Give me All lesion classification on FNAC
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have comprehensive data from multiple authoritative textbooks. Let me compile the complete answer:
FNAC (Fine Needle Aspiration Cytology) - All Lesion Classification Systems
FNAC reporting has been standardized by organ-specific classification systems. Below are all the major classifications used worldwide.
1. THYROID FNAC Classifications
A. The Bethesda System for Reporting Thyroid Cytopathology (BSRTC) - 2023 (3rd edition)
The most widely used international standard, developed by the National Cancer Institute. Six tiered categories:
| Bethesda Category | Diagnosis | Risk of Malignancy (NIFTP ≠ cancer) | Risk of Malignancy (NIFTP = cancer) | Usual Management |
|---|---|---|---|---|
| I | Nondiagnostic / Unsatisfactory | 5%-18% | 5%-20% | Repeat FNA with ultrasound guidance |
| II | Benign | 0%-4% | 2%-7% | Clinical and sonographic follow-up |
| III | Atypia of Undetermined Significance (AUS) / Follicular Lesion of Undetermined Significance (FLUS) | 6%-24% | ~13%-30% | Repeat FNA, molecular testing, or lobectomy |
| IV | Follicular Neoplasm (FN) / Suspicious for Follicular Neoplasm | 17%-28% | 23%-34% | Molecular testing or lobectomy |
| V | Suspicious for Malignancy | 58%-74% | 67%-83% | Near-total thyroidectomy or lobectomy |
| VI | Malignant | 94%-96% | 97%-100% | Near-total thyroidectomy or lobectomy |
NIFTP = Noninvasive Follicular Thyroid Neoplasm with Papillary-like nuclear features
- Source: Sabiston Textbook of Surgery, Table 73.3
Category VI (Malignant) includes: Papillary thyroid carcinoma, medullary carcinoma, poorly differentiated carcinoma, undifferentiated (anaplastic) carcinoma, squamous cell carcinoma, carcinoma with mixed features, metastatic carcinoma, and non-Hodgkin lymphoma.
B. BTA/RCPath "Thy" System (UK)
The British Thyroid Association / Royal College of Pathologists system:
| Code | Cytological Diagnosis | Management |
|---|---|---|
| Thy1 | Non-diagnostic | US assessment +/- repeat FNAB |
| Thy1c | Non-diagnostic - cystic lesion | Repeat or clinical correlation |
| Thy2 | Non-neoplastic (benign) | Correlate with clinical/US findings |
| Thy2c | Non-neoplastic - cystic lesion | Correlate clinically |
| Thy3a | Neoplasm possible - atypia (uncategorized) | Further US +/- repeat FNAB |
| Thy3f | Neoplasm possible - possible follicular neoplasm | Diagnostic hemithyroidectomy |
| Thy4 | Suspicious of malignancy | Diagnostic hemithyroidectomy |
| Thy5 | Diagnostic of malignancy (Malignant) | Surgical resection / near-total thyroidectomy |
- Source: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1; Bailey & Love's Short Practice of Surgery 28th Ed.
C. Italian TIR System
| Code | Diagnosis | Risk of Malignancy |
|---|---|---|
| TIR 1 | Non-diagnostic | - |
| TIR 1c | Non-diagnostic cystic | - |
| TIR 2 | Non-malignant | <3% |
| TIR 3A | Low Risk Indeterminate Lesion (LRIL) | <10% |
| TIR 3B | High Risk Indeterminate Lesion (HRIL) | 15%-30% |
| TIR 4 | Suspicious of malignancy | 60%-80% |
| TIR 5 | Malignant | >95% |
D. Japanese System
| Code | Diagnosis | Risk of Malignancy |
|---|---|---|
| 1 | Inadequate | ~10% |
| 2 | Normal or benign | <1% |
| 3A | Follicular neoplasm A-1 (favour benign) | <15% |
| 3A | Follicular neoplasm A-2 (borderline) | 15%-30% |
| 3A | Follicular neoplasm A-3 (favour malignant) | 40%-60% |
| 3B | Indeterminate - Others | 40%-60% |
| 4 | Malignancy suspected | >80% |
| 5 | Malignant | - |
E. Australian System
| Code | Diagnosis | Risk of Malignancy |
|---|---|---|
| 1 | Non-diagnostic | 0%-10% |
| 2 | Benign | 0%-3% |
| 3 | Indeterminate / follicular lesion of undetermined significance | 5%-15% |
| 4 | Suggestive of a follicular neoplasm | 15%-30% |
| 5 | Suspicious of malignancy | 60%-75% |
| 6 | Malignant | >97% |
- All thyroid comparison data from: Scott-Brown's Otorhinolaryngology, Table 58.1
2. SALIVARY GLAND FNAC - Milan System
Proposed by an international panel of experts (American Society of Cytopathology and International Academy of Cytology). Six categories:
| Category | Diagnosis | Risk of Malignancy | Usual Management |
|---|---|---|---|
| I | Non-diagnostic | 25% | Clinical/radiological correlation; repeat FNAC |
| II | Non-neoplastic | 10% | Clinical follow-up and radiological correlation |
| III | Atypia of Undetermined Significance (AUS) | 20% | Repeat FNAC or surgery |
| IVA | Benign Neoplasm | <5% | Conservative surgery or clinical follow-up |
| IVB | Salivary Gland Neoplasm of Uncertain Malignant Potential (SUMP) | 35% | Conservative surgery* |
| V | Suspicious for malignancy | 60% | Surgery* |
| VI | Malignant | >90% | Surgery* (extent depends on type and grade) |
Intraoperative frozen section may help determine extent of surgery
- Source: Bailey & Love's Short Practice of Surgery 28th Ed., Table 54.4; Cummings Otolaryngology Head & Neck Surgery
Category details:
- Non-neoplastic (II): Includes inflammatory, metaplastic, and reactive processes - requires clinicoradiologic correlation
- AUS (III): Reactive atypia or poorly sampled neoplasms - requires repeat FNA or surgery
- Benign Neoplasm (IVA): Clear-cut benign neoplasms (e.g. pleomorphic adenoma, Warthin tumour)
- SUMP (IVB): Neoplasm identified but specific entity cannot be determined and malignancy cannot be excluded
3. CERVICAL / ANAL CYTOLOGY - Bethesda Classification
| Category | Meaning |
|---|---|
| Negative for Intraepithelial Lesion or Malignancy (NILM) | Normal / reactive changes |
| ASC-US | Atypical Squamous Cells of Undetermined Significance |
| ASC-H | Atypical Squamous Cells - cannot exclude HSIL |
| LSIL | Low-Grade Squamous Intraepithelial Lesion (CIN 1, HPV effect) |
| HSIL | High-Grade Squamous Intraepithelial Lesion (CIN 2/3) |
| SCC | Squamous Cell Carcinoma |
| AGC | Atypical Glandular Cells |
| AIS | Adenocarcinoma in Situ |
| Adenocarcinoma | Malignant glandular lesion |
The same Bethesda classification is applied to anal cytology with parallel terminology.
- Source: Tietz Textbook of Laboratory Medicine 7th Ed.; Pfenninger and Fowler's Procedures for Primary Care
4. BREAST FNAC - UK/NHS Classification (C-coding)
The standard UK breast FNAC reporting uses a 5-tier C-code system:
| Code | Category | Description |
|---|---|---|
| C1 | Inadequate/Non-diagnostic | Insufficient material for diagnosis |
| C2 | Benign | Benign epithelial cells, no malignant features |
| C3 | Atypia - probably benign | Atypical cells but most likely benign (equivocal) |
| C4 | Suspicious - probably malignant | Atypical cells with high suspicion of malignancy |
| C5 | Malignant | Diagnostic of malignancy |
Note: Breast FNAC is increasingly being supplemented or replaced by core biopsy, which provides architectural assessment and allows ER/PR/HER2 receptor testing.
5. GENERAL / GENERIC FNAC Classification
For non-organ-specific or general purpose reporting, the following broad five-tier scheme is used in many centers:
| Category | Description |
|---|---|
| Unsatisfactory | Insufficient cells for diagnosis; <6 follicles of 10+ cells (thyroid equivalent) |
| Benign / Non-neoplastic | No evidence of malignancy; benign features |
| Indeterminate / Atypical | Equivocal; cannot classify as clearly benign or malignant |
| Suspicious of malignancy | Features highly suggestive but not diagnostic of malignancy |
| Malignant | Diagnostic of malignancy (specify type: carcinoma, lymphoma, sarcoma, etc.) |
Histological Cytological Images - Bethesda Thyroid Categories
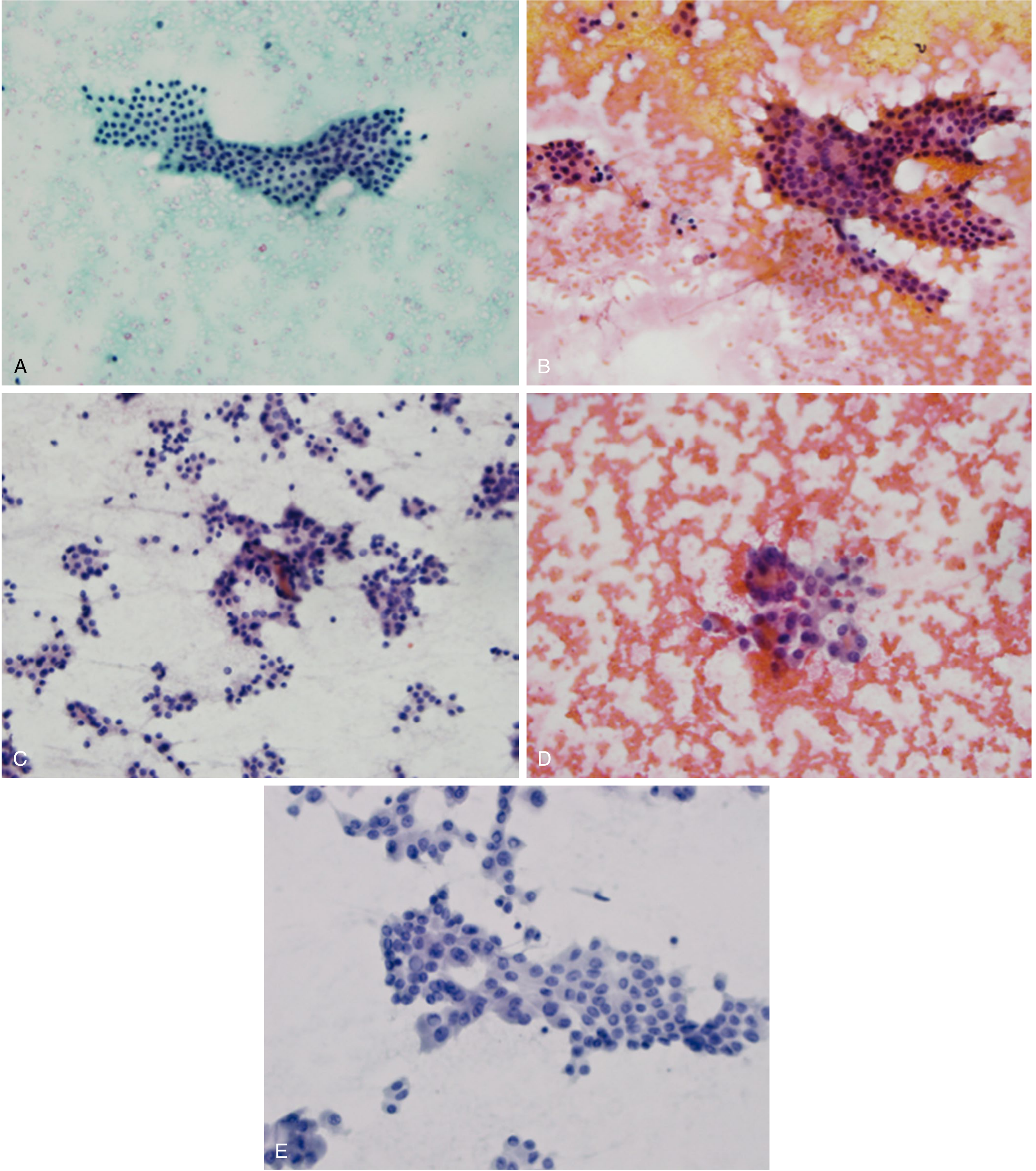
Representative cytologic features by Bethesda category: (A) Cat. II - benign colloid nodule with bland follicular cells in macrofollicular pattern; (B) Cat. III - AUS with nuclear enlargement and occasional intranuclear grooves; (C) Cat. IV - follicular neoplasm with highly cellular aspirate in microfollicles; (D) Cat. V - suspicious for PTC with nuclear enlargement and pale chromatin; (E) Cat. VI - PTC with "Orphan Annie eye" nuclei and intranuclear pseudoinclusions.
- Source: Sabiston Textbook of Surgery
Summary Table - FNAC Classification Systems by Organ
| Organ / Site | Classification System | No. of Categories |
|---|---|---|
| Thyroid | Bethesda System (BSRTC) - International | 6 |
| Thyroid | BTA/RCPath Thy System - UK | 6 (Thy1-Thy5 + subcategories) |
| Thyroid | Italian TIR System | 6 |
| Thyroid | Japanese System | 5 |
| Thyroid | Australian System | 6 |
| Salivary Gland | Milan System | 6 (I-VI) |
| Breast | C-coding System (UK/NHS) | 5 (C1-C5) |
| Cervix / Anal | Bethesda Cervical Classification | Multiple (NILM, ASC-US, LSIL, HSIL, etc.) |
| General / Generic | Five-tier scheme | 5 |
Key Clinical Principle: Regardless of organ system, all FNAC classification systems share the same fundamental principle - stratifying lesions by risk of malignancy to guide clinical management (repeat FNA, observation, surgery). The non-diagnostic and indeterminate categories are the most clinically challenging and often require additional workup (repeat FNA, molecular testing, or core biopsy).
Sources: Bailey & Love's Short Practice of Surgery 28th Ed. | Sabiston Textbook of Surgery | Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 | Cummings Otolaryngology Head & Neck Surgery | Tietz Textbook of Laboratory Medicine 7th Ed.
Nodules swelling below right ear since one month on aspiration sorrows metrical can ?
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Microscopy shows occasional lymphocytes with occasional cyst macrophage against proteinaceous background.
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Create a diagnostic flowchart for neck cysts with FNAC findings
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.