Now I have all the material I need. Let me compile the topper-level USMLE notes.
Type 1 (Distal) RTA - Topper-Level USMLE Notes
THE CORE DEFECT
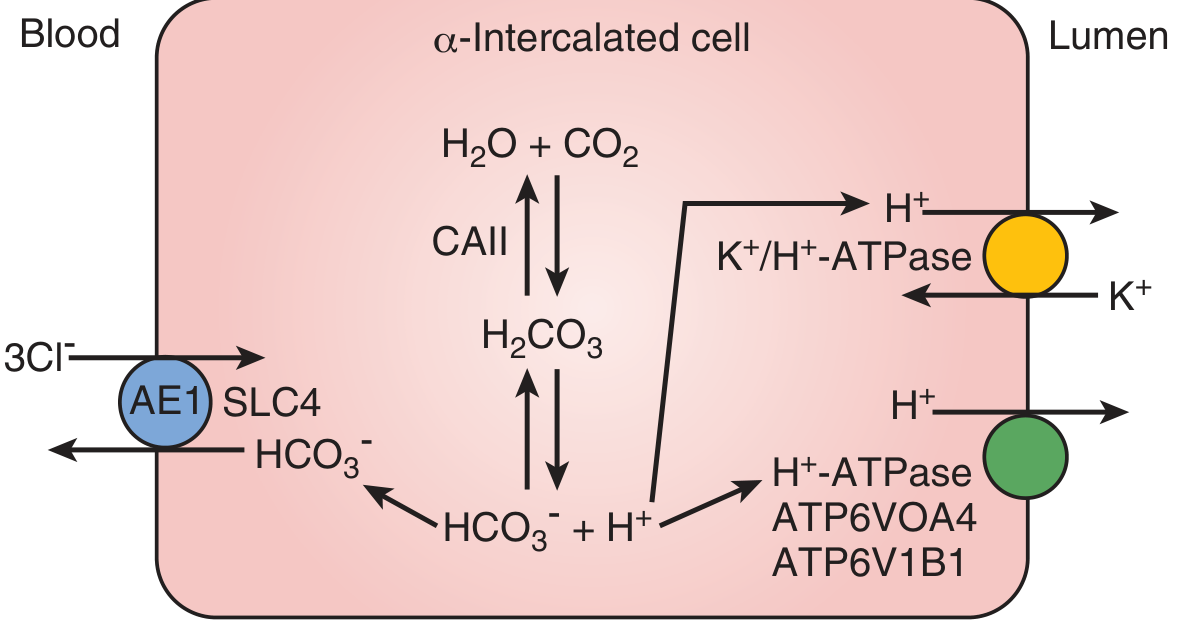
The alpha-intercalated cells of the collecting duct fail to secrete H+ into the tubular lumen. These cells normally use two apical pumps - H+-ATPase (ATP6V0A4/ATP6V1B1) and H+/K+-ATPase - to drive a 1000:1 H+ gradient that can acidify urine down to pH 4.5. The basolateral AE1 (SLC4A1) Cl-/HCO3- exchanger simultaneously recovers HCO3- into blood. When any of these fail, urine pH is stuck above 5.5 permanently.
Genes to know:
- SLC4A1 → AE1 exchanger defect → autosomal dominant dRTA
- ATP6V1B1 / ATP6V0A4 → H+-ATPase subunit defects → autosomal recessive dRTA + sensorineural deafness
- CA2 → carbonic anhydrase II defect → mixed proximal + distal RTA
THE PATHOGNOMONIC PARADOX (High-Yield)
| Finding | Direction | Explanation |
|---|
| Blood pH | ↓ (acidotic) | H+ retention, HCO3- loss |
| Serum HCO3- | ↓ (often severe, pH ~7.2) | Continuous acid retention |
| Urine pH | > 5.5 always | Cannot acidify despite acidosis |
| Serum Cl- | ↑ (hyperchloremic) | Non-anion gap MA |
| Anion gap | Normal | Hyperchloremic compensation |
| Serum K+ | ↓ | See mechanism below |
The paradox: Systemic acidosis with alkaline urine. Every other cause of metabolic acidosis produces urine pH < 5.5 (kidneys compensate). Type 1 RTA cannot. Urine pH > 5.5 despite metabolic acidosis = pathognomonic.
STONE FORMATION - THE TRIPLE THREAT
Three simultaneous factors drive nephrolithiasis (stones in ~70% of patients):
1. Alkaline urine (pH > 5.5)
Calcium phosphate (CaHPO4 - brushite) crystallizes preferentially in alkaline urine. Struvite forms here too. Uric acid and calcium oxalate prefer acidic urine - a common trap.
2. Hypercalciuria
Chronic metabolic acidosis buffers H+ in bone → demineralizes bone → secondary hyperparathyroidism → hypercalciuria. Calcium floods the urine.
3. Hypocitraturia (arguably the most important factor)
Metabolic acidosis increases proximal tubule reabsorption of citrate. Intracellular acidosis also drives citrate into mitochondria. Citrate normally chelates calcium and inhibits crystallization - without it, stones form readily. This is the most important stone risk factor in Type 1 RTA.
Nephrocalcinosis (calcium deposits in renal parenchyma) is also common and can progress to CKD.
HYPOKALEMIA MECHANISM
Two additive mechanisms:
- Impaired H+ secretion → compensatory K+ secretion: When the alpha-intercalated cell fails to secrete H+, more distal Na+ reabsorption must be paired with K+ secretion instead (principal cells increase K+ loss to maintain electroneutrality).
- Volume depletion → secondary hyperaldosteronism: Chronic metabolic acidosis increases Na+ and water delivery to the distal nephron → volume depletion → aldosterone surge → further K+ wasting.
This is why Type 1 and Type 2 RTA both cause hypokalemia, while Type 4 RTA causes hyperkalemia (hypoaldosteronism).
RTA COMPARISON TABLE (Classic Exam Killer)
| Feature | Type 1 (Distal) | Type 2 (Proximal) | Type 4 |
|---|
| Defect | H+ secretion in CD | HCO3- reabsorption in PCT | Hypoaldosteronism |
| Urine pH | > 5.5 always | > 5.5 only with HCO3- load; < 5.5 at steady state | < 5.5 |
| Serum K+ | ↓ | ↓ | ↑ |
| Anion gap | Normal | Normal | Normal |
| HCO3- level | Often very low | Mildly low (stable) | Mildly low |
| Stones | Yes (CaPO4) | No | No |
| Nephrocalcinosis | Yes | No | No |
| Key associations | Sjögren, SLE, amphotericin B | Multiple myeloma, Fanconi syndrome, tenofovir | DM, ACEi/ARB, K+-sparing diuretics, Addison's |
EXAM TRAP: Stone Type vs. Urine pH
| Urine pH | Stone Type |
|---|
| Alkaline | Calcium phosphate, Struvite (triple phosphate) |
| Acidic | Uric acid, Cystine |
| Either | Calcium oxalate (most common overall) |
Students assume all stones come from acidic urine. The exam tests the reverse: Type 1 RTA makes urine too alkaline, which crystallizes calcium phosphate and causes nephrocalcinosis.
DIAGNOSIS
- Spontaneous urine pH > 5.5 in setting of metabolic acidosis rules in Type 1 RTA
- If urine pH < 5.5, Type 1 RTA is ruled out (Goldman-Cecil Medicine)
- Urine AG (Na+ + K+ - Cl-) is positive → indicates impaired NH4+ excretion (normally NH4+ carries Cl-, so NH4+ loss makes urine Cl- fall and UAG goes positive)
- If diagnosis uncertain: give NH4Cl load or furosemide 40 mg - urine pH should fall below 5.5 in normal kidneys; failure to do so confirms Type 1 RTA
TREATMENT
- Sodium bicarbonate or sodium citrate - replaces daily acid load (adults need ~1-2 mEq/kg/day; children need more due to growth)
- Potassium citrate preferred when hypokalemia is present - corrects both K+ deficit and hypocitraturia simultaneously, preventing stones
- Correcting acidosis usually corrects hypokalemia automatically; some patients need chronic K+ supplementation
- NaHCO3 requirements in Type 1 RTA are small (1-3 mEq/kg/day) vs. Type 2 (requiring massive doses because the kidney keeps spilling HCO3-)
HIGH-YIELD ASSOCIATIONS
- Sjögren syndrome - most classic secondary cause of Type 1 RTA (also associated with Type 2)
- Systemic lupus erythematosus
- Amphotericin B - creates pores in tubular cells, leaks H+ back
- Hereditary elliptocytosis, sickle cell anemia - red cell membrane AE1 mutations extend to renal AE1
- Obstructive uropathy, chronic pyelonephritis
- Autoimmune thyroiditis, primary biliary cholangitis
ONE-LINER FOR VIGNETTES
Middle-aged woman with Sjögren syndrome, metabolic acidosis (pH 7.28, HCO3- 14), urine pH 6.5, hypokalemia, and calcium phosphate kidney stones = Type 1 (Distal) RTA. Treat with potassium citrate.
Sources: Campbell-Walsh-Wein Urology; Goldman-Cecil Medicine; Frameworks for Internal Medicine; Henry's Clinical Diagnosis and Management by Laboratory Methods