drunkometer in forensic medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a thorough answer. Here is a complete, well-organized summary:
Drunkometer in Forensic Medicine
What It Is
The drunkometer (also called breath analyser, alcometer, or intoximeter) is a device used for detecting alcohol in expired (exhaled) air. It is one of the most common preliminary screening tests used by law enforcement agencies for roadside detection of drunken driving.
Fig: Modern digital breath analyzer (alcometer/drunkometer)
Basic Principle
The test is based on the Breath-Blood Alcohol Ratio:
2100 mL of alveolar air = 1 mL of blood in terms of alcohol content
This ratio is constant at a given temperature (reference temperature of exhaled air ~34°C). The alcohol concentration in deep lung (alveolar) air is dependent on arterial blood. So, the breath alcohol content closely mirrors the blood alcohol concentration (BAC). - The Essentials of Forensic Medicine and Toxicology, 36th ed. and PC Dikshit Textbook of Forensic Medicine and Toxicology
Chemical Reaction (Classic Drunkometer)
The subject blows 60-100 mL of breath into:
- A dry balloon or plastic bag, OR
- Directly into a glass tube containing the reagent mixture
The reagent is a crystalline bichromate-sulfuric acid (dichromate-H₂SO₄) mixture.
Reaction:
When exhaled air containing ethyl alcohol is passed over concentrated sulfuric acid + dichromate crystals:
Ethyl alcohol + Dichromate (orange/yellow) → Greenish colour change
- The intensity of the green colour is proportional to the amount of alcohol present
- A BAC >80 mg% is considered a positive result (green colour) - PC Dikshit Textbook
Procedure
- The person is asked to blow into a special container or directly into the breath analyser
- 60-100 mL of exhaled (deep lung) breath is collected
- The breath contacts the bichromate-sulfuric acid reagent
- Colour change (yellow/orange → green) indicates the presence and amount of alcohol
- This is a qualitative/semi-quantitative screening test
Modern (electronic) breathalyzers do NOT necessarily rely on chemical oxidation - they use electrochemical or infrared sensors and give quantitative results, with some producing printed output accepted for court work. - Parikh's Textbook of Medical Jurisprudence
Causes of False Positive Results
| Cause | Explanation |
|---|---|
| Residual mouth alcohol | Alcohol may remain in the mouth up to 20-30 minutes after even a small peg - test must be repeated after 20 minutes |
| Hyperventilation | Lowers alveolar alcohol concentration (actually gives false low) |
| Physical exercise | Can affect readings |
| Emesis / Regurgitation | Stomach contents containing alcohol can contaminate breath sample |
| Acetone, ether, paraldehyde | May be estimated as alcohol by some devices |
To preserve breath samples, plastic, aluminium, and other flexible bags are available, allowing samples to be kept for several hours for re-analysis. - PC Dikshit Textbook
Comparison with Other Samples for Alcohol Analysis
| Sample | Notes |
|---|---|
| Blood | Best sample; gives direct evidence of BAC in brain; peripheral vein preferred |
| Urine | 20% higher than blood; two samples needed (1st to empty bladder, 2nd after 25-30 min); urine alcohol lags blood by 20-25 min |
| Breath | Rapid, non-invasive; good screening tool; 2100 mL air = 1 mL blood |
| Saliva | ~same as blood alcohol |
| Vitreous humour | Useful postmortem; resistant to putrefaction; used when blood unavailable |
Legal / Medicolegal Significance
- The drunkometer/breathalyser is the primary roadside screening test used by police
- In India, the statutory blood alcohol limit is 30 mg% under Section 185, Motor Vehicles Act 1988
- First offence: fine up to ₹5,000 or 6 months imprisonment or both
- Subsequent offences: fine up to ₹3,000 or 2 years imprisonment or both
- Electronic breath analysers with printed output have been accepted for court work in some countries abroad
- A limitation: if alcohol absorption is not yet complete at the time of testing, BAC may be overestimated - Parikh's Textbook
Widmark Formula (Supplementary)
When direct BAC is unavailable, the Widmark formula estimates total body alcohol:
a = p × r × c
Where:
- a = weight of alcohol in the body (grams)
- p = body weight (kg)
- r = distribution constant (0.68 for males; 0.55 for females)
- c = concentration of alcohol in blood (mg/kg)
This is used in forensic reconstruction of BAC at the time of an incident. - PC Dikshit Textbook of Forensic Medicine and Toxicology
Sources:
SLE
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I have a very thorough dataset from Harrison's 22e (2025) and Goldman-Cecil. I now have everything needed for a comprehensive answer.
Systemic Lupus Erythematosus (SLE)
Definition
SLE is a multisystem autoimmune disease in which overactive innate and adaptive immune systems cause tissue damage through the effects of autoantibodies and immune complexes. It targets multiple organ systems - cutaneous, musculoskeletal, renal, pulmonary, cardiovascular, hematologic, serosal, and CNS. The course is typically waxing and waning. - Harrison's 22e (2025)
Epidemiology
| Feature | Detail |
|---|---|
| Sex ratio | Female : Male = 9:1 in adults |
| Peak age | 15-44 years (childbearing age) |
| US prevalence | ~72.8 per 100,000 |
| Incidence | ~5.1 per 100,000/year |
| Racial disparity | Black women > Hispanic > White; Black men have highest prevalence among men |
| Children / >55 yrs | F:M ratio closer to 2:1 |
~90% of affected individuals are women. Prognosis varies by geographic region, ethnicity, and access to care. - Harrison's 22e; Goldman-Cecil Medicine
Pathogenesis
Genetic Factors
- Multiple susceptibility genes (polygenic, cumulative-hit model)
- Impaired inactivation of the X-chromosome may explain the female predominance
- Strong HLA associations (HLA-DR2, HLA-DR3)
- Complement deficiencies (C1q, C2, C4) predispose to SLE
Environmental Triggers
- UV light - alters DNA methylation, generates stimulatory nucleic acids, activates keratinocyte immune responses
- Epstein-Barr virus - induces IFN response, expresses viral proteins activating SLE susceptibility genes
- Low socioeconomic status, mercury, pesticides, diet
- Gut microbiome - increased gut permeability promotes translocation of gut microbes, contributing to autoantibody development
Innate Immunity Defects
- Neutrophils have higher turnover in SLE, delivering large loads of stimulatory nucleic acids
- Defective macrophage/dendritic cell clearance of cellular debris and immune complexes
- Excess uncleared debris triggers nucleic acid sensors and TLRs in plasmacytoid dendritic cells
- Result: massive upregulation of type I interferon (IFN) - the "IFN signature" central to SLE
Adaptive Immunity Defects
- B cells lose tolerance - expand as "age-associated B cells (ABCs)" that mature into autoantibody-secreting plasma cells
- T follicular and T peripheral helper cells promote B-cell differentiation into high-affinity autoantibody plasma cells
- T regulatory cells are defective - cannot maintain tolerance
- Autoantibodies form immune complexes that deposit in tissues causing inflammation
Autoantibodies in SLE
| Autoantibody | Sensitivity | Specificity | Clinical Association |
|---|---|---|---|
| ANA | >95% | Low | Screening test; almost all SLE patients positive |
| Anti-dsDNA | 70% | 97% | Highly specific; correlates with disease activity and nephritis |
| Anti-Sm (Smith) | 25-30% | 55-100% | Highly specific for SLE |
| Anti-histone | 70% | Low | Drug-induced lupus |
| Antiphospholipid (aPL) | 30-40% | Moderate | Antiphospholipid syndrome (thrombosis, fetal loss) |
| Anti-Ro/SSA | 30-40% | Low | Neonatal lupus, subacute cutaneous lupus, Sjogren overlap |
| Anti-La/SSB | 15-20% | Low | Associated with anti-Ro; neonatal lupus |
| Low C3/C4 | Variable | Moderate | Complement consumption; active disease |
Key rule: ANA sensitivity is >95% (excellent screening), but Anti-dsDNA and Anti-Sm are the most specific antibodies for SLE. - Harrison's 22e; Harriet Lane Handbook
Classification Criteria: 2019 EULAR/ACR
Step 1 - Entry criterion: ANA titer ≥1:80. If absent, do NOT classify as SLE.
Step 2 - Additional weighted criteria (count only the highest criterion per domain):
| Domain | Criterion | Points |
|---|---|---|
| Constitutional | Fever | 2 |
| Neuropsychiatric | Delirium | 2 |
| Psychosis | 3 | |
| Seizure | 5 | |
| Mucocutaneous | Non-scarring alopecia | 2 |
| Oral ulcers | 2 | |
| Subacute cutaneous / discoid lupus | 4 | |
| Acute cutaneous lupus (malar rash) | 6 | |
| Musculoskeletal | Joint involvement | 6 |
| Serosal | Pleural or pericardial effusion | 5 |
| Acute pericarditis | 6 | |
| Hematologic | Leukopenia | 3 |
| Thrombocytopenia | 4 | |
| Autoimmune hemolysis | 4 | |
| Renal | Proteinuria >0.5 g/24h | 4 |
| Renal biopsy class II or V LN | 8 | |
| Renal biopsy class III or IV LN | 10 | |
| Antiphospholipid Ab | Anticardiolipin OR anti-β2GPI OR lupus anticoagulant | 2 |
| Complement | Low C3 OR low C4 | 3 |
| Low C3 AND low C4 | 4 | |
| SLE-specific Ab | Anti-dsDNA | 6 |
| Anti-Sm | 6 |
Classify as SLE if total score ≥ 10 points - Goldman-Cecil Medicine
Note: A renal biopsy showing class III or IV lupus nephritis alone scores 10 points and is sufficient.
Clinical Manifestations
Cutaneous (70-80%)
- Malar (butterfly) rash - erythema over cheeks and nose bridge, sparing nasolabial folds; triggered/worsened by UV
- Discoid lupus - chronic scarring plaques, may cause permanent alopecia
- Subacute cutaneous lupus (SCLE) - annular or papulosquamous lesions, associated with anti-Ro
- Photosensitivity
- Non-scarring alopecia - hair loss/thinning during flares
- Oral/nasal ulcers - usually painless
- Vasculitic lesions - Raynaud's phenomenon, livedo reticularis
Musculoskeletal (90%)
- Arthralgia and non-erosive arthritis - symmetrical, involving small joints (hands, wrists, knees)
- Jaccoud's arthropathy - reversible deformity due to tendon/ligament laxity (not erosive)
- Myalgia, myositis (less common)
- Osteonecrosis (avascular necrosis) - especially with steroid use
Renal (40-75%) - Lupus Nephritis
- One of the most serious manifestations
- WHO/ISN-RPS Classes:
- Class I: Minimal mesangial
- Class II: Mesangial proliferative
- Class III: Focal proliferative (< 50% glomeruli)
- Class IV: Diffuse proliferative (≥ 50% glomeruli) - most severe, worst prognosis
- Class V: Membranous
- Class VI: Advanced sclerosis
- Presents with haematuria, proteinuria, hypertension, nephrotic/nephritic syndrome
Neuropsychiatric (50%)
- Headache, cognitive dysfunction, "brain fog"
- Seizures, psychosis, stroke (often aPL-mediated)
- Peripheral neuropathy, myelitis
Cardiovascular
- Pericarditis (most common cardiac manifestation)
- Myocarditis, endocarditis (Libman-Sacks endocarditis - sterile verrucous vegetations on valve surfaces)
- Accelerated atherosclerosis - major cause of morbidity/mortality in long-term disease
- Raynaud's phenomenon
Pulmonary
- Pleuritis/pleural effusion (most common pulmonary manifestation)
- Pneumonitis, pulmonary hypertension
- "Shrinking lung syndrome" - diaphragmatic dysfunction
Hematologic
- Anemia - often autoimmune hemolytic; also anemia of chronic disease
- Leukopenia (lymphopenia is most characteristic)
- Thrombocytopenia
Antiphospholipid Syndrome (aPL)
- Present in ~30-40% of SLE patients
- Causes: venous/arterial thrombosis, recurrent miscarriage, thrombocytopenia
- Lab: lupus anticoagulant, anticardiolipin Ab, anti-β2GPI Ab
Treatment
Overview: Treat-to-Target Approach
- Goal: remission or lowest possible disease activity to prevent organ damage
- Hydroxychloroquine (HCQ) 5 mg/kg/day is the backbone of therapy for ALL patients unless contraindicated - reduces flares, damage, and mortality
- Minimize glucocorticoid exposure; taper as quickly as possible
Treatment by Severity
Mild disease (cutaneous, arthritis, constitutional):
- NSAIDs (with caution - risk of aseptic meningitis, renal dysfunction)
- HCQ +/- low-dose glucocorticoids
- Methotrexate or azathioprine for steroid-sparing
Moderate-Severe disease (nephritis, CNS, haematologic):
- Glucocorticoids - IV methylprednisolone pulse for severe flares, then oral taper
- Mycophenolate mofetil (MMF) - first-line for lupus nephritis induction and maintenance
- Cyclophosphamide (CYC) - IV; used for severe nephritis (NIH regimen or Euro-lupus low-dose)
- Azathioprine (AZA) - maintenance therapy, safe in pregnancy
- Rituximab (RTX) - anti-CD20; for refractory disease
Biologics
- Belimumab (anti-BLyS/BAFF) - approved for active SLE and lupus nephritis; reduces flares; given as add-on to standard therapy with MMF or low-dose CYC
- Anifrolumab (anti-IFN receptor) - approved for moderate-to-severe SLE; particularly effective for skin disease; NOT recommended for severe neuropsychiatric disease
- Voclosporin (VOC) + MMF - calcineurin inhibitor combination for lupus nephritis
Lupus Nephritis Treatment Algorithm (EULAR 2024):
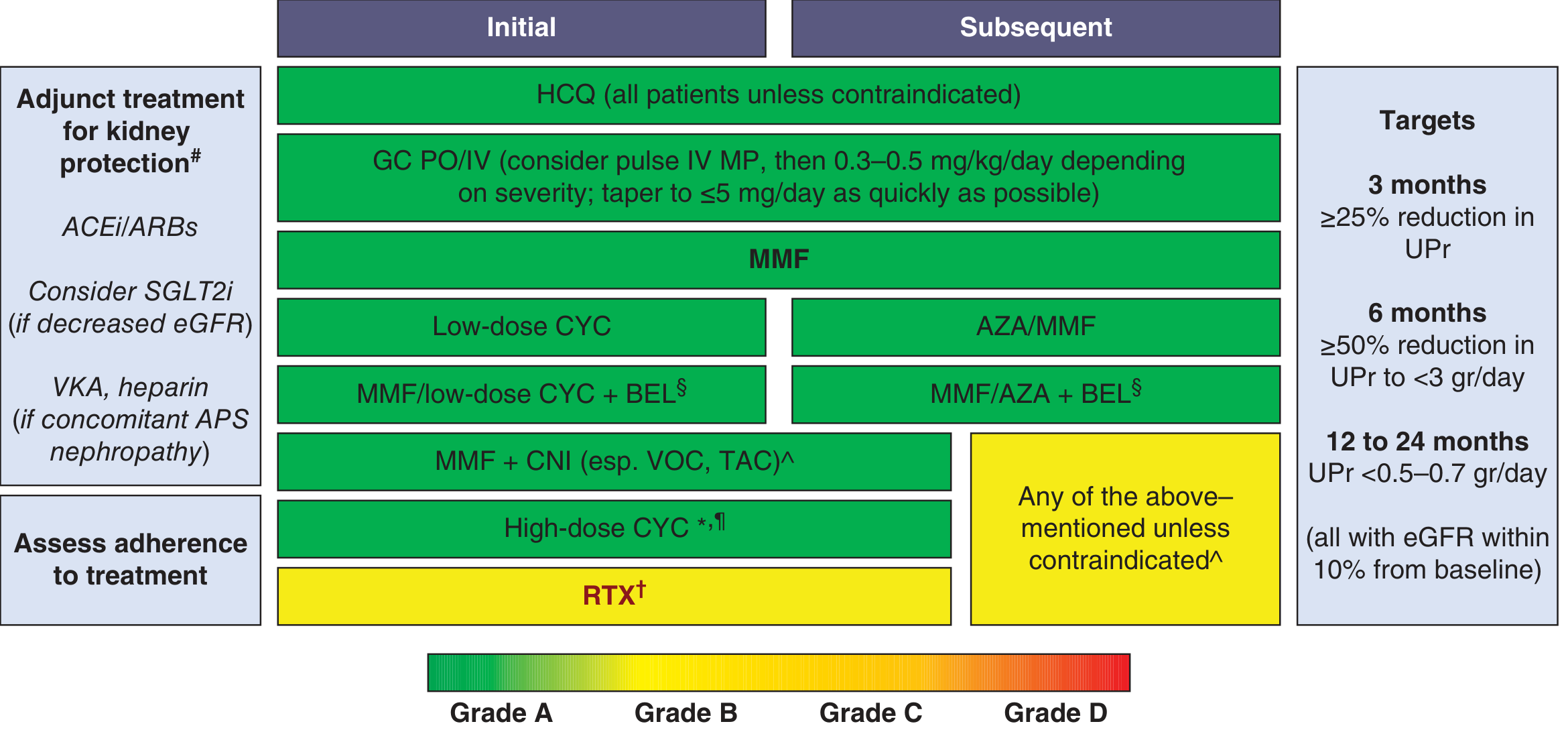
Treatment targets: ≥25% reduction in proteinuria at 3 months; ≥50% reduction to <3 g/day at 6 months; <0.5-0.7 g/day at 12-24 months
Type 1 vs Type 2 Lupus (Harrison's 22e Classification)
| Type 1 SLE | Type 2 SLE | |
|---|---|---|
| Features | Nephritis, arthritis, vasculitis, immune-mediated | Fatigue, diffuse pain, cognitive dysfunction, brain fog, depression |
| Mechanism | Autoimmune inflammation / organ damage | Less clearly autoimmune |
| Response to immunosuppression | Good | Poor |
Prognosis & Monitoring
- Disease activity tracked with SLEDAI (SLE Disease Activity Index) or BILAG scores
- Anti-dsDNA titres and complement (C3/C4) levels correlate with disease activity
- Main causes of death: Infection (especially early), cardiovascular disease (atherosclerosis, especially late), renal failure, CNS disease
- Accelerated atherosclerosis is a major late complication; annual cardiovascular risk assessment recommended
- Blood for alcohol: serum fluoride/oxalate preserved; avoid spirit for skin cleaning (to prevent false-positive alcohol results - from forensic context this time, about SLE, not alcohol!)
Sources:
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - primary reference
- Goldman-Cecil Medicine, International Edition - classification criteria, pathobiology
- Harriet Lane Handbook, 23rd ed. - autoantibody specificity/sensitivity
This is a shared conversation. Sign in to Orris to start your own chat.