Osteomyelitis detailed explanation
Reading File
Finding Sources
Searching PubMed
osteomyelitis management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
I now have extensive, authoritative content from multiple textbooks. Here is the comprehensive explanation:
Osteomyelitis - Detailed Explanation
1. Definition
Osteomyelitis is inflammation of bone and bone marrow, virtually always secondary to infection. It may complicate a systemic infection but frequently presents as a solitary primary focus. All types of organisms - bacteria, viruses, fungi, and parasites - can cause it, but pyogenic bacteria and mycobacteria are by far the most common culprits. - Robbins, Cotran & Kumar Pathologic Basis of Disease
2. Routes of Infection
Organisms reach bone by three pathways:
| Route | Details |
|---|---|
| Hematogenous spread | Most common in children; bacteremia seeds bone from trivial mucosal injuries or skin infections |
| Contiguous spread | Extension from adjacent infected soft tissue or joint |
| Direct implantation | Compound fractures, surgical procedures, puncture wounds |
In adults, osteomyelitis is most often a complication of open fractures, surgical procedures, or diabetic foot infections. - Robbins & Kumar Pathologic Basis of Disease
3. Why the Metaphysis? (Vascular Anatomy)
The location of bone infection is determined by the osseous vascular circulation, which varies with age:
- Neonates: Metaphyseal vessels penetrate the growth plate, so both the metaphysis and epiphysis (and adjacent joint) are at risk. This is why neonatal osteomyelitis commonly spreads to the joint and causes septic arthritis.
- Older children: The metaphysis is the typical site. Slow blood flow through looped metaphyseal vessels combined with microtrauma during bacteremia encourages seeding.
- Adults: After growth plate closure, anastomoses form between metaphyseal and epiphyseal vessels, making subchondral and epiphyseal regions more susceptible.
Infection starts in the metaphyses of long bones, where the slow flow through looped vessels combined with microtrauma encourages seeding during bacteremia. - Bailey and Love's Short Practice of Surgery 28th Ed
4. Causative Organisms
| Setting | Organism |
|---|---|
| Children (all ages, most common) | Staphylococcus aureus (80-90% of culture-positive cases; MRSA is now most common in AHO) |
| Neonates | Group B Streptococci, E. coli |
| Sickle cell disease | Salmonella spp. and other gram-negatives (splenic dysfunction + osteonecrotic nidus) |
| Contiguous/postoperative | Polymicrobial |
| Immunocompromised | Fungi, atypical mycobacteria |
| Spine | S. aureus, gram-negatives, Mycobacterium tuberculosis (Pott disease) |
S. aureus dominates because its cell wall proteins bind bone matrix components such as collagen, facilitating bacterial adherence. Cultures are only positive in approximately 50% of patients. - Robbins, Cotran & Kumar
5. Pathology: Stages and Morphology
Acute Phase
- Bacteria proliferate and induce a neutrophilic reaction
- Necrosis of bone cells and marrow occurs within 48 hours
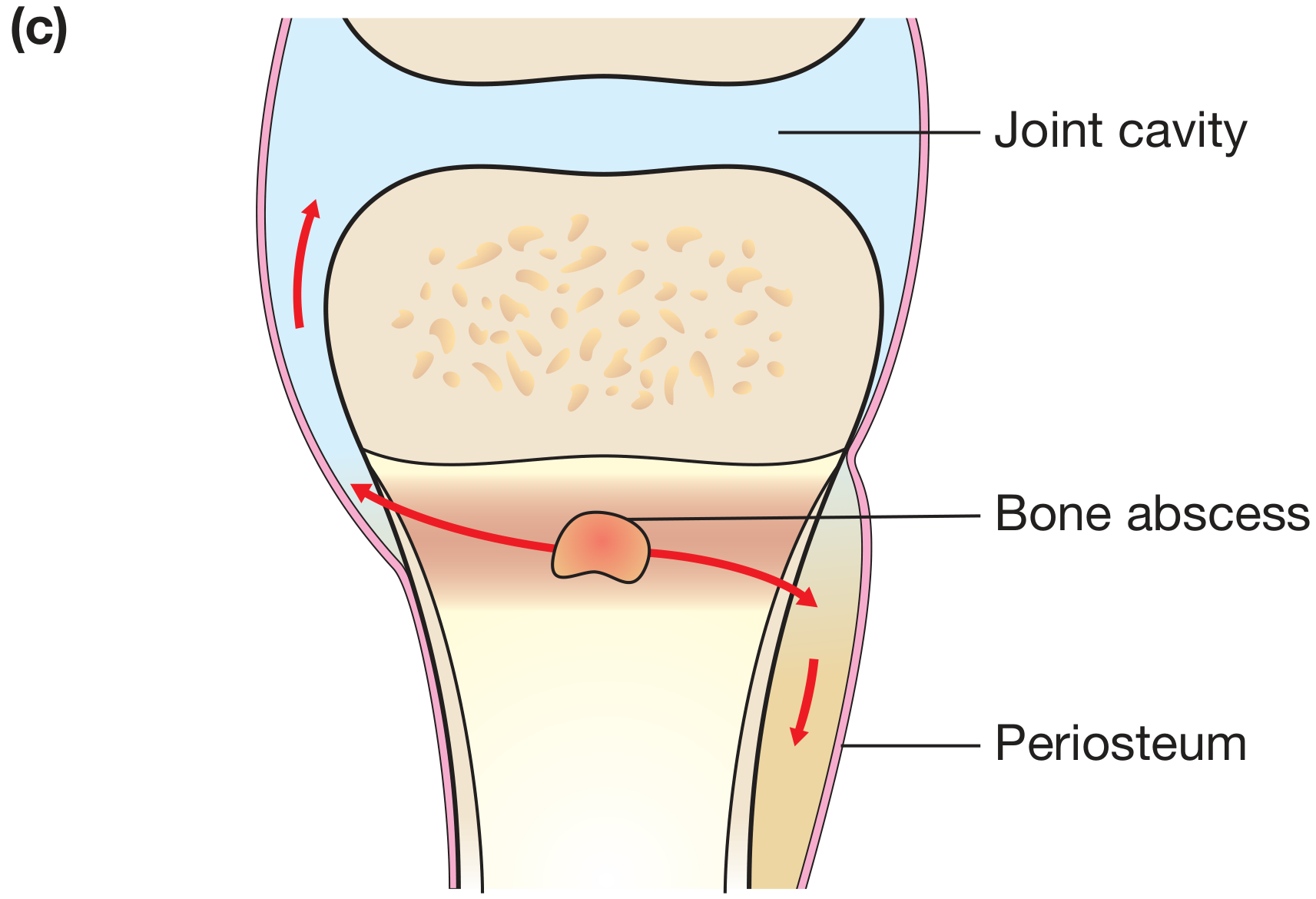
- Bacteria and the inflammatory response spread through Haversian canals to the periosteum
- Because the periosteum is loosely attached to the cortex in children, pus can easily travel along the shaft beneath it (subperiosteal abscess)
- In adults, the periosteum is more firmly attached, so subperiosteal abscesses are less common
Abscess and Necrosis
- Pressure from the abscess leads to bony destruction
- Pus passes through cortical bone and elevates the periosteum, rendering cortical bone avascular (ischemic necrosis)
- Areas of dead bone cut off from blood supply = sequestra
Chronic Phase - the classic triad:
| Term | Definition |
|---|---|
| Sequestrum | Fragment of dead, devascularized bone; acts as a nidus for persistent infection |
| Involucrum | New periosteal bone that forms around the sequestrum (stimulated by periosteal elevation); creates a "bone-within-a-bone" appearance |
| Cloaca | Gaps/perforations in the involucrum through which pus may track outward |
| Sinus tract | When pus tracks to the skin surface, forming a draining fistula; common in chronic osteomyelitis |
| Brodie abscess | A subacute form - a well-defined lytic lesion with a sclerotic rim on imaging (chronic walled-off infection) |
The periosteal elevation is a potent stimulus for new bone formation. In untreated or chronic infection, new bone (involucrum) surrounds the dead bone (sequestrum), leading to a 'bone-within-a-bone' appearance. - Bailey and Love's 28th Ed
6. Classification
By Duration
- Acute: < 2 weeks; predominantly neutrophilic, marrow edema
- Subacute: 2 weeks - 3 months; includes Brodie abscess
- Chronic: > 3 months; sequestrum, involucrum, sinus tracts, sclerosis
By Mechanism (Waldvogel Classification)
- Hematogenous - most common in children
- Contiguous focus without vascular insufficiency - e.g., post-trauma/surgery
- Contiguous focus with vascular insufficiency - e.g., diabetic foot
Cierny-Mader Staging (for chronic osteomyelitis)
- Stage 1 (Medullary): infection within medullary canal
- Stage 2 (Superficial): cortical surface infection only
- Stage 3 (Localized): full-thickness cortical involvement
- Stage 4 (Diffuse): circumferential, unstable bone
7. Clinical Features
Acute Osteomyelitis
- Fever, rigors, may appear toxic
- Systemic symptoms: headache, fatigue, malaise, anorexia
- Point tenderness over infected segment - the most consistent physical finding
- Localized warmth, swelling, erythema
- Children: sudden limp or refusal to bear weight on the affected limb
- Children with AHO have a male:female ratio of 2:1 to 3:1; involves long bones ~80% of the time; distal metaphysis is the most common site
Chronic Osteomyelitis
- Less systemic toxicity
- Persistent local pain and tenderness
- Draining sinus tracts
- Palpable involucrum or sequestrum
- Sympathetic effusion in adjacent joint (even when the joint itself is not infected) - Rosen's Emergency Medicine
8. Investigations
Laboratory
| Test | Finding |
|---|---|
| CBC | Leukocytosis (may be absent in chronic OM) |
| ESR | Elevated in >90% of acute cases |
| CRP | Elevated; useful for monitoring treatment response |
| Blood cultures | Positive in ~50% acute, nearly always negative in chronic OM |
| Bone biopsy culture | Gold standard for organism identification |
Cultures from draining fistulas or sinus tracts are not a reliable substitute - organisms from sinus tracts often differ from those in the underlying bone. - Rosen's Emergency Medicine
Imaging
| Modality | Findings | Timing |
|---|---|---|
| Plain X-ray | Soft tissue swelling, cortical irregularity, periosteal reaction, bone destruction | Lags up to 2 weeks behind clinical onset |
| Ultrasound | Subperiosteal fluid collection, soft tissue abscess; useful in infants; guides aspiration | Early |
| CT | Best for defining cortical destruction, identifying sequestra, surgical planning | Useful in chronic OM |
| MRI with gadolinium | Highest sensitivity and specificity; T1: decreased marrow signal; T2: increased signal; gadolinium differentiates viable from devitalized bone; identifies sinus tracts, abscesses | Best for early detection |
| Radionuclide scan (³⁹⁹mTc-MDP) | 3-phase bone scan; useful when MRI unavailable or contraindicated; whole-body scan valuable in multifocal disease | Outpatient evaluation |
MRI: osteomyelitis produces a diminished intensity of the normal marrow signal on T1-weighted images and normal or increased signal on T2-weighted images. Gadolinium should be used if there are no contraindications - it enhances the interface between normal and abnormal marrow and helps distinguish abscess from phlegmon. - Rosen's Emergency Medicine
A subacute infection on MRI may show a characteristic penumbra sign: a peripheral high-signal ring (granulation tissue) surrounding a low-signal central zone (abscess cavity). - Grainger & Allison's Diagnostic Radiology
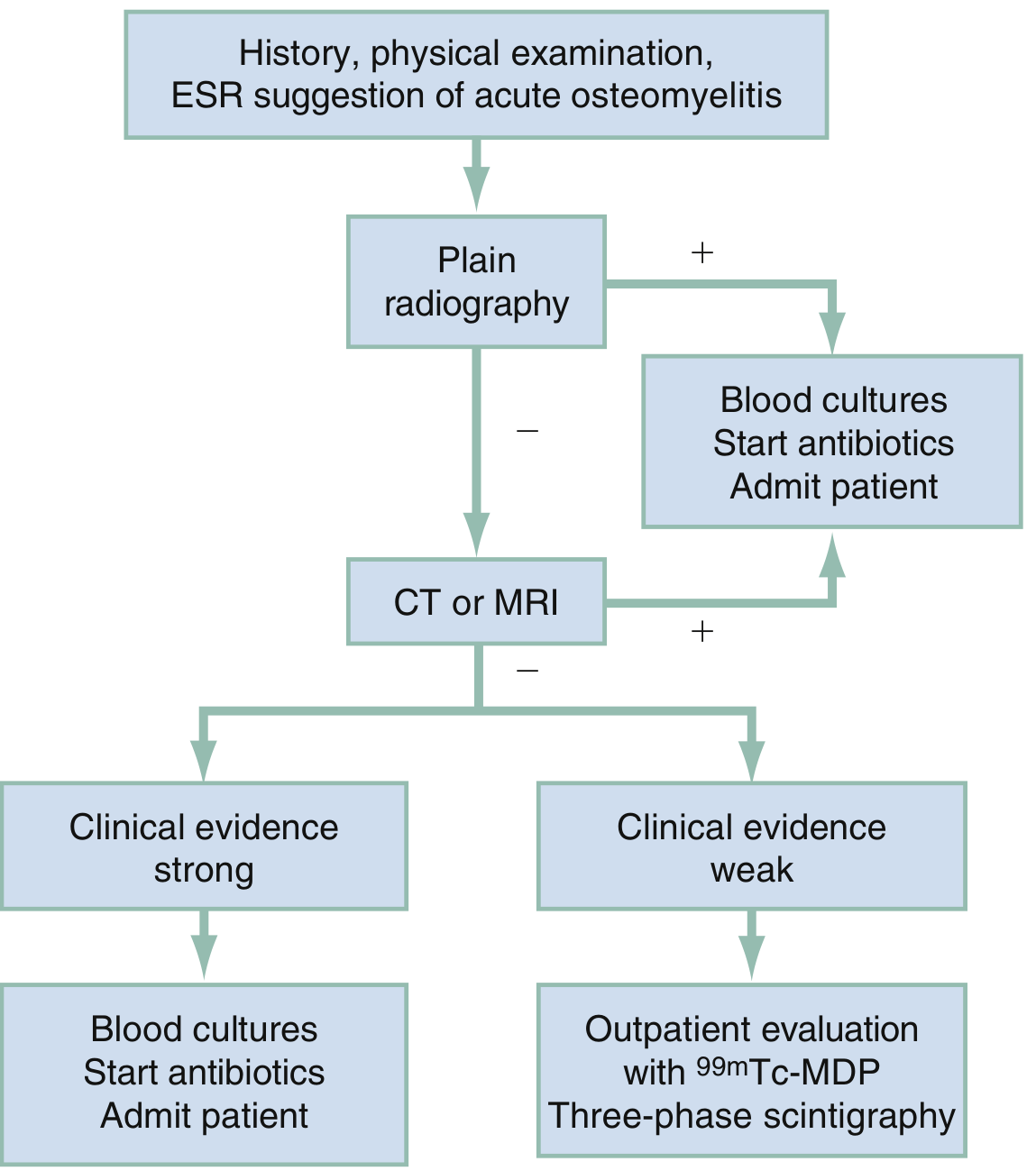
Diagnostic Algorithm
9. Special Forms
Vertebral Osteomyelitis (Spondylodiscitis)
- Most common in adults over 50
- Hematogenous seeding of vertebral endplates
- Low back pain + fever; neurological complications if epidural abscess forms
- MRI shows endplate destruction, disc space involvement (distinguishes from tumor)
- Common organisms: S. aureus, gram-negatives, Mycobacterium tuberculosis (Pott disease)
- Pott disease: destroys vertebral bodies and intervertebral discs leading to compression fractures and kyphosis
Diabetic Foot Osteomyelitis
- Usually contiguous spread from soft tissue ulcer
- Polymicrobial (S. aureus, Streptococcus, gram-negatives, anaerobes)
- Probe-to-bone test: high predictive value if bone is palpable
- Treatment: prolonged antibiotics; surgical debridement often required
Chronic Recurrent Multifocal Osteomyelitis (CRMO)
- Non-infectious, autoinflammatory condition in children
- Mimics infectious osteomyelitis
- Treatment: NSAIDs, bisphosphonates
10. Management
Principles
The goal of therapy is to contain the infection before bone necrosis occurs, as cure rates fall dramatically once necrosis develops. - Rosen's Emergency Medicine
Medical Management (Antibiotics)
Empirical therapy is started after blood cultures are drawn. Choice guided by:
- Most likely organism (age, setting, local MRSA prevalence)
- Culture and sensitivity results when available
| Setting | Empirical Choice |
|---|---|
| Children (MSSA likely) | Anti-staphylococcal penicillin (nafcillin/flucloxacillin) or first-generation cephalosporin |
| MRSA suspected/confirmed | Vancomycin (IV); oral linezolid or trimethoprim-sulfamethoxazole for step-down |
| Neonates | Cover S. aureus + gram-negatives (e.g., nafcillin + gentamicin) |
| Adults (hematogenous vertebral) | Anti-staphylococcal ± gram-negative coverage depending on risk |
Duration: Typically 4-6 weeks total (IV then oral step-down once clinically and biochemically improving). Shorter IV courses followed by oral antibiotics are now accepted for uncomplicated acute hematogenous osteomyelitis in children responding well.
- IV to oral switch is appropriate once the patient is improving clinically and haematologically
- MRSA with the Panton-Valentine leukocidin gene increases morbidity - Bailey & Love
Surgical Management
Indicated for:
- Formation of abscess (requires drainage)
- Presence of sequestrum (requires surgical removal - sequestrectomy)
- Failure to respond to antibiotics
- Chronic osteomyelitis with involucrum
- Pathological fracture
- Spinal cord compression (vertebral OM)
- Implant-related infections
Surgical principles for chronic osteomyelitis:
- Debridement of all necrotic and infected tissue
- Dead space management: antibiotic-loaded PMMA beads (e.g., gentamicin), calcium sulfate beads, or muscle/fasciocutaneous flap closure
- Stabilization of the affected bone if needed
- Antibiotic-loaded implants and local delivery systems are used as adjuncts to systemic antibiotics
Adjunctive Therapies
- Rest and splintage of the affected limb
- Analgesia
- Hyperbaric oxygen (adjunct in refractory/ischemic osteomyelitis)
- Correction of underlying conditions (nutritional deficiency, sickle cell disease, diabetes)
11. Complications
| Complication | Notes |
|---|---|
| Bacteremia and sepsis | Can occur with acute osteomyelitis |
| Septic arthritis | Direct spread to adjacent joint, especially in neonates and when metaphysis is intracapsular (hip, shoulder) |
| Growth disturbance | Epiphyseal involvement damages the growth plate; results in shortened or deformed limb |
| Pathological fracture | Through areas of infected/necrotic bone |
| Chronic osteomyelitis | Most feared long-term complication; sequestrum perpetuates infection |
| Squamous cell carcinoma | Rare but well-recognized complication of long-standing sinus tracts (Marjolin's ulcer) |
| Brain abscess, meningitis, empyema | Extension depending on site of infection |
| Amyloidosis | Rare complication of long-standing chronic osteomyelitis (secondary/AA amyloidosis) |
Treated appropriately, most cases of sepsis resolve with no sequelae. However, in the neonate, vascular channels pass through the physis, connecting the metaphysis with the epiphysis, and poorer outcomes may ensue. - Bailey & Love
12. Prognosis
- Acute hematogenous osteomyelitis in children: excellent prognosis with early IV antibiotic treatment; many cases do not require surgery
- Vertebral osteomyelitis: generally responds to prolonged antibiotics; surgery needed for spinal instability or neurological compromise
- Chronic osteomyelitis: difficult to eradicate; recurrence is common; requires combined medical and surgical approach
- Diabetic foot osteomyelitis: high risk of recurrence; amputation may be required
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Bailey and Love's Short Practice of Surgery 28th Ed | Rosen's Emergency Medicine | Grainger & Allison's Diagnostic Radiology | Campbell's Operative Orthopaedics 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.