Footdrop Differential
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative neurology textbooks. Let me compile this into a structured differential diagnosis.
Foot Drop — Differential Diagnosis
Foot drop (inability to dorsiflex the foot) results from dysfunction anywhere along the neuraxis from cortex to muscle. The anatomical level of the lesion is the primary organizing framework.
Anatomical Framework
Cortex/UMN → Spinal Cord → Anterior Horn Cell →
Nerve Root (L4–L5) → Lumbosacral Plexus →
Sciatic Nerve → Common Peroneal Nerve → Muscle
1. Peripheral Nerve — Most Common Causes
Common Peroneal (Fibular) Neuropathy ⭐ Most common cause of unilateral foot drop
- Compression at the fibular head (vulnerable due to superficial location)
- Classic precipitants: leg crossing, weight loss/emaciation, prolonged squatting, tight casts, lateral decubitus positioning, total knee arthroplasty, yoga, natural childbirth ("pushing palsy")
- Also: trauma (bumper injury), intraneural ganglia from superior tibiofibular joint, vasculitis
- Deficits: foot dorsiflexion ↓, eversion ↓, toe extension ↓; sensory loss over anterolateral leg and dorsum of foot
- Key distinguishing feature: foot inversion is spared (tibialis posterior = tibial nerve, intact)
- Most cases resolve spontaneously when mechanical cause removed
— Harrison's Principles of Internal Medicine 22E; Neuroanatomy through Clinical Cases 3rd Ed.
Sciatic Neuropathy
- Causes: hip arthroplasty, pelvic surgery/lithotomy position, trauma, hematoma, tumor, vasculitis, idiopathic
- The peroneal division of the sciatic nerve is disproportionately vulnerable, so presentation may mimic peroneal neuropathy alone
- Full sciatic: weakness of all ankle/toe movements + knee flexion; sensory loss entire foot + distal lateral leg; absent ankle jerk
— Harrison's Principles of Internal Medicine 22E
Peripheral Neuropathy (Bilateral foot drop)
- Charcot-Marie-Tooth disease (hereditary motor-sensory neuropathy, peroneal muscular atrophy) — classic distal-predominant pattern
- Chronic acquired neuropathies: diabetic, inflammatory (CIDP), toxic, nutritional
- Guillain-Barré syndrome (ascending), tick paralysis
- Amyloid neuropathy
— Adams and Victor's Principles of Neurology 12th Ed.; Rosen's Emergency Medicine
2. Nerve Root
L5 Radiculopathy ⭐ Key mimic of peroneal palsy
- Common causes: disc herniation (L4–L5), degenerative joint disease, osteophytes
- Deficits: foot dorsiflexion ↓, eversion ↓, inversion ↓ (tibialis posterior = L5 via tibial nerve)
- May have hip abduction weakness (gluteus medius, L5)
- Back/buttock/lateral leg pain often present; paresthesias in L5 distribution (lateral leg → dorsum of foot → great toe)
- EMG: denervation in L5-innervated muscles (including tibialis posterior and gluteus medius — not peroneal territory)
Critical L5 radiculopathy vs. Peroneal palsy distinction:
| Feature | Peroneal Neuropathy | L5 Radiculopathy |
|---|---|---|
| Foot dorsiflexion | Weak | Weak |
| Foot eversion | Weak | Weak |
| Foot inversion | Spared | Weak |
| Hip abduction | Spared | May be weak |
| Ankle jerk | Normal | Normal (S1 root) |
| EMG | Slowing at fibular head | Denervation in L5 muscles |
| Back/radicular pain | Absent | Usually present |
— Harrison's 22E; Schwartz's Surgery 11th Ed.; Neuroanatomy through Clinical Cases 3rd Ed.
L4 Radiculopathy
- Less common cause; weakness of tibialis anterior + inversion; diminished patellar reflex
3. Lumbosacral Plexopathy
- Trauma, retroperitoneal hematoma, tumor (lymphoma, sarcoma), radiation, diabetic amyotrophy (Bruns-Garland syndrome)
- L5 division of plexus involvement → foot drop + variable other lower limb deficits
- Key: pattern of weakness exceeds a single nerve or root territory
4. Anterior Horn Cell Disease
- ALS (Amyotrophic Lateral Sclerosis): can present with focal lower motor neuron foot drop early; look for UMN signs elsewhere, fasciculations, bulbar involvement
- Progressive spinal muscular atrophy
- Poliomyelitis (or post-polio syndrome)
— Adams and Victor's Principles of Neurology 12th Ed.
5. Central / Upper Motor Neuron
Spasticity (UMN Foot Drop)
- Stroke (cortical or subcortical — foot area of motor cortex or internal capsule)
- MS plaques affecting corticospinal tracts
- Cerebral palsy
- Spinal cord lesion (myelopathy)
- Gait: spastic/circumduction rather than high-steppage; hyperreflexia, upgoing plantar response
6. Muscle / Neuromuscular Junction
Myopathies
- Distal muscular dystrophies (e.g., Miyoshi, Nonaka, Welander) — distal leg involvement
- Scapuloperoneal syndromes (facioscapulohumeral MD variant)
- Myotonic dystrophy (distal weakness, foot drop can be presenting feature)
Non-neuromuscular musculoskeletal
- Tibialis anterior tendon (TAT) rupture — pure foot drop, no sensory loss, no neurologic signs; pathognomonic: absent tendon palpation; spared eversion and hip abduction
— Localization in Clinical Neurology 8e
7. Other / Functional
Dystonia
- Action dystonia of foot (equinovarus posture while walking); dystonia may diminish or resolve when walking backwards — a pathognomonic feature
- Sensory trick (geste antagoniste) may relieve it
Sensory Ataxia
- Mimics foot drop gait; seen in severe polyneuropathy, dorsal column disease (tabes dorsalis, subacute combined degeneration, B12 deficiency)
- Romberg positive; high-stepping due to proprioceptive loss rather than true dorsiflexion weakness
Functional (psychogenic)
- Inconsistent weakness, Hoover sign positive, non-anatomic sensory loss
Summary by Level
| Level | Key Diagnoses |
|---|---|
| Cortex/UMN | Stroke, MS, myelopathy, CP |
| Anterior horn | ALS, SMA, polio |
| Root (L4–L5) | Disc herniation, DJD, spondylolisthesis |
| Plexus | Diabetic amyotrophy, trauma, tumor, radiation |
| Sciatic nerve | Hip surgery, trauma, hematoma, vasculitis |
| Peroneal nerve | Compression at fibular head (most common) |
| Muscle | Distal dystrophies, scapuloperoneal syndromes |
| Tendon | TAT rupture |
| Other | Dystonia, sensory ataxia, functional |
High-Yield Diagnostic Approach
- Inversion intact? → Points to peroneal nerve (not L5 root)
- Knee flexion weak? → Points to sciatic nerve (not peroneal)
- Bilateral? → Think polyneuropathy (CMT, GBS, diabetes), ALS, myelopathy
- Back pain + radiation? → L5 radiculopathy
- UMN signs? → Central cause (stroke, MS, cord)
- No sensory loss, no EMG abnormality? → TAT rupture, dystonia, functional
- EMG/NCS — indispensable: peroneal motor conduction shows slowing/amplitude drop across fibular head in peroneal palsy; L5 denervation involves tibialis posterior (tibial nerve territory) in radiculopathy
— Bradley and Daroff's Neurology in Clinical Practice; Adams and Victor's Principles of Neurology 12th Ed.; Harrison's Principles of Internal Medicine 22E; Localization in Clinical Neurology 8e; Neuroanatomy through Clinical Cases 3rd Ed.
Difference between deep and common peroneal nerve
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I have all the needed information. Here's a comprehensive comparison:
Common vs. Deep Peroneal Nerve
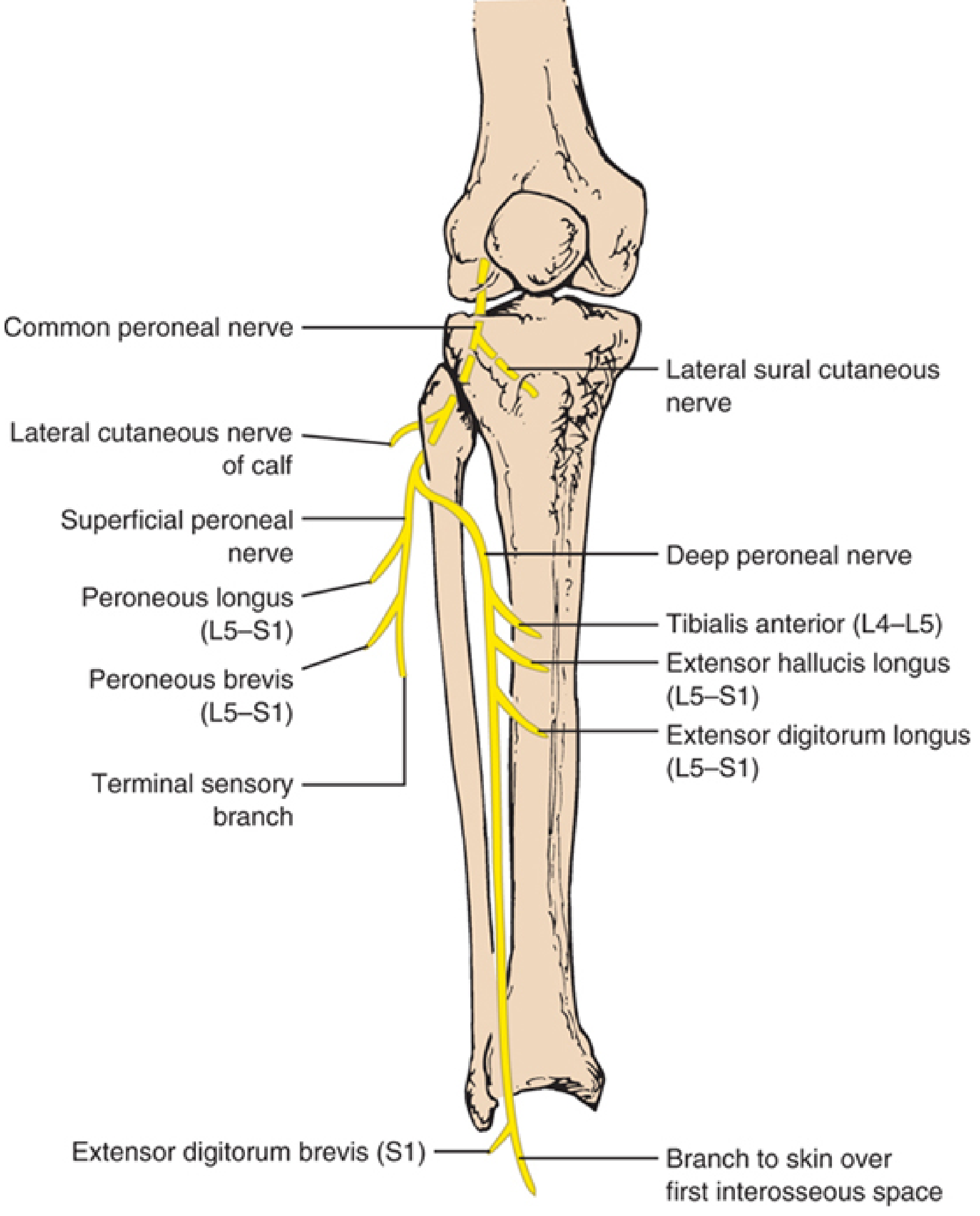
The peroneal nerve and its branches — Localization in Clinical Neurology, 8e
The Hierarchy
Sciatic nerve (L4–S2)
└── Common Peroneal Nerve ← divides at fibular head
├── Superficial Peroneal Nerve
└── Deep Peroneal Nerve
The common peroneal nerve is the parent trunk. It is not the same as the deep peroneal nerve — it gives rise to both the superficial and deep branches after rounding the fibular head and entering the substance of peroneus longus.
Comparison Table
| Feature | Common Peroneal | Deep Peroneal | Superficial Peroneal |
|---|---|---|---|
| Origin | Terminal branch of sciatic | Branch of common peroneal | Branch of common peroneal |
| Root levels | L4–S2 | L4–L5 (predominant) | L5–S1 |
| Division point | N/A (it is the trunk) | At fibular head, within peroneus longus | At fibular head, within peroneus longus |
| Course | Popliteal fossa → lateral, winds around fibular neck | Anterior compartment of leg, runs with anterior tibial artery | Lateral compartment of leg |
| Compartment | None (passes through fibular tunnel) | Anterior | Lateral |
Motor Innervation
| Nerve | Muscles | Action |
|---|---|---|
| Common peroneal | None directly (proximal to bifurcation) | — |
| Deep peroneal | Tibialis anterior (L4–L5) | Dorsiflexion + inversion |
| Extensor hallucis longus (L5–S1) | Great toe extension + dorsiflexion | |
| Extensor digitorum longus (L5–S1) | Lateral toe extension + dorsiflexion | |
| Extensor digitorum brevis (L5–S1) | Toe extension at proximal phalanges | |
| Superficial peroneal | Peroneus longus (L5–S1) | Plantar flexion + eversion |
| Peroneus brevis (L5–S1) | Plantar flexion + eversion |
Key motor distinction: The deep peroneal nerve drives dorsiflexion (foot drop if injured); the superficial peroneal nerve drives eversion.
Sensory Innervation
| Nerve | Sensory Territory |
|---|---|
| Common peroneal | Gives off lateral sural cutaneous nerve (lateral leg below knee) before bifurcating |
| Deep peroneal | Small patch: first web space (dorsal skin between 1st and 2nd toes) only |
| Superficial peroneal | Dorsum of foot and toes (except 1st web space) + distal anterolateral leg |
The deep peroneal nerve is predominantly motor with a tiny sensory territory. The superficial peroneal nerve has a large sensory distribution over the dorsum of the foot.
Clinical Syndromes by Level
Common Peroneal Neuropathy (at fibular head)
- Affects both branches → complete foot drop (dorsiflexion ↓) + eversion ↓
- Sensory loss: dorsum of foot + anterolateral leg
- Most common: compression at fibular head (leg crossing, weight loss, cast, arthroplasty)
Isolated Deep Peroneal Neuropathy (anterior tarsal tunnel syndrome)
- Compression at the inferior extensor retinaculum / talonavicular joint level
- Dorsiflexion weak (tibialis anterior, toe extensors); eversion spared
- Sensory loss confined to 1st web space
- Causes: tight footwear, ganglion cyst, osteophyte
Isolated Superficial Peroneal Neuropathy
- Eversion weakness; dorsiflexion spared (no foot drop)
- Sensory loss over dorsum of foot
- Causes: ankle inversion/plantar flexion sprains, lateral compartment hernias, fascial defects, surgery
High-Yield Bedside Distinction
| Finding | Implies |
|---|---|
| Foot drop + eversion loss + dorsal foot numbness | Common peroneal palsy |
| Foot drop alone, eversion intact, 1st web space numb | Deep peroneal palsy |
| Eversion weakness, no foot drop, dorsal foot numb | Superficial peroneal palsy |
| Foot drop + inversion loss | L5 radiculopathy (or sciatic nerve) |
Note: In 20–28% of individuals an accessory deep peroneal nerve (branch of the superficial peroneal) supplies the lateral portion of extensor digitorum brevis — an anatomical variant that can mislead EMG interpretation.
— Localization in Clinical Neurology 8e; Imaging Anatomy Text and Atlas Vol. 3; Harrison's Principles of Internal Medicine 22E
Bilateral footdrop causes
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.