Deviated nasal septum from basics to clinical
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"deviated nasal septum" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the content needed to write a comprehensive, clinically rich response. Let me compile the full answer:
Deviated Nasal Septum (DNS): Basics to Clinical
1. Anatomy of the Nasal Septum
The nasal septum is the midline partition dividing the nasal cavity into two chambers. It is composed of three parts:
Bony septum (posterior/superior):
- Perpendicular plate of ethmoid (superior)
- Vomer (posteroinferior)
- Maxillary crest and palatine bones (most posterior floor)
- Nasal process of the frontal bone (superoanteriorly)
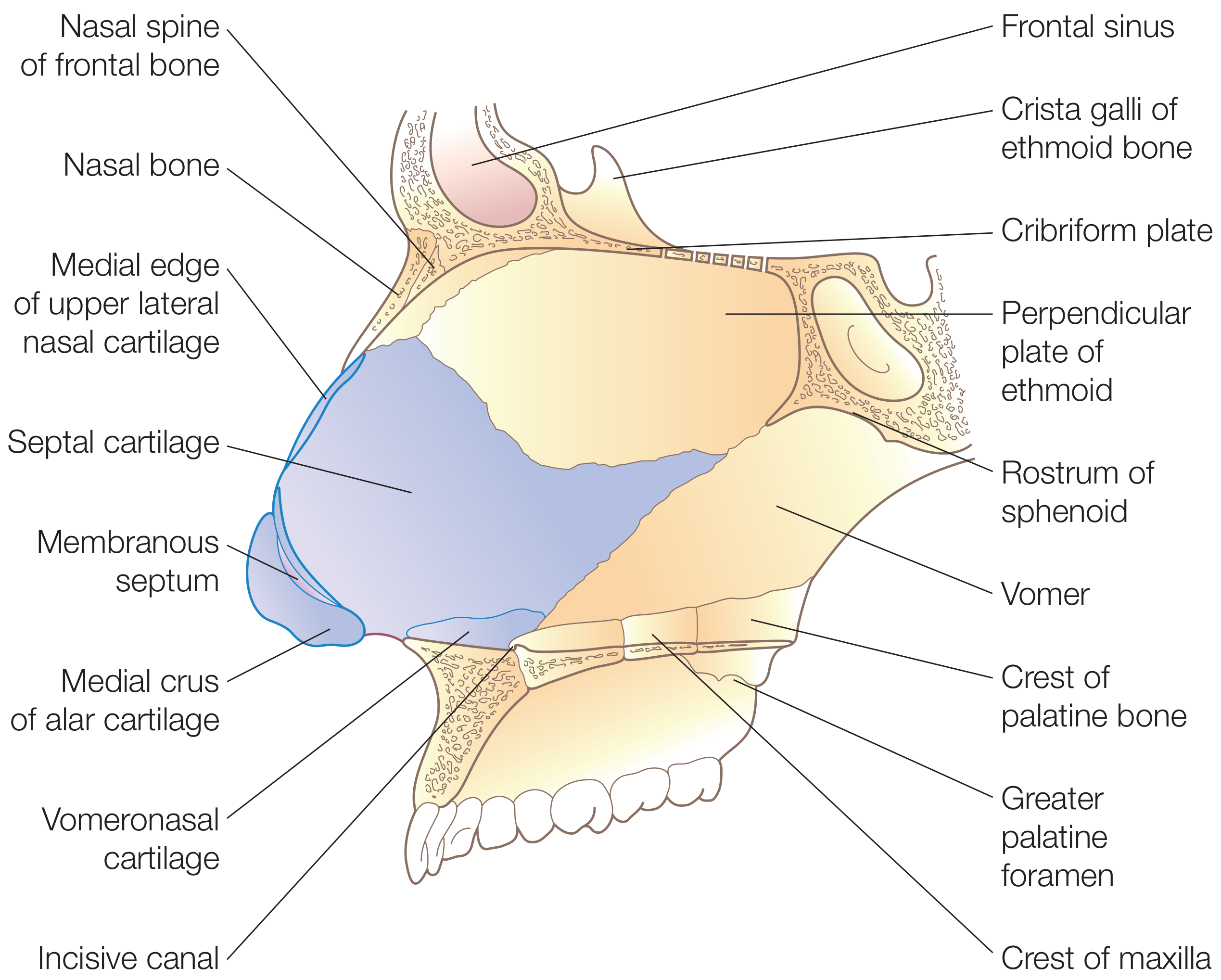
Cartilaginous septum (anterior):
- Quadrilateral cartilage (the main septal cartilage)
- Crucially, the cartilaginous septum is not an isolated structure - it is fused with the upper lateral cartilages (ULCs), forming one cartilaginous unit
Membranous septum (caudal):
- A segment of connective tissue between the caudal edge of the septal cartilage and the columella
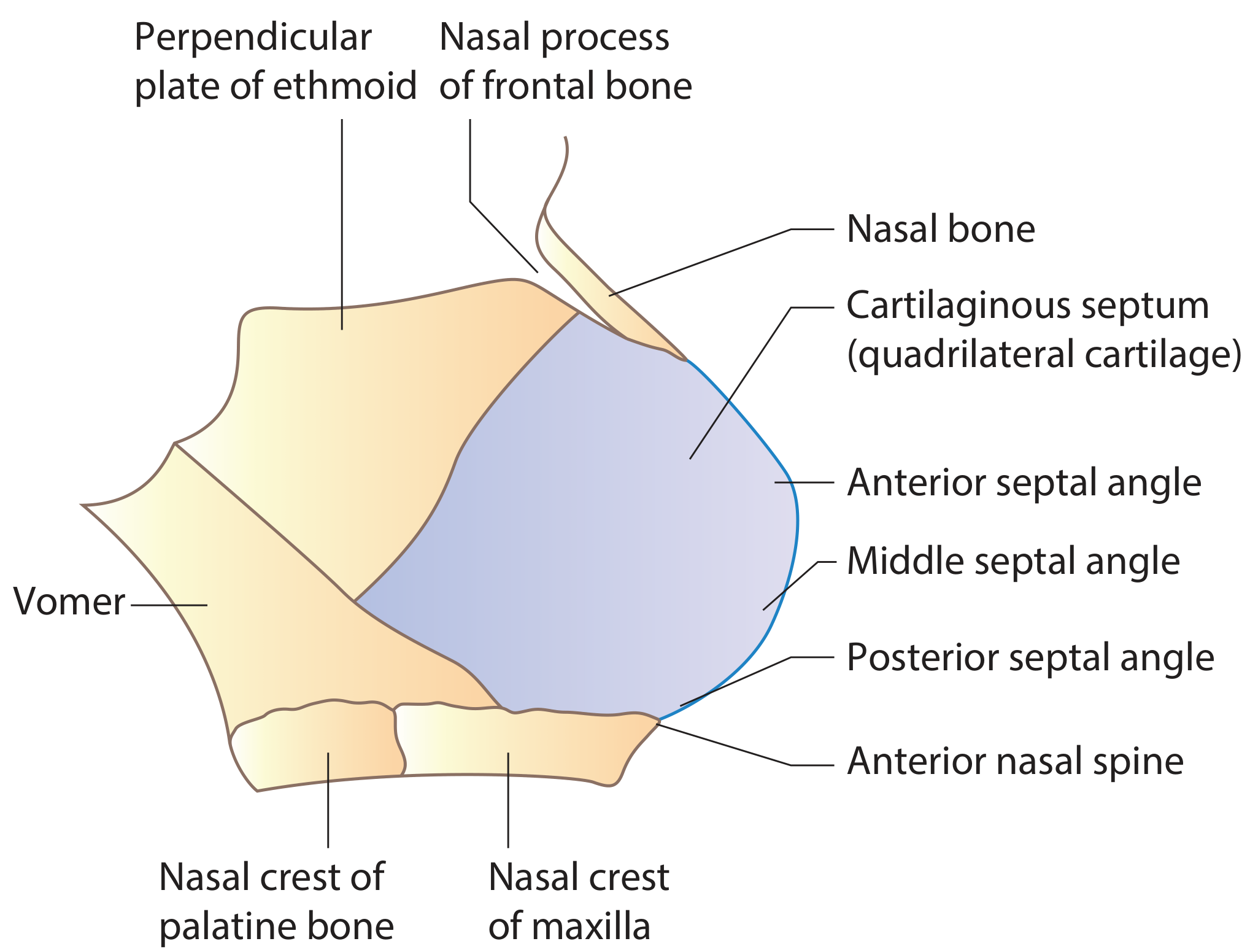
Nasal septal anatomy with terminology - Scott-Brown's Otorhinolaryngology
Cartilaginous and bony components of the nasal septum - Scott-Brown's Otorhinolaryngology
The L-Strut
An L-shaped strut of approximately 1 cm width along the dorsal and caudal margins of the quadrilateral cartilage is the structural backbone of the external nasal skeleton. This concept is surgically critical - any operation that violates the L-strut risks nasal collapse.
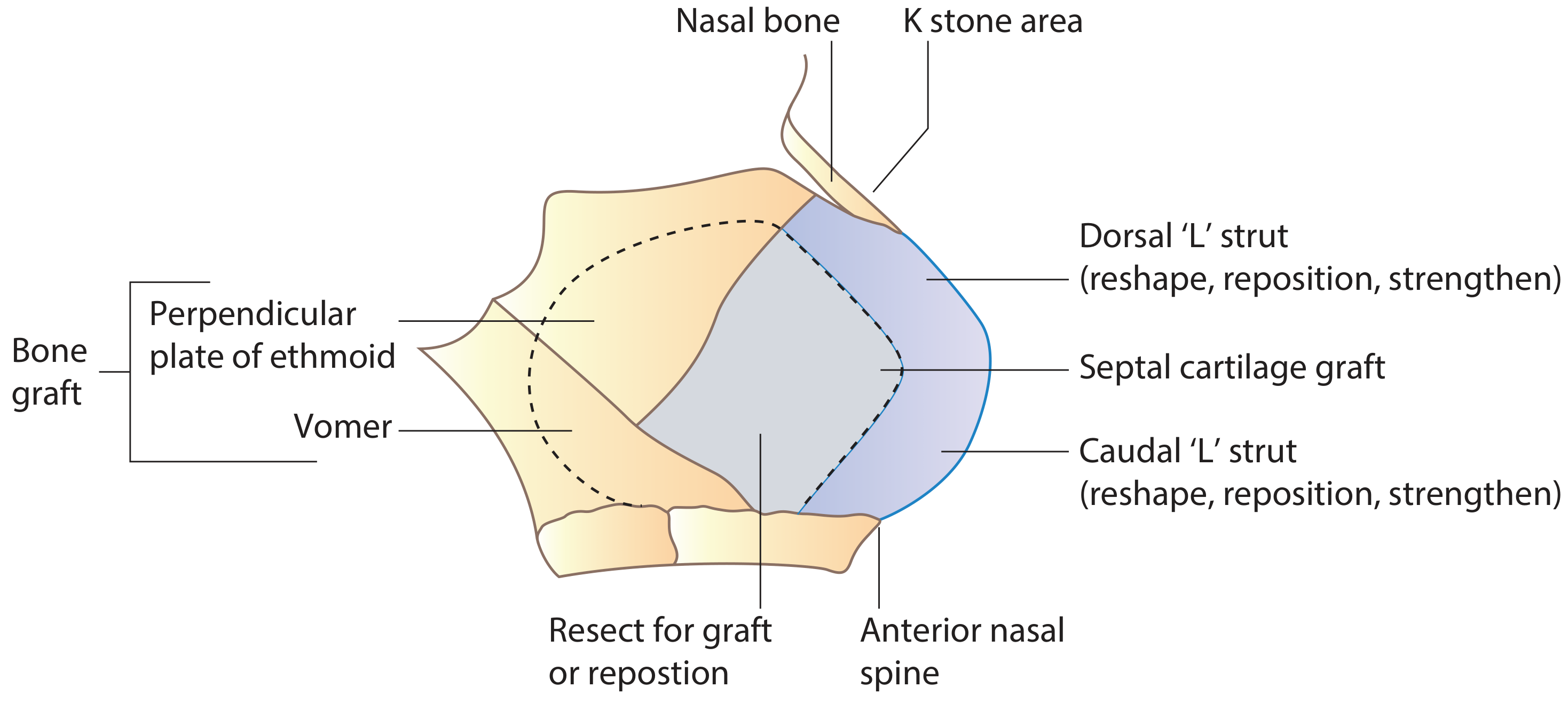
Septal cartilaginous L-strut (minimum 10mm) preserved for structural support. The rest of the septum can be resected or used as graft - Scott-Brown's Otorhinolaryngology
Blood Supply
Both the external and internal carotid arteries supply the septum:
- External carotid: Sphenopalatine artery (posteroinferior septum via posterior septal artery - the basis of the nasoseptal flap for skull base reconstruction) and greater palatine artery (anteroinferior via incisive canal)
- Internal carotid: Anterior and posterior ethmoid arteries (branches of the ophthalmic artery - anterosuperior and posterosuperior septum)
- Facial artery: Septal branch of superior labial artery (caudal septum and columella)
Kiesselbach's plexus (Little's area): The anterior ethmoid artery, posterior septal artery, and superior labial septal branch converge on the anteroinferior septum - the most common site of epistaxis.
Septal Swell Body
A widened region of the anterior septum anterior to the middle turbinate at the internal nasal valve, histologically rich in venous sinusoids. It modulates nasal airflow similar to the inferior turbinates.
2. Nasal Valve
The internal nasal valve is the narrowest segment of the nasal airway and the dominant source of nasal resistance. Its angle (10-15 degrees in white patients, wider in non-whites) is bounded by:
- Medially: the nasal septum
- Laterally: the inferior edge of the upper lateral cartilages (ULCs)
- Inferiorly: the anterior aspect of the inferior turbinate
The external nasal valve is the laterally based area at the piriform aperture, bounded by the ULC, lower lateral cartilage (LLC), and soft tissue of the ala.
Any septal deviation impinging on the internal nasal valve is surgically more significant because even a small narrowing dramatically increases airway resistance (Poiseuille's law - resistance is proportional to the inverse of the radius to the fourth power).
3. Aetiology of DNS
DNS may be:
- Developmental/congenital: Intrinsic growth asymmetry of septal cartilage vs. surrounding bony skeleton. Birth trauma (forceps delivery or passage through the birth canal) is a recognized early cause
- Traumatic: Nasal or midfacial trauma (most common in adults). The trauma may have occurred in childhood with no recollection by the patient
- Iatrogenic: Post-surgical distortion
The deviation may involve the cartilage, bone, or both, and may present at different anatomic regions (caudal, dorsal, body, posterior bony spur).
4. Types/Classification of DNS
Septal deviations are described by:
| Type | Description |
|---|---|
| C-shaped (simple) | Curved deviation to one side |
| S-shaped | Bilateral deviation (nasal obstruction on both sides) |
| Caudal dislocation | Caudal septum displaced off the maxillary crest/anterior nasal spine |
| Posterior bony spur | Sharp bony projection from vomer/maxillary crest causing point obstruction |
| High dorsal deviation | Impinges on the internal nasal valve - most functionally significant |
| Horizontal shelf | Flat horizontal plate of deviation |
Clinically, the most important distinction is whether the L-strut is involved, as this dictates surgical approach (submucosal resection vs. full septoplasty with reconstruction).
5. Clinical Features
Symptoms
- Nasal obstruction - typically unilateral but can be bilateral (e.g., S-shaped deformity, or compensatory inferior turbinate hypertrophy on the contralateral side)
- Constant obstruction suggests anatomical/structural cause; intermittent obstruction suggests mucosal/inflammatory cause
- Epistaxis - turbulent airflow over the deviated area dries mucosa
- Snoring / obstructive sleep apnea - from increased nasal resistance
- Hyposmia - if the olfactory area is compromised
- Headache / sinus pain - mucosal contact point headaches (when deviated septum contacts the lateral nasal wall/turbinate)
- Recurrent sinusitis - obstruction of the sinus drainage pathways
- Mouth breathing - especially nocturnal
Paradoxical Nasal Obstruction
A counter-intuitive phenomenon: the patient perceives the larger, open side as obstructed. This occurs because the nasal cycle shifts, and the mucosal lining on the wide side swells, causing perceived obstruction. Patients can be shown an endoscopic image or tested after decongestion to demonstrate the true anatomy.
6. Examination
External Examination
- Assess nasal symmetry, skin, external nasal valve, tip position (tip ptosis worsens obstruction)
- Deviated external nose often accompanies a septal deviation
Clinical photo: Deviated nose before (A) and after (B) septoplasty alone - demonstrating that septoplasty can correct external nasal deviation

Internal Examination (Anterior Rhinoscopy)
- Map the position of the deviation relative to the L-strut
- Look for: caudal deviation, posterior spurs (easily missed without posterior examination), turbinate hypertrophy, polyps, masses
Nasal Valve Assessment
- Cottle maneuver: Lateral cheek traction to widen the nasal valve - positive if breathing improves. However, many false-positives due to bulk tissue movement.
- Modified/more specific test: Gentle lateralization of the ULC with a cotton-tipped applicator or cerumen curette - a positive test predicts benefit from spreader grafts.
- Dynamic nasal wall collapse on forced inspiration should be noted.
Nasendoscopy (Rigid/Flexible)
- Assess the full nasal cavity, posterior spur, choanae, adenoids, polyps, sinonasal pathology
- No surprises should occur at the time of surgery due to inadequate preoperative assessment
Palpation
- Feel for attachment to the anterior nasal spine, fracture lines
- In revision cases, an applicator probe identifies cartilage-deficient areas
Objective Measurement
- Rhinomanometry: Measures trans-nasal airflow and pressure. Results before and after decongestion distinguish mucosal hypertrophy from structural deformity
- Acoustic rhinometry: Cross-sectional area measurements
- NOSE Scale (Nasal Obstruction Symptom Evaluation): Validated patient-reported outcome tool - five domains (0-4 each), multiplied by 5, max score 100
7. Imaging
CT scan of the paranasal sinuses (coronal cuts) is the investigation of choice when:
- Sinusitis is suspected
- Preoperative planning for complex deviations
- Endoscopic sinus surgery is anticipated alongside septoplasty
CT identifies the level and nature of the deviation, identifies spurs, assesses turbinate pathology, and reveals sinus disease.
8. Treatment
Conservative (Non-Surgical)
- Indicated when symptoms are mild or mucosal inflammation is the dominant cause
- Intranasal corticosteroids - reduce turbinate hypertrophy, improve nasal airflow
- Nasal saline irrigation - mucosal hygiene
- Antihistamines / decongestants - for concurrent allergic rhinitis
- A 2025 systematic review and meta-analysis (PMID: 39230606) directly compared septoplasty vs. non-surgical management - surgical treatment provided superior outcomes for nasal obstruction.
Surgical Treatment
Surgery is indicated when symptoms are significant, constant, and structural. Two main procedures:
a. Submucosal Resection (SMR)
The older procedure, now largely replaced by septoplasty. Involves resecting the deflected cartilaginous and bony septum beneath the mucosal flaps while preserving the perichondrium. Limitation: Cannot adequately address L-strut deviations and risks structural collapse. Provides good graft material.
b. Septoplasty
The modern standard. Emphasizes reconstruction rather than resection - straightening, repositioning, and reinforcing the septum while preserving structural integrity.
Incisions:
- Hemitransfixion incision - at the caudal edge of the septum. Full hemitransfixion accesses the entire septum including the caudal L-strut; partial hemitransfixion suffices for less extensive deviations; extended hemitransfixion provides access to the nasal floor.
- The mucosal flap is usually raised on the concave side only (reduces risk of perforation by keeping contralateral mucosa intact). For S-shaped deformities, bilateral flaps are needed.
Four main surgical techniques (used alone or in combination):
| Technique | Description |
|---|---|
| Cutting (Scoring) | Scoring the concave side allows the septum to spring to midline; scar tissue stabilizes it. Unreliable alone - often combined with splinting. For caudal deviation: "swinging door" - excise excess caudal L-strut, suture back to anterior nasal spine. |
| Grafting | Harvested septal cartilage used as batten grafts, spreader grafts, or columellar struts to reinforce weakened areas |
| Suturing | Mattress/quilting sutures to straighten and fix the septum, reduce dead space, prevent hematoma |
| Relocating | Excision and reinsertion (extracorporeal septoplasty) for severely deviated segments; the cartilage is removed, straightened ex vivo, and replaced |
Extracorporeal septoplasty is reserved for complex cases where in situ correction is inadequate.
Endoscopic septoplasty offers improved visualization, especially for posterior spurs and targeted areas.
Paediatric septoplasty is controversial - generally deferred until growth is complete (late teens) to avoid disturbing septal growth centers, though significant airway compromise is a relative indication earlier.
9. Concurrent Procedures
Inferior turbinate reduction is commonly performed alongside septoplasty because compensatory hypertrophy of the contralateral inferior turbinate often develops. Options include:
- Submucous resection of the conchal bone
- Microdebrider reduction
- Radiofrequency ablation
- Modified Mabry technique (incision on undersurface, conservative resection preserving mucosa)
Preserving turbinate function is essential to prevent empty nose syndrome - a debilitating condition of paradoxical obstruction and dryness from excessive turbinate removal.
Septorhinoplasty combines septoplasty with rhinoplasty when external nasal deviation accompanies the septal problem. Notably, septoplasty alone often corrects external deviation significantly, so osteotomies should never be performed before first straightening the septum.
10. Postoperative Care
- Light non-adherent nasal packing (or none) with a quilting stitch (5-0 plain) to prevent hematoma
- Saline flushing 4x daily after pack removal
- Antibiotic ointment to vestibule from 24 hours post-op
- Gentle suctioning days 5-10
- No nose blowing for 3 weeks; no strenuous exercise for 6 weeks
- Internal silastic splints only in specific cases (perforation repair, excoriated mucosa)
11. Complications
| Complication | Notes |
|---|---|
| Persistent nasal obstruction | Most common - often due to inadequate addressing of posterior bony spur |
| Septal hematoma | Failure to use quilting suture; presents as bluish/fluctuant midline swelling; risk of perichondrial necrosis and cartilage collapse if untreated |
| Septal perforation | From unrepaired bilateral mucoperichondrial tears; presents with whistling, crusting, epistaxis |
| Nasal saddling / dorsal collapse | Over-resection of dorsal strut or loss of L-strut support |
| Tip ptosis | Over-resection of caudal strut |
| Synechiae (intranasal adhesions) | Between septum and turbinate; especially with traumatic suturing technique |
| Infection | Rare; risk increased by hematoma |
| Rhinorrhea | May persist months postoperatively |
| Anosmia | Rare; if olfactory epithelium is disrupted |
12. Recent Evidence
A 2025 systematic review and meta-analysis of RCTs (PMID: 39230606) confirmed that septoplasty provides superior improvement in nasal obstruction compared to non-surgical management, supporting surgery as the definitive treatment for symptomatic structural DNS.
A 2024 systematic review (PMID: 39323198) found that sphenopalatine ganglion block provides effective postoperative pain control after septoplasty.
Summary Table
| Feature | Detail |
|---|---|
| Definition | Displacement of the nasal septum from the midline |
| Most common cause | Trauma (adults); birth trauma/developmental (children) |
| Key anatomy | Perpendicular plate of ethmoid + vomer (bone); quadrilateral cartilage (cartilage); membranous (caudal) |
| Most critical structure | L-strut (10 mm dorsal + caudal margins) |
| Key symptom | Unilateral nasal obstruction (constant = structural) |
| Paradoxical obstruction | Wider side perceived as blocked due to turbinate cycle |
| Diagnosis | Clinical (anterior rhinoscopy + nasendoscopy); CT if sinus disease suspected |
| Conservative Rx | Topical steroids, saline irrigation, antihistamines |
| Definitive Rx | Septoplasty (reconstruction-focused) |
| Key complication | Septal hematoma (emergency), saddle nose (chronic) |
Sources: Cummings Otolaryngology Head and Neck Surgery, 6th Ed. | Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1 | Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.