Make notes on SA NODE block and AV NODE Block in detail, all the type , add ecg with labeling (multiple different different examples of ecg)
Reading File
Finding Sources
Finding Sources
Searching the Web
SA node sinoatrial block types ECG examples labeled
Finding Sources
Finding Sources
Searching the Web
AV block types ECG examples labeled first second third degree Wenckebach Mobitz
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed. Let me compile the comprehensive notes.
SA NODE BLOCK & AV NODE BLOCK - Detailed Notes
PART 1: SA NODE (SINOATRIAL) BLOCK
Anatomy & Physiology Background
The SA node sits at the subepicardial surface at the junction of the right atrium and superior vena cava. It contains two cell types:
- P cells (pacemaker cells) - generate the electrical impulse
- T cells (transitional cells) - transmit the impulse outward to atrial myocardium
In SA block, the impulse is either generated normally but fails to exit (exit block), or generation itself fails (sinus arrest). The critical distinction: the SA node depolarization is NOT visible on surface ECG - only the resulting P wave is visible. So SA block is inferred from P wave patterns alone.
Sinoatrial exit block results from failure of sinus node activity to propagate to the atrium. - Harrison's Principles of Internal Medicine 22E
Causes of SA Node Block
| Category | Examples |
|---|---|
| Ischemia | SA nodal artery occlusion (branch of RCA), inferior MI |
| Fibrosis / Degeneration | Sick sinus syndrome, age-related fibrosis |
| Inflammation | Myocarditis, endocarditis, rheumatic fever |
| Medications | Digitalis, beta-blockers, calcium channel blockers, antiarrhythmics |
| Vagal tone | Well-trained athletes, carotid sinus hypersensitivity |
| Infiltrative disease | Amyloidosis, sarcoidosis |
Types of SA Node Block
SA block is classified analogously to AV block, but only 2nd degree can be diagnosed on the surface ECG. First and third degree require invasive electrophysiology study.
TYPE 1: FIRST-DEGREE SA BLOCK
Mechanism: Fixed delay between SA node firing and atrial depolarization (prolonged SA conduction time), but every impulse eventually reaches the atrium.
ECG: CANNOT be seen on surface ECG. Requires an intracardiac electrophysiology study (EPS) placing a wire near the SA node to record SA node electrogram and measure SA conduction time (SACT).
Clinical significance: Benign. Usually asymptomatic.
TYPE 2: SECOND-DEGREE SA BLOCK - TYPE I (Sinoatrial Wenckebach)
Mechanism: Progressive increase in SA conduction time with each beat until one impulse fails to exit - no P wave (and no QRS) appears. Then the cycle resets.
ECG Key Features:
- P-P interval progressively shortens (because the increment of delay decreases each beat - the same mechanism as R-R shortening in AV Wenckebach)
- Followed by a pause (dropped P + QRS)
- The pause is less than twice the shortest P-P interval
- "Grouped beating" pattern (clusters of beats)
ECG Example - SA Wenckebach (Type I) with ladder diagram:
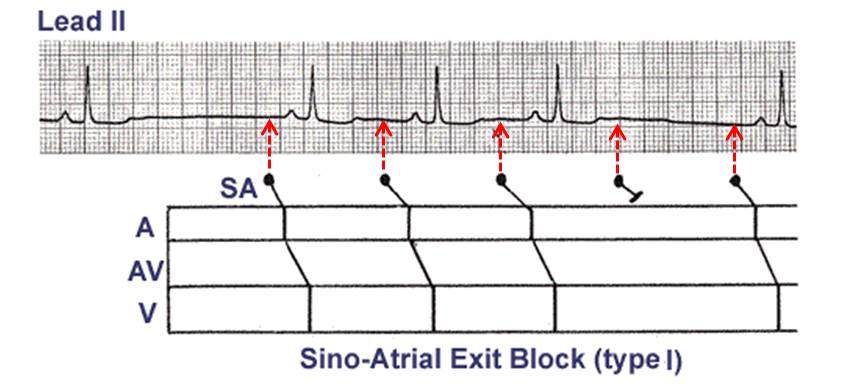
The P-P intervals progressively shorten before the pause. The ladder diagram shows the SA node fires regularly but with increasing conduction delay until one beat is blocked.
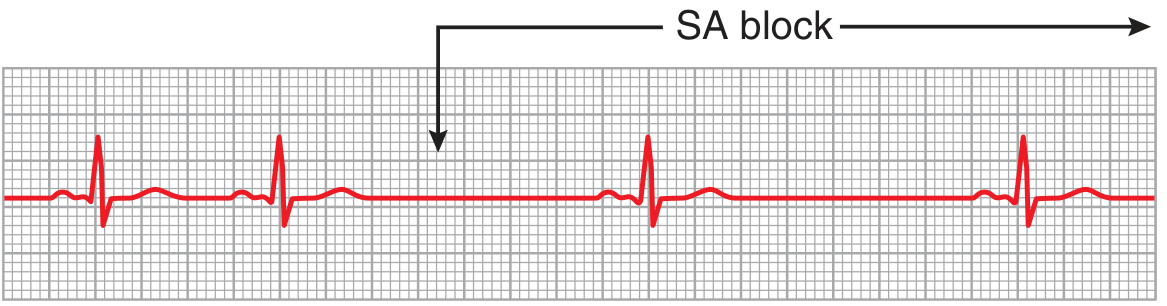
TYPE 3: SECOND-DEGREE SA BLOCK - TYPE II (Mobitz II)
Mechanism: Fixed SA conduction time with sudden intermittent failure of propagation. Every other impulse (or every 3rd, etc.) fails to exit.
ECG Key Features:
- P-P intervals remain constant before the dropped beat
- The pause is exactly (or approximately) twice the normal P-P interval
- Abrupt transition to a sinus rate that is half the previous rate (2:1 SA block)
- No gradual shortening of P-P intervals before the pause
Type II second-degree SA block can be inferred on the ECG if the sinus rate abruptly transitions to a sinus rate that is half the previous rate. - Harrison's 22E
ECG Key:
- Constant P-P intervals → sudden pause = 2x P-P = Type II SA block
- Mimics sinus pause but the pause is a mathematically exact multiple of the P-P
TYPE 4: THIRD-DEGREE (COMPLETE) SA BLOCK
Mechanism: No impulses exit the SA node at all. The atria are depolarized by a subsidiary pacemaker (junctional or ventricular escape).
ECG:
- No visible P waves from SA node
- Escape rhythm appears (junctional at 40-60 bpm, or ventricular at 20-40 bpm)
- Cannot be distinguished from sinus arrest on surface ECG - requires EPS
ECG from Guyton & Hall - SA Block with AV Nodal Escape:
After the SA block begins, P waves disappear. Ventricles establish their own rhythm via the AV node. The escape QRS complexes are narrow and slower.
SA Block vs. Sinus Arrest - Key Distinction
| Feature | SA Exit Block (Type II) | Sinus Arrest |
|---|---|---|
| Mechanism | Impulse generated, fails to exit | SA node stops firing |
| Pause duration | Exact multiple of P-P interval | NOT a multiple of P-P |
| P-P before pause | Constant (Type II) or shortening (Type I) | Variable |
| Distinguishable on ECG? | Yes (Type II by math) | Yes (by exclusion) |
Sinoatrial Exit Block ECG from Harrison's 22E:
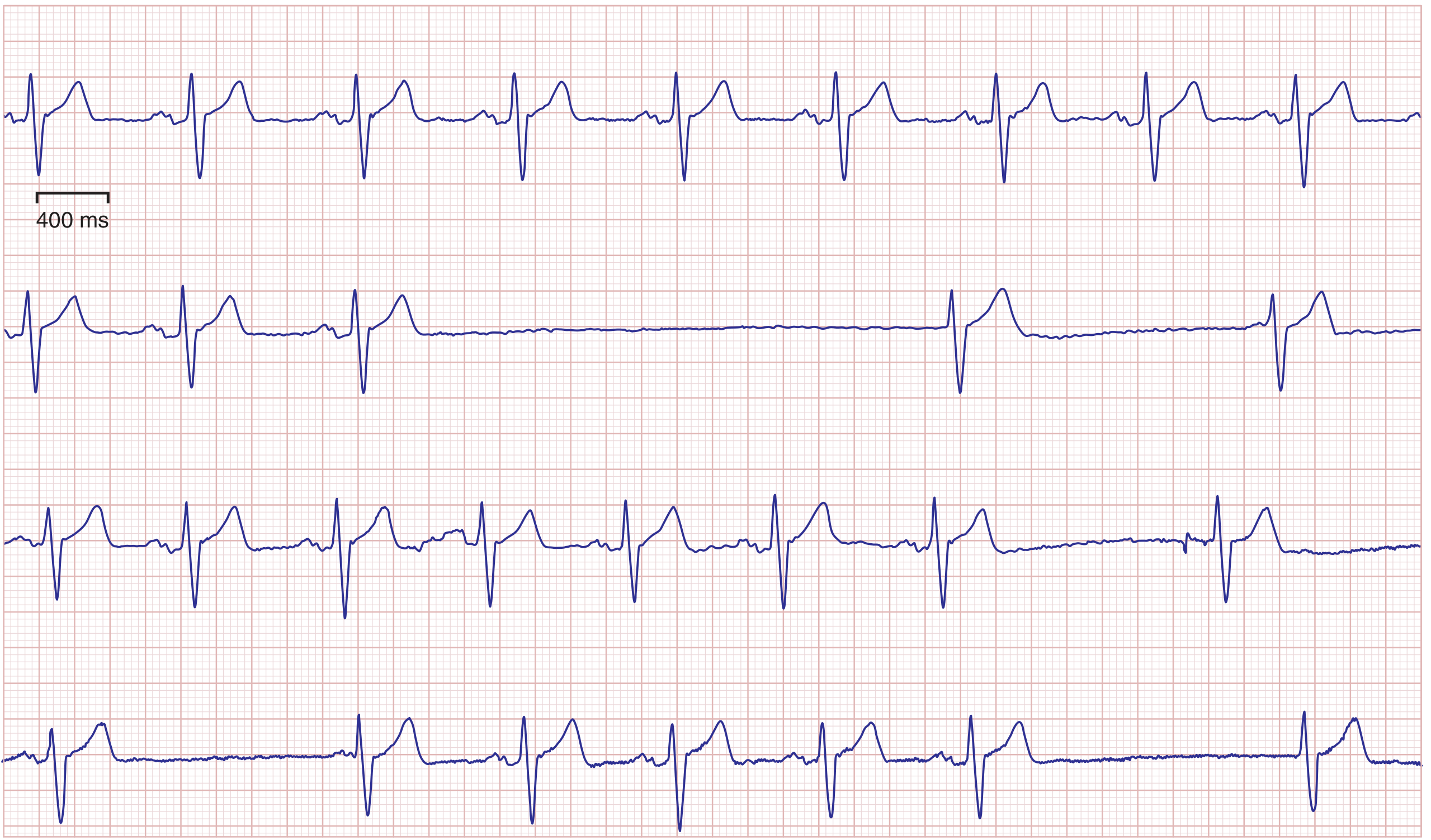
Line 2 shows a long pause with absent P wave and absent QRS, followed by a junctional escape beat, then gradual return of sinus rhythm P waves.
SA Block - Management
| Type | Management |
|---|---|
| 1st degree | No treatment needed |
| 2nd degree (asymptomatic) | Identify + remove reversible causes (medications, hypothyroidism, electrolytes) |
| 2nd degree (symptomatic) | Atropine, pacemaker consideration |
| 3rd degree | Permanent pacemaker if no reversible cause |
| Tachy-Brady syndrome | Often requires pacemaker (allows safe use of rate-control agents) |
PART 2: AV NODE BLOCK (ATRIOVENTRICULAR BLOCK)
Anatomy
Impulses travel from SA node → atrial myocardium → AV node (inferior right atrium) → Bundle of His → Right & Left bundle branches → Purkinje fibers → ventricular myocardium.
The AV node is the only normal electrical connection between atria and ventricles. Block at any level of this pathway = AV block.
Causes of AV Block
From Guyton & Hall:
- Ischemia of AV node or bundle of His (RCA occlusion most common)
- Compression by scar tissue or calcified cardiac structures
- Inflammation - rheumatic fever, diphtheria, endocarditis, myocarditis
- Excessive vagal tone - carotid sinus syndrome, trained athletes
- Degeneration - age-related fibrosis (Lev's disease, Lenègre's disease)
- Medications - digitalis, beta-blockers, calcium channel blockers
CLASSIFICATION OF AV BLOCK
FIRST-DEGREE AV BLOCK
Mechanism: Slowed conduction through AV node. Every atrial impulse reaches the ventricles, but with delay. NOT a true block - all impulses conduct.
ECG Criteria:
- PR interval > 200 ms (>0.20 sec) on every beat
- Every P wave is followed by a QRS complex
- QRS morphology is normal (narrow unless BBB coexists)
- Regular rhythm
Normal PR = 0.12-0.20 sec | 1st degree = >0.20 sec
ECG - First-Degree AV Block (Guyton & Hall, Fig 13.5):
PR interval is approximately 0.30 sec (normal ≤0.20 sec). Each P wave conducts to a QRS. Rhythm is regular.
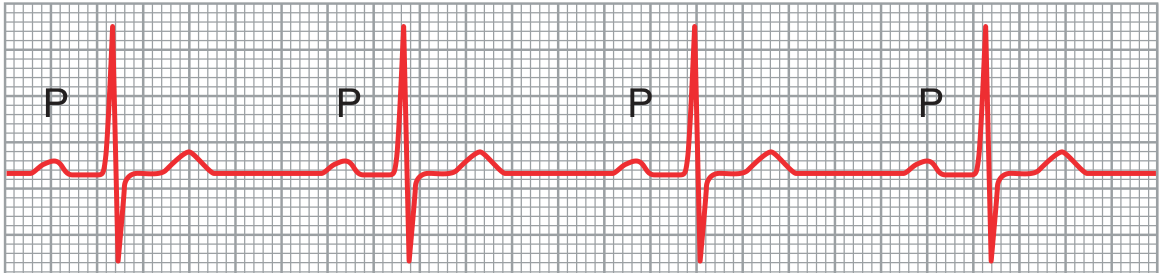
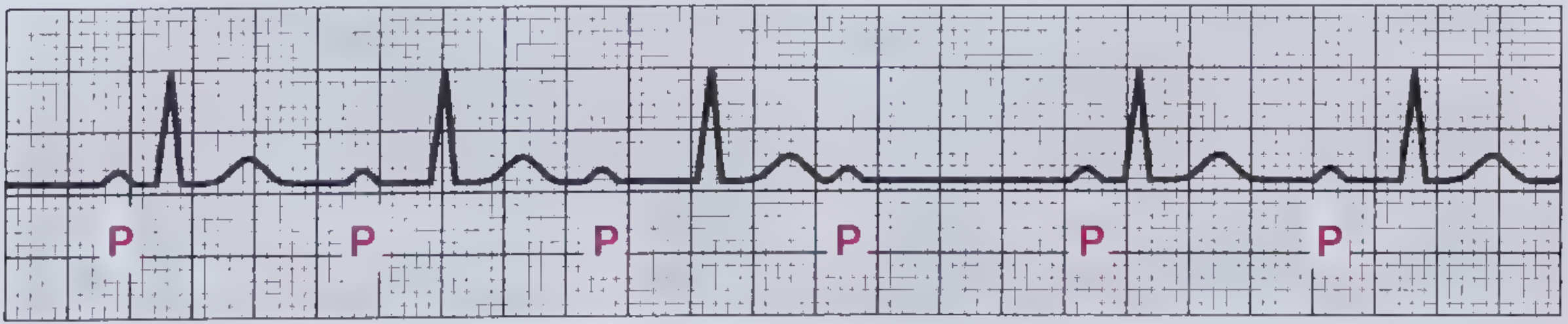
Another example - First-Degree AV Block with labeled P waves:
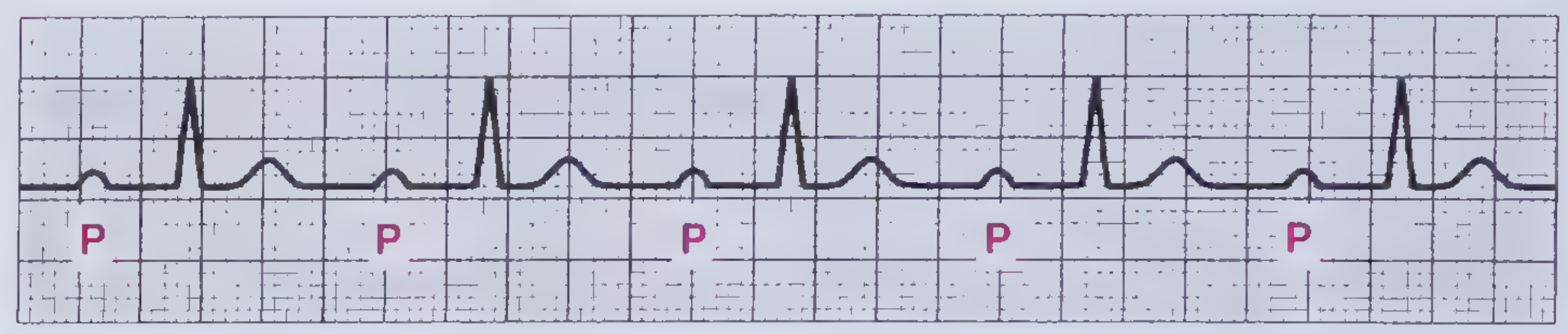
Clinical significance: Usually benign. Commonly seen with increased vagal tone, inferior MI, medications. Requires no specific treatment unless symptomatic or progresses.
SECOND-DEGREE AV BLOCK
Some (not all) atrial impulses conduct to ventricles = intermittent dropped QRS complexes.
SECOND-DEGREE AV BLOCK - MOBITZ TYPE I (WENCKEBACH)
Mechanism: Progressive fatigue/decremental conduction in the AV node until one impulse fails to conduct. The cycle then resets.
Location of block: AV node (above Bundle of His)
ECG Criteria:
- PR interval progressively lengthens beat to beat
- After the longest PR, a P wave is NOT followed by a QRS (dropped beat)
- PR interval after the dropped beat resets to its shortest value
- R-R interval progressively shortens up to the dropped beat
- P-P interval remains constant
- "Grouped beating" is the hallmark - clusters of 3, 4, or 5 beats
Mobitz I is defined by the presence of nonconducted beats that are preceded by conducted beats associated with progressively longer PR intervals on ECG. - Frameworks for Internal Medicine
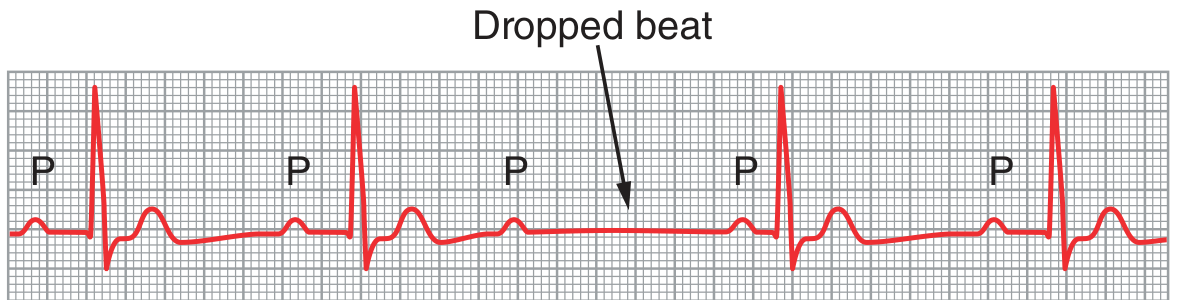
ECG - Mobitz I Wenckebach (from Frameworks for Internal Medicine, Fig 3-3):
P-wave rate is constant. PR gets progressively longer (1st → 2nd → 3rd → 4th P wave), then the 4th P wave is blocked (no QRS). The next PR interval resets to shortest.
ECG - Mobitz I (Type I) - Guyton & Hall, Fig 13.6:
Arrow marks the dropped beat. Note P wave without a QRS response.
Associated with: Right coronary artery territory MI (inferior STEMI - look for ST elevation in II, III, aVF). Usually reversible.
Prognosis: Generally benign. Often reversible if cause treated. Rarely progresses to complete heart block.
Treatment: Usually no treatment needed. Atropine if symptomatic bradycardia. Pacemaker rarely required.
SECOND-DEGREE AV BLOCK - MOBITZ TYPE II
Mechanism: Sudden intermittent failure of conduction WITHOUT prior PR prolongation. The block is below the AV node (infranodal) - in the Bundle of His or bundle branches.
Location of block: Bundle of His or Purkinje system (infranodal)
ECG Criteria:
- PR interval is constant (fixed) before the dropped beat - does NOT progressively lengthen
- Sudden P wave not followed by QRS (dropped beat)
- The PR interval does NOT change before or after the dropped beat
- Conduction ratio may be: 2:1, 3:1, 3:2, 4:3, etc.
- QRS may be wide (if associated bundle branch block, which is common)
Prognosis: Serious. High rate of progression to complete (3rd degree) heart block. Increased mortality.
Treatment: Pacemaker almost always required. Atropine is often ineffective (infranodal block). Dopamine/isoproterenol as bridge.
SECOND-DEGREE AV BLOCK - 2:1 AV BLOCK
A special pattern deserving its own category:
ECG:
- Every other P wave is blocked - alternating conducted and nonconducted beats
- Cannot distinguish Mobitz I from Mobitz II because there are not 2 consecutive conducted beats to compare PR intervals
2:1 AV Block ECG (Frameworks for Internal Medicine, Fig 3-5):

There are twice as many P waves as QRS complexes. Every other P wave is blocked. Cannot differentiate Mobitz I vs II from this pattern alone.
How to determine level of block in 2:1 AV block:
| Feature | Suggests Nodal (Mobitz I) | Suggests Infranodal (Mobitz II) |
|---|---|---|
| QRS width | Narrow | Wide |
| Rate response to atropine | Increases conduction | No improvement |
| Response to exercise | Improves conduction | Worsens |
| Associated MI territory | Inferior | Anterior |
THIRD-DEGREE (COMPLETE) AV BLOCK
Mechanism: No impulses whatsoever pass from atria to ventricles. Atria and ventricles beat completely independently (AV dissociation). A subsidiary escape pacemaker takes over the ventricles.
ECG Criteria (from Guyton & Hall):
- P waves and QRS complexes are completely dissociated - no fixed relationship
- P-P interval is regular (atrial rate ~60-100 bpm)
- R-R interval is regular but SLOWER (escape rhythm)
- PR intervals vary completely - P waves "march through" the QRS complexes
- Escape rhythm rate:
- Junctional escape (AV node/proximal His): 40-60 bpm, narrow QRS
- Ventricular escape (distal His/Purkinje): 20-40 bpm, wide QRS (≥0.12 sec)
Complete block of the impulse from the atria into the ventricles occurs...the P waves become dissociated from the QRS and T complexes...the rate of ventricular beat is less than 40 beats/min. - Guyton & Hall
ECG - Complete (Third-Degree) AV Block (Guyton & Hall, Fig 13.7):
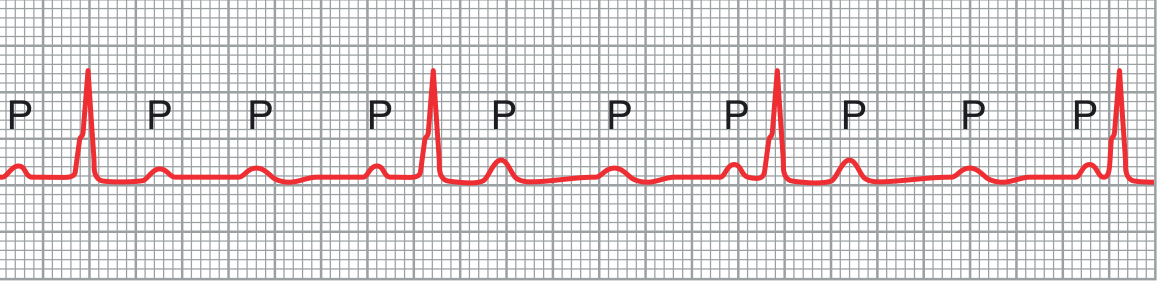
Atrial rate ~100 bpm (P waves). Ventricular rate <40 bpm (QRS). P waves have no relationship to QRS - they march through at their own rate. This is complete AV dissociation.
ECG - Complete Heart Block (2:1 pattern progressed):
Stokes-Adams Syndrome: In complete AV block, the ventricular escape may be delayed 5-30 seconds after block onset, causing syncope (Stokes-Adams attack). Death can occur if escape does not appear within 1-2 minutes.
Clinical Features:
- Wide pulse pressure
- Cannon A waves (JVP) - right atrium contracts against closed tricuspid valve
- Bradycardia
- Syncope, fatigue, heart failure symptoms
- 1-year mortality in symptomatic patients can reach 50% without treatment
Treatment: Permanent pacemaker required in virtually all cases without a reversible cause.
SUMMARY TABLE: AV BLOCK COMPARISON
| Feature | 1st Degree | 2nd Degree Mobitz I | 2nd Degree Mobitz II | 3rd Degree |
|---|---|---|---|---|
| PR interval | Fixed, prolonged >200ms | Progressively lengthens | Fixed, constant | No fixed PR (dissociated) |
| Dropped beats | None | Yes, periodically | Yes, suddenly | All - no conduction |
| P:QRS ratio | 1:1 | e.g. 4:3, 5:4 | e.g. 2:1, 3:1 | P>QRS (dissociated) |
| QRS width | Narrow | Usually narrow | Often wide | Narrow (junctional) or wide (ventricular) |
| Block location | AV node | AV node | Infranodal (His/Purkinje) | Any level |
| Prognosis | Benign | Usually benign | Serious | Life-threatening |
| Pacemaker? | No | Rarely | Almost always | Always |
| Associated MI | Inferior | Inferior | Anterior | Any |
QUICK MEMORY AIDS
SA Block Types:
- 1st degree = delay but conducts (invisible on ECG)
- 2nd degree Type I = P-P shortens then drops (Wenckebach pattern)
- 2nd degree Type II = constant P-P then exact double pause
- 3rd degree = no exit at all, escape rhythm takes over
AV Block Types:
- 1st = "Long PR, no dropped beats" → PR > 200ms
- 2nd Mobitz I = "Longer, longer, longer, DROP - then reset" (Wenckebach)
- 2nd Mobitz II = "Same PR, then sudden DROP" → dangerous
- 3rd = "Completely divorced" - P and QRS independent
Poem for 1st degree: "If the P-R is long and more than two, first-degree block is running through."
Sources: Guyton and Hall Textbook of Medical Physiology; Harrison's Principles of Internal Medicine 22E (2025); Frameworks for Internal Medicine; Braunwald's Heart Disease; LITFL ECG Library
This is a shared conversation. Sign in to Orris to start your own chat.