Myocarditis deseases basic to advance clinical explain kro
Reading File
Finding Sources
Searching PubMed
myocarditis diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a thorough, well-structured answer. Let me compile the complete clinical overview:
Myocarditis - Basic to Advanced Clinical Overview
1. Definition
Myocarditis is an inflammatory process involving the myocardium (heart muscle), characterized histologically by myocyte injury (degeneration or necrosis) with an inflammatory cellular infiltrate - not due to ischemia. It encompasses a diverse group of clinical entities triggered by infectious agents, immune-mediated processes, or toxins.
It is important to distinguish myocarditis from conditions like ischemic heart disease, where inflammation is secondary to another cause of myocardial injury.
- Goldman-Cecil Medicine, p. 511
- Robbins & Kumar Basic Pathology, p. 375
2. Epidemiology
- Incidence and prevalence are hard to estimate due to variable presentation (often subclinical)
- Population estimates: 1 in 100,000 to 1 in 10,000
- Postmortem studies: myocarditis found in up to 12% of young victims of sudden cardiac death
- More common in young adults and males
- May also be the inflammatory phase of arrhythmogenic cardiomyopathy
3. Etiology - Causes (Complete Classification)
A. Infectious Causes
| Category | Examples |
|---|---|
| Viral (most common in Western world) | Coxsackievirus A & B (most common), Enteroviruses, Adenovirus, Parvovirus B19, HHV-6, CMV, HIV, Influenza, SARS-CoV-2, Hepatitis C, RSV |
| Protozoal (most common worldwide) | Trypanosoma cruzi (Chagas disease), Toxoplasma gondii |
| Bacterial | Corynebacterium diphtheriae, Mycoplasma pneumoniae, Staphylococcus, Neisseria meningitidis, Mycobacterium, Brucella |
| Spirochetal | Borrelia burgdorferi (Lyme disease), Treponema pallidum, Leptospira |
| Fungal | Aspergillus, Candida, Cryptococcus, Histoplasma |
| Rickettsial | Rickettsia rickettsii, Coxiella burnetii |
| Parasitic | Trichinella spiralis, Echinococcus, Taenia solium |
B. Immune-Mediated Causes
- Autoantigens: SLE, polymyositis/dermatomyositis, systemic sclerosis, EGPA
- Alloantigens: Heart transplant rejection
- Allergen (drug hypersensitivity): Penicillin, sulfonamides, methyldopa, tetracycline, thiazides, tricyclic antidepressants
C. Toxic Causes
- Drugs: Anthracyclines, cocaine, amphetamines, cyclophosphamide, 5-FU, trastuzumab, checkpoint inhibitors (increasingly recognized), clozapine
- Physical agents: Electric shock, radiation, hyperpyrexia
- Heavy metals: Copper, iron, lead
- Others: Arsenic, snake bite, scorpion venom, carbon monoxide
D. Special Cases
-
mRNA COVID-19 vaccine myocarditis: Rare, especially in male adolescents/young adults after the 2nd dose, usually within 1 week - most recover uneventfully
-
Giant cell myocarditis (GCM): Rare, fulminant, aggressive - requires early immunosuppression
-
Eosinophilic myocarditis: Drug hypersensitivity or hypereosinophilic syndrome
-
Goldman-Cecil Medicine, Table 47-3, p. 510-511
-
Robbins & Kumar Basic Pathology, p. 375
4. Pathogenesis
Phase 1 - Direct Viral Invasion (Days 1-4)
Cardiotropic viruses enter cardiomyocytes via receptor-mediated endocytosis (e.g., Coxsackievirus binds CAR receptor). The viral genome is translated intracellularly and may contribute to myocyte dysfunction by cleaving dystrophin (a cytoskeletal protein).
Phase 2 - Innate Immune Activation (Days 4-14)
Natural killer (NK) cells and macrophages are recruited; proinflammatory cytokines (IL-1, TNF-alpha) are released. This phase can eliminate the virus but also injures cardiomyocytes.
Phase 3 - Adaptive Immune Response / Autoimmunity (Weeks onwards)
- Activation of CD4+ T lymphocytes promotes clonal expansion of B lymphocytes
- Circulating anti-heart antibodies are produced (against myosin heavy chain, adenine nucleotide translocator, beta-1 adrenoceptors, contractile and mitochondrial proteins)
- Molecular mimicry: Viral antigens cross-react with myocardial proteins
- This autoimmune response leads to long-term ventricular remodeling and extracellular matrix changes
Why Some Progress to Dilated Cardiomyopathy (DCM)?
Three proposed mechanisms:
- Immunopathogenic hypothesis - Abnormal immune response "smolders" into subacute/chronic phase
- Viral persistence - Virus persists in myocardium and drives ongoing inflammation
- Combined mechanisms - Both viral persistence + autoimmunity + possible genetic susceptibility
- Goldman-Cecil Medicine, p. 511
- Fuster & Hurst's The Heart 15e, p. (ch. 55)
5. Histopathology (Morphology)
Dallas Criteria (1986) - Still Referenced
Four patterns recognized on endomyocardial biopsy (EMB):
| Pattern | Definition |
|---|---|
| Active myocarditis | Myocyte degeneration/necrosis + definite cellular infiltrate ± fibrosis |
| Borderline myocarditis | Definite cellular infiltrate WITHOUT myocyte injury |
| Persistent myocarditis | Continued active myocarditis on repeat biopsy |
| Resolving/Resolved myocarditis | Diminished/absent infiltrate with connective tissue healing |
Limitation: Dallas criteria have low specificity and sensitivity - diagnostic yield as low as 10-20% in some series.
Microscopic Appearance (Viral)
- Myocardium: edema, interstitial inflammatory infiltrates, myocyte injury
- Diffuse lymphocytic infiltrate is most common
- In acute phase: heart appears normal or dilated, may be flabby and mottled with pale/hemorrhagic areas
- Mural thrombi may be present
Giant Cell Myocarditis (Special)
- Multinucleated giant cells + eosinophils + lymphocytes
- Indicates aggressive disease with poor prognosis
Eosinophilic (Hypersensitivity) Myocarditis
-
Eosinophil-rich infiltrate
-
Often drug-related; typically mild but rarely causes CHF or sudden death
-
Robbins & Kumar Basic Pathology, p. 375
-
Goldman-Cecil Medicine, p. 511
6. Clinical Presentations
Myocarditis has an extremely variable clinical spectrum:
A. Asymptomatic / Subclinical
- Most common form
- Manifests only as transient ECG abnormalities (nonspecific ST-T changes)
- Discovered incidentally
B. Myopericarditis (Chest Pain Syndrome)
- Prodrome: Fever, myalgia, coryza, gastroenteritis (viral illness 1-2 weeks prior)
- Chest pain - sharp, pleuritic, mimics ACS (but coronaries are normal!)
- Mildly elevated troponin
- Usually good prognosis if LV function preserved
- ~15% may develop recurrent myopericarditis
C. New-Onset Heart Failure / Dilated Cardiomyopathy
- Exertional dyspnea, fatigue, orthopnea, PND
- Signs of LV failure
- Most common presentation requiring hospitalization
D. Acute/Fulminant Myocarditis
- Cardiogenic shock with acute cardiovascular collapse
- Rapid hemodynamic compromise
- May require mechanical circulatory support
- Paradoxically, can have better long-term prognosis than subacute forms if patient survives the acute phase
E. Arrhythmia Presentation
- Palpitations, syncope, sudden cardiac death (sometimes the first presentation)
- PVCs, NSVT, accelerated idioventricular rhythm, polymorphic VT
- In lymphocytic myocarditis: PVCs often originate from inferior LV (RBBB + superior axis morphology)
- AV block (especially in Lyme disease - self-limited, may need temporary pacing)
- Ventricular arrhythmias persist even after apparent healing due to residual scar (late gadolinium enhancement substrate)
F. Autoimmune Rheumatic Disease Associated
-
SLE: Most common symptom = exertional dyspnea; ECG shows sinus tachycardia, ST-T changes; troponin I may rise markedly
-
Polymyositis/Dermatomyositis, SSc, EGPA: Also recognized associations
-
May be initial feature of underlying rheumatic disease
-
Goldman-Cecil Medicine, p. 512
-
Grainger & Allison Diagnostic Radiology, p. 330-331
-
Braunwald's Heart Disease, ch. 55
7. Diagnosis
High index of suspicion is required - myocarditis can mimic many common conditions.
Step 1: History & Physical
- Recent viral illness + new cardiac symptoms = high suspicion
- Physical exam: tachycardia, S3 gallop, signs of heart failure, friction rub (if pericarditis)
Step 2: Laboratory Tests
| Test | Findings |
|---|---|
| Troponin T/I | Elevated (may be absent even in biopsy-proven cases) |
| BNP/NT-proBNP | Elevated if HF present |
| CBC | Leukocytosis (especially eosinophilia in drug reactions) |
| ESR/CRP | Elevated (nonspecific) |
| Viral serology | Rising antibody titers (coxsackievirus, etc.) |
| ANA, anti-dsDNA, complement C3/C4 | If autoimmune cause suspected (SLE) |
| Myositis immunoblot screen | If polymyositis/dermatomyositis suspected |
| Anti-cardiac autoantibodies | Anti-myosin, anti-adenine nucleotide translocator - biomarkers of autoimmune myocarditis |
| miRNA | has-miR-Chr8:96 - seen in myocarditis, rarely in MI (emerging biomarker) |
Step 3: ECG
- Most common: sinus tachycardia
- Nonspecific ST-T wave changes
- Pathologic Q waves
- Low QRS voltages
- AV block (Lyme)
- SVT / VT / PVCs
Step 4: Echocardiography
No pathognomonic features, but may reveal:
- Impaired LV or RV systolic function (with or without dilation)
- Regional wall motion abnormalities
- LV thrombus
- Diastolic impairment
- Pericardial effusion
Step 5: Cardiac MRI (CMR) - Key Non-Invasive Tool
Lake Louise Criteria - CMR diagnosis based on:
- T2-weighted imaging - myocardial edema (T2 signal ratio >2.0)
- Early gadolinium enhancement (EGE) - hyperemia/capillary leak (global EGE ratio >4.0)
- Late gadolinium enhancement (LGE) - necrosis/fibrosis
Classic Pattern: Subepicardial LGE in the lateral and/or inferior wall - in a non-ischemic distribution (distinguishes from MI where LGE is subendocardial or transmural). In Takotsubo CMP, LGE is typically absent.
A negative LGE does NOT exclude myocarditis - early enhancement (EGE) should be assessed when macroscopic necrosis is absent.
CMR also detects:
- Coronary microvascular dysfunction (adenosine stress first-pass perfusion)
- Myocardial fibrosis for arrhythmic risk stratification
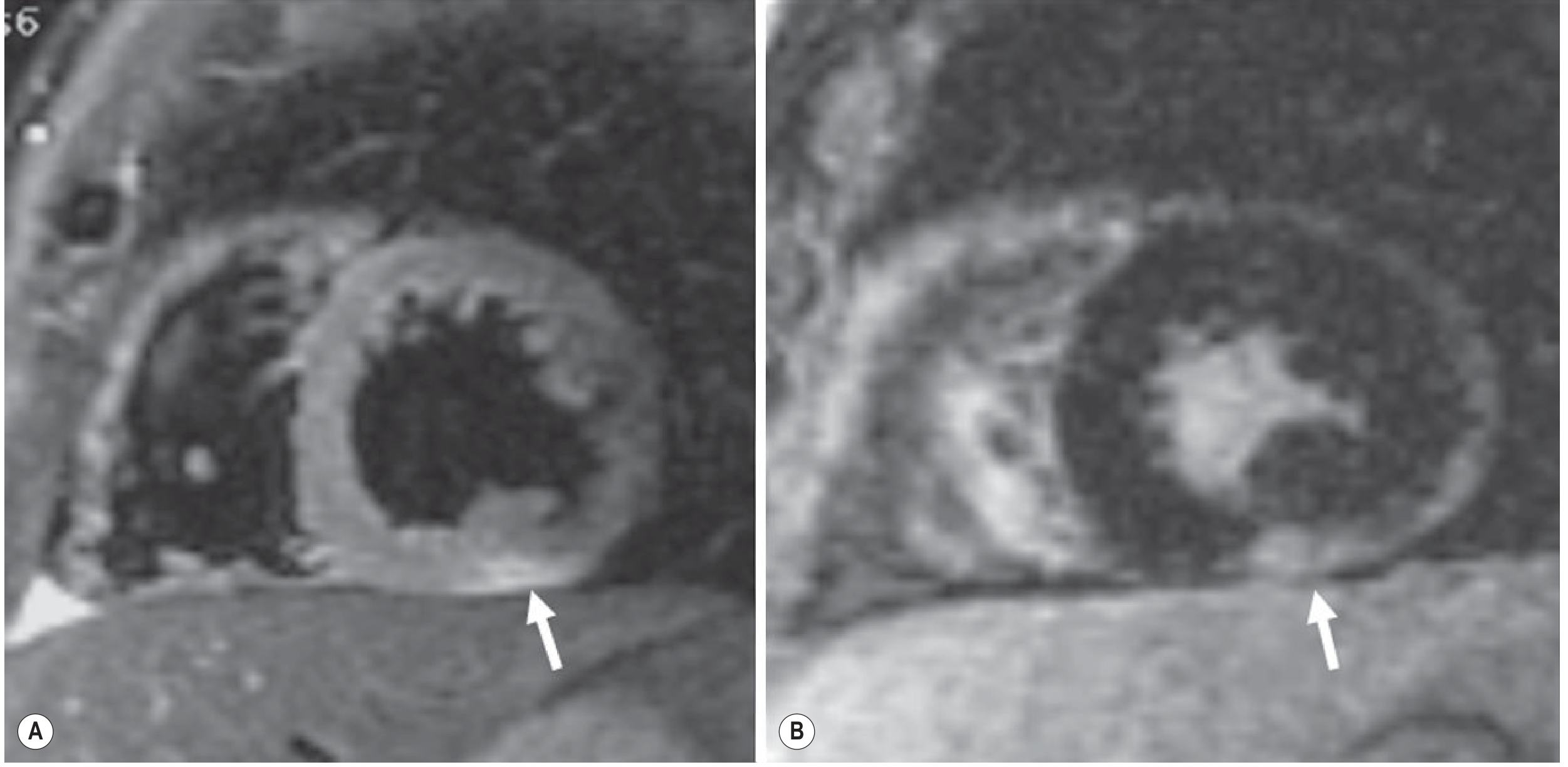
Fig: Acute Myocarditis CMR. (A) T2 STIR: subepicardial edema (arrow) inferior wall. (B) LGE: non-ischemic pattern. - Grainger & Allison Diagnostic Radiology
Step 6: Endomyocardial Biopsy (EMB) - Gold Standard
Still the definitive test, but reserved for specific indications due to sampling error and low sensitivity.
AHA/ACC Indications for EMB:
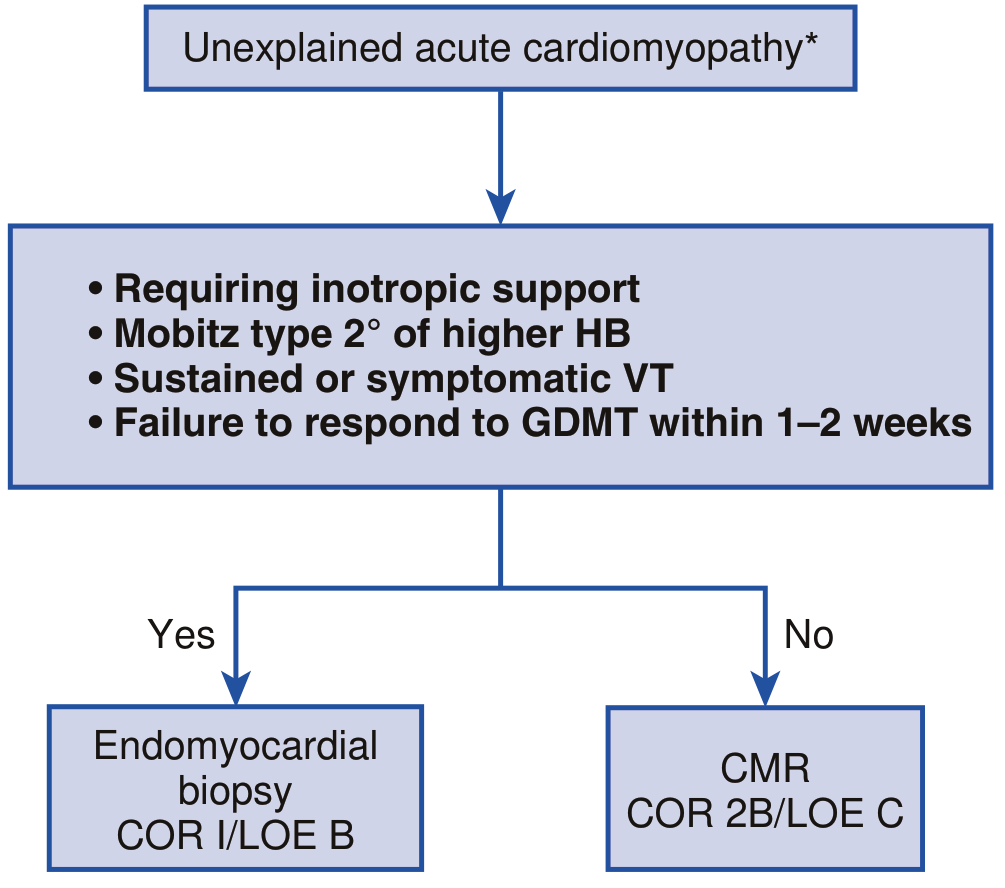
EMB is indicated (Class I) when:
- Requiring inotropic support
- Mobitz type 2° or higher heart block
- Sustained or symptomatic VT
- Failure to respond to guideline-directed medical therapy (GDMT) within 1-2 weeks
- Features suggesting systemic disease (amyloidosis, sarcoidosis, hemochromatosis)
Modern EMB analysis uses:
-
Conventional H&E + Dallas criteria
-
Immunohistochemistry - subtypes of infiltrating lymphocytes, abnormal cellular adhesion molecule expression
-
PCR/RT-PCR on extracted RNA/DNA - for viral genome detection
-
Immunofluorescence - immune complex deposition (in SLE)
-
Goldman-Cecil Medicine, p. 512
-
Grainger & Allison Diagnostic Radiology, p. 331
-
Braunwald's Heart Disease, Figure 55.7
8. Special Subtypes
Giant Cell Myocarditis (GCM)
- Rare, idiopathic, often associated with autoimmune diseases and thymoma
- Fulminant course - high mortality without treatment
- Histology: multinucleated giant cells, diffuse inflammation with eosinophils
- Requires combined immunosuppression (cyclosporine + steroids ± azathioprine)
- May need transplantation; disease can recur in transplanted heart
Chagas Disease (Trypanosoma cruzi)
- Most common infective myocarditis worldwide (~6 million infected in Latin America)
- ~300,000 infected in USA (immigration)
- Acute phase: Sometimes causes severe myocarditis, 10% die; often unrecognized
- Chronic phase (10-20 years later): Progressive CHF, RBBB + left anterior hemiblock, PVCs, apical aneurysm, VT, sudden death
- VT mechanism: scar-related reentry from inferolateral LV (RBBB + right axis morphology)
Lyme Myocarditis
- Occurs in ~5% of Lyme disease patients
- Primarily manifests as self-limited conduction system disease (AV block)
- Frequently requires temporary pacemaker
Immune Checkpoint Inhibitor (ICI) Myocarditis
- Increasingly recognized with cancer immunotherapy (PD-1/PD-L1/CTLA-4 inhibitors)
- Fulminant presentation common; high mortality (~40-50%)
- Requires immediate immunosuppression with high-dose corticosteroids + stopping ICI
COVID-19 / Post-mRNA Vaccine Myocarditis
- Vaccine: predominantly males <30 years, after 2nd dose, within 7 days
- Most resolve uneventfully with conservative management
- SARS-CoV-2 infection itself also causes lymphocytic myocarditis
9. Management
A. General Supportive Care (All Patients)
-
Bed rest - restrict strenuous physical activity for at least 3-6 months (competitive sports contraindicated)
-
Heart failure guideline-directed medical therapy (GDMT):
- ACE inhibitor / ARB - for LV dysfunction
- Beta-blockers - for HF with reduced EF
- Diuretics - for volume overload / congestion
- MRA (spironolactone/eplerenone) - if EF <35%
-
NSAIDs - useful for pericarditic chest pain; colchicine as adjunct
- Note: NSAIDs may worsen myocarditis in experimental models - use cautiously in pure myocarditis
-
Anticoagulation - if LV thrombus, AF, or severe LV dysfunction (EF <30%)
B. Hemodynamic Support (Fulminant)
- Vasopressors/inotropes - norepinephrine, dobutamine
- Intra-aortic balloon pump (IABP)
- Ventricular assist devices (VADs) - temporary (Impella, TandemHeart, ECMO)
- Permanent VAD as bridge to recovery or transplantation
C. Immunosuppressive Therapy
This is the most debated area. Current evidence:
| Situation | Recommendation |
|---|---|
| Routine acute viral myocarditis | NOT recommended (Myocarditis Treatment Trial showed no benefit) |
| Giant cell myocarditis | STRONGLY indicated - cyclosporine + prednisone ± azathioprine |
| Autoimmune (virus-negative) myocarditis | Beneficial - prednisone + azathioprine (anti-cardiac antibodies present, no viral genome) |
| SLE/PM-DM myocarditis | Effective immunosuppression improves outcomes |
| Eosinophilic/Hypersensitivity | Discontinue offending drug + corticosteroids |
| ICI-associated myocarditis | High-dose IV methylprednisolone + stop ICI |
| Sarcoid myocarditis | Corticosteroids |
Key trial: Myocarditis Treatment Trial (MTT) - 111 biopsy-proven patients randomized to prednisone + azathioprine or cyclosporine vs placebo. Both groups improved LVEF by ~9% - immunosuppression offered no additional benefit in unselected patients. This underscores the need to identify virus-negative, autoimmune subgroups first.
D. Antiviral Therapy
- No proven benefit currently for viral myocarditis in clinical trials
- Theoretical basis: if viral persistence drives inflammation, antivirals could help
- HIV myocarditis: highly active antiretroviral therapy (HAART)
E. Arrhythmia Management
- PVCs/NSVT: beta-blockers; antiarrhythmic drugs if needed
- AV block: temporary pacing (Lyme resolves spontaneously)
- ICD: Consider for:
- Sustained VT + depressed LV function
- LGE on CMR (arrhythmic risk marker)
- Inducible VT on EP testing
- Catheter ablation for recurrent VT: Challenging due to varied scar locations; recurrence rates >50%
F. Cardiac Transplantation
- Last resort for refractory end-stage heart failure
- Note: GCM can recur in the transplanted heart
10. Prognosis
| Clinical Scenario | Prognosis |
|---|---|
| Myopericarditis + preserved LV function | Excellent - most recover fully |
| Acute/fulminant myocarditis | Paradoxically better long-term survival if acute phase survived |
| Acute DCM from myocarditis | Intermediate - ~15% risk of death/transplantation |
| Giant cell myocarditis | Poor without aggressive immunosuppression |
| Children with acute myocarditis | LV recovery extends up to 8 years; ~30% risk death/transplant |
| DCM with LGE on CMR | Higher arrhythmic event risk |
| Persistent viral genomes on EMB | Associated with poorer outcome |
| Anti-cardiac autoantibodies present | May predict response to immunosuppression |
Long-term risk: Even after apparent clinical resolution, patients face risk of late HF due to diastolic dysfunction years later.
11. Summary Flow - Diagnostic Approach
Young patient + chest pain / HF / arrhythmia / prodromal viral illness
↓
ECG + Troponin + Echo
↓
Exclude ACS (coronary angiography if needed - normal coronaries in myocarditis)
↓
Cardiac MRI (Lake Louise Criteria)
↓
If hemodynamically unstable / no GDMT response / high-grade AV block / VT
↓
Endomyocardial Biopsy → Dallas criteria + Immunohistochemistry + PCR
↓
Subtype-directed treatment
Sources
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine (Braunwald's)
- Goldman-Cecil Medicine International Edition (Goldman-Cecil)
- Robbins & Kumar Basic Pathology 10e (Robbins)
- Grainger & Allison's Diagnostic Radiology
- Fuster & Hurst's The Heart, 15th Edition
- Firestein & Kelley's Textbook of Rheumatology
This is a shared conversation. Sign in to Orris to start your own chat.