BP 170/90 how to low
Reading File
Searching the Web
how to lower blood pressure 170/90 hypertension treatment 2025
Finding Sources
Searching PubMed
"hypertension" AND "treatment" AND "lifestyle"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a thorough, evidence-based answer:
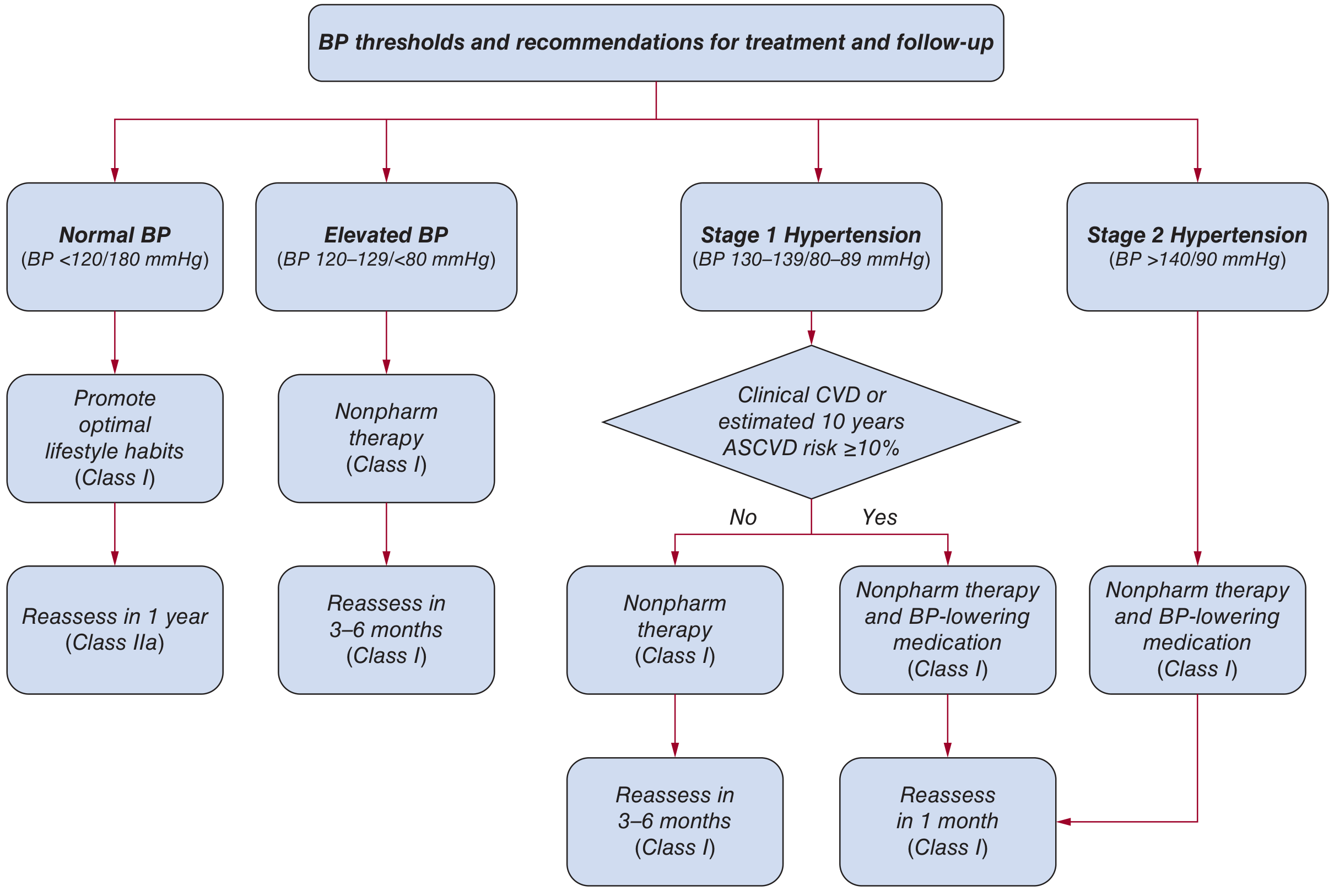
Blood Pressure 170/90 mmHg - How to Lower It
A reading of 170/90 mmHg qualifies as Stage 2 Hypertension (BP >140/90). At this level, guidelines are clear: you need both lifestyle changes AND medication - started together, not sequentially.
1. Lifestyle Changes (Non-drug - Start Immediately)
These are not optional - each intervention has a measurable impact on systolic BP (SBP):
| Intervention | How to Do It | Expected SBP Drop |
|---|---|---|
| Weight loss | ~1 mmHg drop per 1 kg lost | up to -5 mmHg |
| DASH diet | Rich in fruits, vegetables, low-fat dairy; less saturated fat | -4 to -11 mmHg |
| Reduce sodium | Target <1,500 mg/day; avoid processed foods, canned soups, fast food | -5 to -6 mmHg |
| Increase potassium | More fruits and vegetables (bananas, leafy greens, potatoes) | -4 to -5 mmHg |
| Exercise | 90-150 min/week of aerobic activity (brisk walking, swimming, cycling); aim for 65-75% of max heart rate | -5 to -8 mmHg |
| Limit alcohol | Men: ≤2 drinks/day; Women: ≤1 drink/day | -4 mmHg |
| Quit smoking | For overall cardiovascular risk reduction (not a direct BP effect, but critical for heart health) | - |
Sources: Fuster and Hurst's The Heart, 15th Ed.; National Kidney Foundation Primer on Kidney Diseases, 8th Ed.
2. Medication (Required at This BP Level)
At 170/90, your BP is more than 20/10 mmHg above the target of 130/80, which means you almost certainly need two medications, ideally in a single combination pill.
Best evidence for first-line combinations:
- ACE inhibitor + Calcium Channel Blocker (amlodipine) - strongest evidence from the ACCOMPLISH trial
- ACE inhibitor + Thiazide diuretic - acceptable alternative
- If you can't tolerate ACE inhibitors, substitute an ARB (e.g., losartan, valsartan)
Special situations:
- Diabetes or kidney disease: ACE inhibitor or ARB is preferred (kidney-protective)
- Heart failure or post-MI: Beta-blocker + ACE inhibitor/ARB
- Black adults: Thiazide diuretic or CCB tend to be more effective first-line
- Do NOT combine two renin-angiotensin blockers (e.g., ACE inhibitor + ARB together) - contraindicated
Reassessment: At Stage 2, recheck BP within 1 month of starting treatment.
3. What the 2025 ACC/AHA Guideline Adds
The 2025 ACC/AHA hypertension guideline (updated from 2017) reinforces:
- Treatment goal: <130/80 mmHg for all adults
- Anyone with BP ≥140/90 should start medication alongside lifestyle changes
- For Stage 2, starting with a single-pill combination of two drugs is preferred for better adherence
- Risk stratification using the PREVENT calculator helps personalize care
4. Common Reasons BP Stays High Despite Treatment
If BP is not coming down:
- Non-adherence - up to 50% of patients miss doses; once-daily combination pills help significantly
- Too much sodium - the most common dietary culprit
- Inadequate drug dose - "therapeutic inertia" (under-dosing) is very common
- White coat hypertension - confirm with home readings
- Secondary causes - kidney disease, sleep apnea, aldosterone excess (consider if BP resists 3+ drugs)
Important: See a doctor promptly. A BP of 170/90 carries real risk for stroke, heart attack, and kidney damage. Medication at this level is not optional - lifestyle alone is unlikely to bring you to goal. If you have chest pain, severe headache, vision changes, or shortness of breath, seek emergency care immediately (hypertensive urgency/emergency).
This is a shared conversation. Sign in to Orris to start your own chat.