Carpal Tunnel Syndrome
Reading File
Finding Sources
Searching PubMed
"carpal tunnel syndrome"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough answer. Here is the complete overview of Carpal Tunnel Syndrome:
Carpal Tunnel Syndrome (CTS)
Anatomy
The carpal tunnel is a rigid bony-fibrous canal bounded on three sides by the carpal bones and volarly (anteriorly) by the transverse carpal ligament (flexor retinaculum). Nine flexor tendons plus the median nerve pass through this tunnel. Any process that increases pressure within this fixed-volume space compresses the nerve.
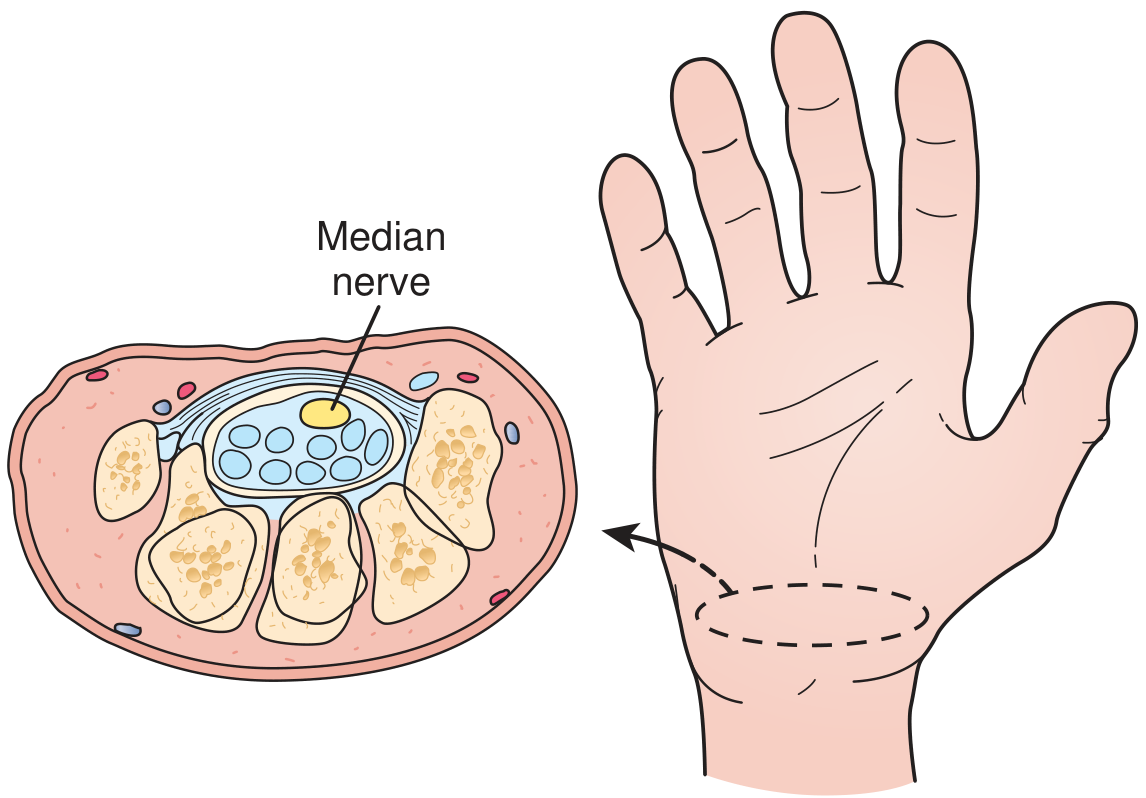
Cross-section of the wrist: the median nerve (yellow, central) and nine flexor tendons (blue ovals) travel within the carpal tunnel. - Textbook of Family Medicine 9e
Definition & Epidemiology
CTS is the most common compressive (entrapment) mononeuropathy, caused by compression of the median nerve at the wrist. It affects approximately 3% of the adult American population and is 3x more prevalent in women. About half of patients are aged 40-60 years, though it occasionally occurs in children. It is now recognized as an occupational hazard related to repetitive wrist/hand motion (e.g., typing). - Firestein & Kelley's Textbook of Rheumatology
Risk Factors & Associated Conditions
CTS is usually idiopathic but is associated with many conditions:
| Category | Specific Causes |
|---|---|
| Physiological | Pregnancy (usually resolves post-delivery), obesity |
| Endocrine/Metabolic | Diabetes, hypothyroidism (myxedema), acromegaly |
| Inflammatory/Rheumatic | Rheumatoid arthritis, gout, tenosynovitis |
| Structural | Osteoarthritis, synovial cysts, wrist trauma |
| Infiltrative | Amyloid deposition, sarcoidosis |
| Systemic disease | Congestive heart failure, multiple myeloma, tuberculosis |
| Occupational | Repetitive hand/wrist motion |
Screening blood studies (thyroid function, glucose, inflammatory markers) should be checked in all patients. - Bradley and Daroff's Neurology in Clinical Practice
Pathophysiology
The most common mechanism is tenosynovitis of the hand flexors, leading to swelling within the tunnel, which raises intracanal pressure and compresses the median nerve. Prolonged or severe compression causes demyelination and eventually axonal injury, producing both sensory and motor deficits.
Clinical Features
Symptoms
- Nocturnal paresthesia - the hallmark; waking the patient at night
- Numbness, tingling, pain in the distribution of the median nerve: thumb, index finger, middle finger, and radial half of the ring finger (radial 3.5 digits)
- Relief by shaking or elevating the hand ("flick sign")
- Diffuse brachialgia or shoulder pain may be present
- Weakness or clumsiness of the hand, reduced grip strength
Key Anatomical Note
The palmar cutaneous branch of the median nerve leaves the nerve proximal to the flexor retinaculum - so sensory loss in CTS involves the distal thumb/index/middle fingers but not the thenar eminence skin itself. This is a useful diagnostic point. - Bradley and Daroff's Neurology
Signs (Physical Examination)
| Sign / Test | How Performed | Sensitivity / Notes |
|---|---|---|
| Tinel's sign | Tap over the carpal tunnel at the volar wrist; paresthesia radiates in median distribution | ~50-60%; indicates nerve irritation |
| Phalen's maneuver | Sustained wrist flexion 90° for up to 1 min; reproduction of symptoms | ~74% sensitive, ~25% false-positive rate |
| Carpal compression test | Direct manual compression over the tunnel | Most sensitive provocative test |
| Thenar atrophy | Wasting of the thenar eminence (abductor pollicis brevis) | Late sign - advanced disease |
| Decreased sensation | Objective sensory loss in median distribution | Late sign |
Diagnosis
The diagnosis is primarily clinical. The combination of:
- History of pain/paresthesia in the median nerve distribution
- Thenar atrophy
- Decreased sensation over radial 3.5 digits
...correlates strongly with positive nerve conduction studies and is highly diagnostic.
Nerve Conduction Studies (NCS) / Electrodiagnostics:
- Gold standard for confirmation - prolonged distal motor and sensory latencies across the carpal canal
- EMG shows polyphasic reinnervation potentials in the abductor pollicis brevis
- Not needed to initiate treatment in most patients but should be done before surgery
- Note: up to 25% false-negative rate in clinically confirmed CTS
- Also useful to exclude cervical radiculopathy or thoracic outlet syndrome (by adding cervical paraspinal EMG, H-reflex, F-waves)
Imaging: Generally not required for diagnosis, though ultrasound can show nerve swelling and is used to guide injections. - Goldman-Cecil Medicine
Treatment
Conservative (First-line)
- Activity modification - ergonomic changes, wrist support pads, avoiding provocative positions
- Wrist splinting in neutral position - most effective at night; prevents provocative positioning; should not hold the wrist beyond 10 degrees of extension. Beneficial for mild compression but limited long-term efficacy
- Nerve gliding exercises - routinely prescribed, can provide relief
- NSAIDs / oral analgesics - symptom control (though studies show no more effective than placebo for the underlying condition)
- Vitamin B6 (100-200 mg/day) - helpful in some cases, efficacy not confirmed in RCTs
- Corticosteroid injection - highly effective short-term; long-term efficacy mixed. Technique: inject triamcinolone acetonide or methylprednisolone (5-10 mg) medial to the palmaris longus tendon at 45° angle toward the index finger. Best used when condition is temporary (e.g., pregnancy) or surgery must be deferred. Ultrasound guidance reduces the risk of nerve injury
Most patients improve with conservative measures, but the majority relapse within 1 year. - Textbook of Family Medicine 9e
Surgical (Definitive)
Indications:
- Failed adequate conservative treatment
- Recurrent symptoms after conservative management
- Objective sensory loss or thenar atrophy (late findings) - these warrant early surgery
Procedure: Carpal tunnel release (division of the transverse carpal ligament). The incision is no more than 3 cm and parallels the palmar skin creases.
- Open release vs. Endoscopic release: equivalent long-term results; endoscopic approach is generally preferred (smaller incision, faster recovery)
- Outcomes are excellent
Differential Diagnosis
- Cervical radiculopathy (C6/C7) - proximal symptoms, neck pain, positive Spurling's
- Thoracic outlet syndrome - positional, vascular features
- Cubital tunnel syndrome - ulnar nerve; involves 4th/5th fingers, not median distribution
- Pronator teres syndrome - more proximal median nerve entrapment; thenar eminence sensation IS affected (distinguishes from CTS)
- Peripheral neuropathy - bilateral, stocking-glove distribution
Special Populations
Pregnancy: CTS is common due to fluid retention and hormonal changes. Usually resolves after delivery. Corticosteroid injection or splinting is preferred; surgery is deferred unless severe. - Creasy & Resnik's Maternal-Fetal Medicine
Recent Evidence
Three recent high-quality studies (2024-2025) add context:
- A 2024 global meta-analysis (PMID 39672798) updated prevalence data worldwide
- A 2025 network meta-analysis (PMID 40315975) in Archives of Physical Medicine and Rehabilitation systematically compared conservative treatments - corticosteroid injection ranked among the most effective short-term options
Sources: Firestein & Kelley's Textbook of Rheumatology | Goldman-Cecil Medicine | Bradley and Daroff's Neurology in Clinical Practice | Textbook of Family Medicine 9e | Campbell's Operative Orthopaedics 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.