▼─────────┐
│ Myogenic response │ │ Myogenic response │
│ Afferent arteriole │ │ Afferent arteriole │
│ CONSTRICTS │ │ DILATES │
└─────────┬──────────┘ └──────────┬──────────┘
│ │
┌─────────▼──────────┐ ┌──────────▼─────────┐
│ TGF: ↑GFR→↑NaCl │ │TGF: ↓GFR→↓NaCl │
│ at macula densa │ │at macula densa │
│ → Adenosine → │ │→ Less adenosine │
│ afferent constricts│ │→ afferent dilates │
└─────────┬──────────┘ │+ ↑Renin→↑Ang II │
│ │→ efferent constricts│
│ └──────────┬──────────┘
│ │
┌─────────▼──────────┐ ┌──────────▼─────────┐
│ ↓ Glomerular P │ │↑ Glomerular P │
│ ↓ GFR corrected │ │↑ GFR restored │
└─────────┬──────────┘ └──────────┬──────────┘
│ │
└────────────┬────────────┘
▼
RBF and GFR MAINTAINED
(Autoregulation)
11. Key Clinical Correlates
| Situation | RBF Change | Mechanism |
|---|---|---|
| Hemorrhage / volume depletion | ↓↓ RBF | ↑ SNS → α₁ afferent constriction + ↑ Ang II |
| NSAID use in volume-depleted patient | ↓ RBF, ↓ GFR (AKI risk) | Blocks PGE₂/PGI₂ vasodilation of afferent |
| ACE inhibitors in renal artery stenosis | ↓ GFR (AKI risk) | Blocks Ang II → efferent dilates → glomerular P falls |
| Unilateral renal artery stenosis | ↓ RBF to affected kidney | Fixed mechanical obstruction |
| Exercise | ↓ RBF transiently | ↑ SNS activity redistributes flow to muscle |
| Low-protein diet | ↓ RBF (mild) | Lower metabolic demand, lower GFR set point |
| Sepsis | ↓ RBF (variable) | Endothelin, Ang II, ↑ SNS; NO counteracts |
12. Summary Table
| Parameter | Normal Value | Key Regulator |
|---|---|---|
| RBF | ~1100-1200 mL/min | Arteriolar resistance (afferent + efferent) |
| RPF | ~600-650 mL/min | RPF = RBF × (1 - Hct) |
| GFR | ~125 mL/min | Glomerular hydrostatic pressure |
| Filtration Fraction | ~19-20% | GFR/RPF |
| Autoregulation range | 80-170 mm Hg MAP | Myogenic + TGF |
| Cortical flow | ~98-99% of RBF | High metabolic demand |
| Medullary flow | ~1-2% of RBF | Vasa recta (preserves gradient) |
Sources:
- Guyton and Hall Textbook of Medical Physiology, Chapter 27 (pp. 340-344)
- Costanzo Physiology 7th Edition, Chapter 6 (pp. 262-265)
- Brenner and Rector's The Kidney, Chapter 3, Table 3.1
This is a shared conversation. Sign in to Orris to start your own chat.