I have my university exam of 1 st year of subject physiology These are the important long answer give me answer of this question "Describe the function of basal ganglia, its connections & abnormalities associated with it." and remeber it's a long question
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full exam answer:
Basal Ganglia: Functions, Connections & Abnormalities
1. INTRODUCTION
The basal ganglia (also called basal nuclei) are a group of deeply situated subcortical masses of grey matter within the telencephalon and diencephalon. They form an important part of the extrapyramidal motor system and play a key role in the planning and execution of smooth voluntary movements, as well as contributing to cognitive and affective functions.
2. COMPONENTS / ANATOMY
The basal ganglia consist of five interactive structures on each side of the brain (Ganong's, p. 251):
| Structure | Details |
|---|---|
| Caudate nucleus | C-shaped nucleus forming the medial wall of the lateral ventricle |
| Putamen | Lateral to the globus pallidus |
| Globus pallidus | Divided into external (GPe) and internal (GPi) segments; both use GABA |
| Subthalamic nucleus | In the diencephalon; uses glutamate (excitatory) |
| Substantia nigra | In the midbrain; divided into: - Pars compacta (SNpc) - uses dopamine - Pars reticulata (SNpr) - uses GABA |
Important groupings:
- Striatum = Caudate nucleus + Putamen (receives most cortical input)
- Lenticular nucleus = Putamen + Globus pallidus
- About 95% of striatal neurons are medium spiny neurons (GABAergic); remaining are aspiny interneurons using acetylcholine, somatostatin, or GABA.
3. CONNECTIONS OF THE BASAL GANGLIA
The basal ganglia operate through a cortical-basal ganglia-thalamic-cortical loop.
Inputs to Basal Ganglia
There are two major excitatory (glutamatergic) inputs to the striatum:
- Corticostriatal pathway - from a wide region of cerebral cortex (especially motor cortex)
- Thalamostriatal pathway - from the intralaminar nuclei of the thalamus
Outputs from Basal Ganglia
Both major outputs are inhibitory (GABAergic) and project to the thalamus:
- From GPi (internal globus pallidus)
- From SNpr (substantia nigra pars reticulata)
From the thalamus, an excitatory (glutamatergic) projection goes to the prefrontal and premotor cortex (completing the loop).
The Two Main Pathways: Direct & Indirect
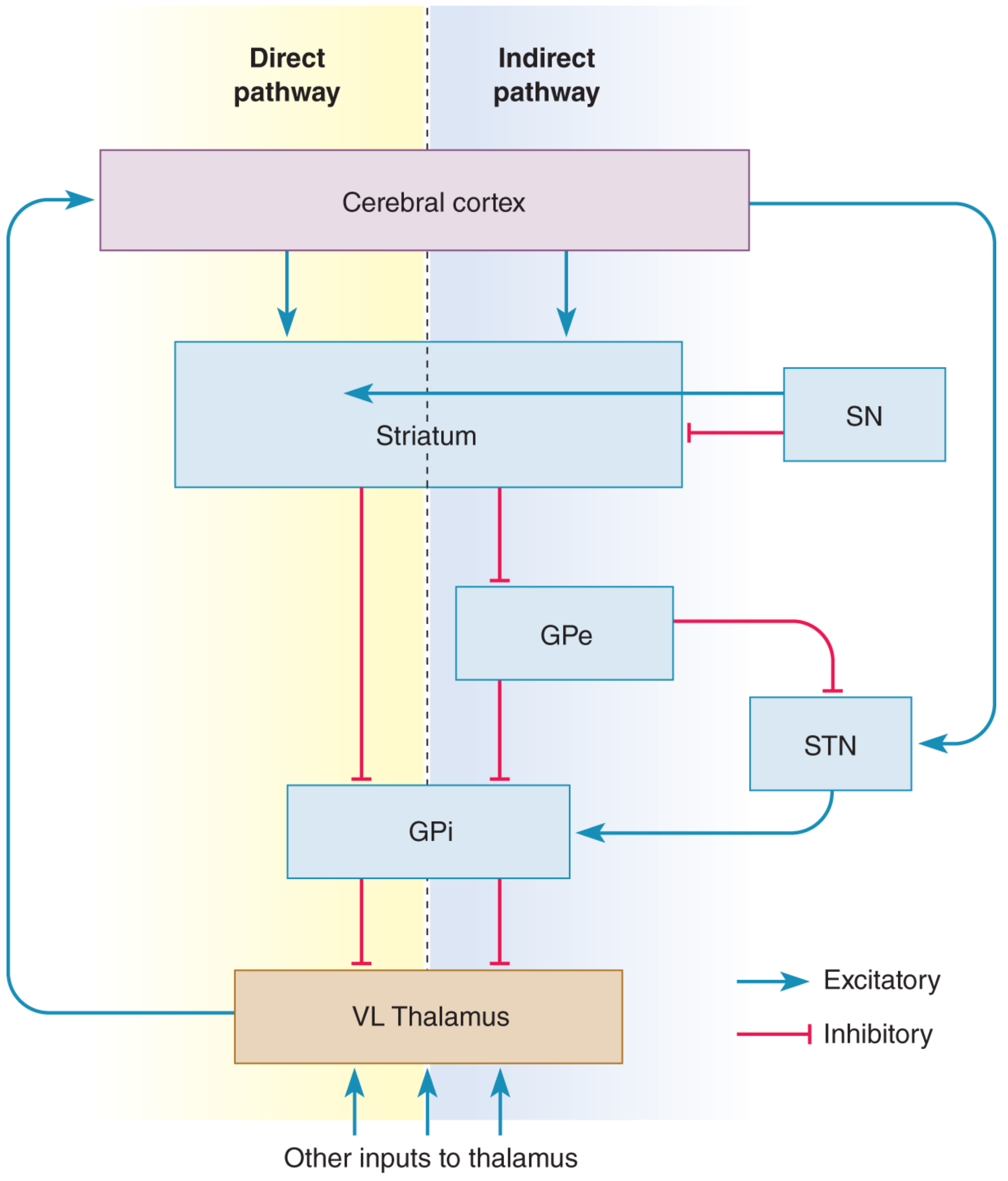
(Fig. 14.15 - Neuroscience: Exploring the Brain, 5th Ed. Blue = Excitatory; Red = Inhibitory)
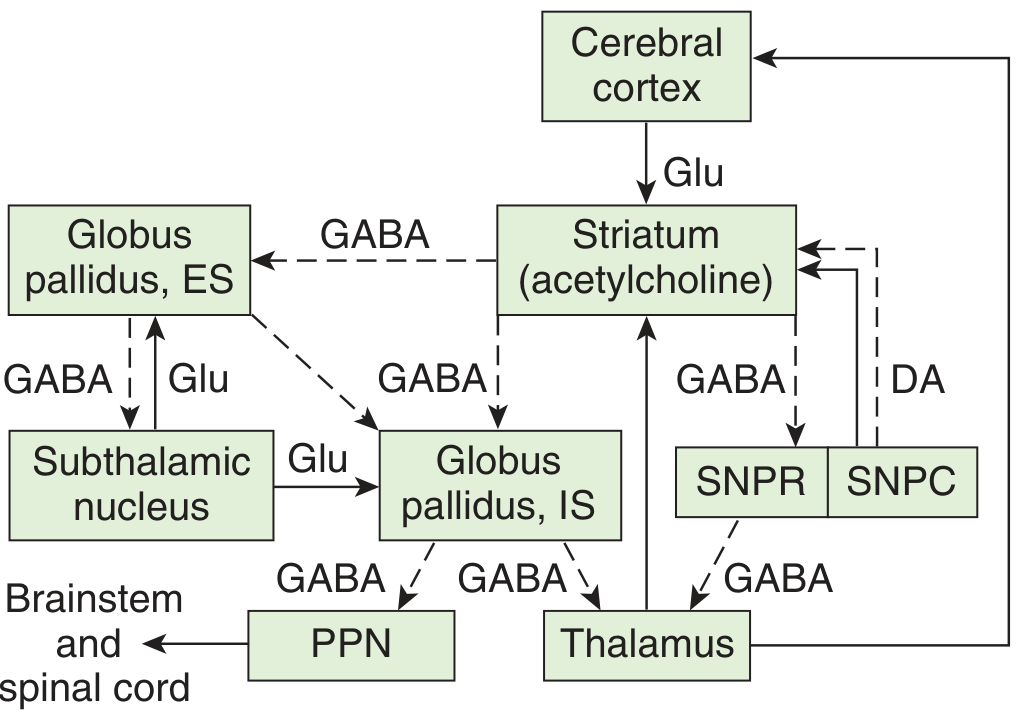
(Fig. 12-14 - Ganong's Review of Medical Physiology. Solid = Excitatory; Dashed = Inhibitory. DA = dopamine; Glu = glutamate)
A. Direct Pathway (Net Effect: EXCITATORY on motor cortex - facilitates movement)
Route: Cortex → Striatum → GPi/SNpr → Thalamus (VL) → Motor Cortex (SMA)
Step by step:
- Cerebral cortex sends excitatory (Glu) input to the striatum (putamen)
- Striatum sends inhibitory (GABA) input to the GPi/SNpr
- This inhibits the GPi (which was tonically inhibiting the thalamus)
- Thalamus (VL nucleus) is released from inhibition → becomes active
- Thalamus sends excitatory (Glu) signals back to the motor cortex (SMA)
Net result: Cortex → Striatum inhibits GPi → GPi releases VL thalamus → VL excites cortex. The double negative becomes a positive - movement is facilitated ("Go" signal).
B. Indirect Pathway (Net Effect: INHIBITORY on motor cortex - suppresses movement)
Route: Cortex → Striatum → GPe → Subthalamic Nucleus → GPi → Thalamus (VL) → Motor Cortex
Step by step:
- Cerebral cortex sends excitatory (Glu) input to the striatum
- Striatum sends inhibitory (GABA) to GPe (external globus pallidus)
- GPe's inhibitory output to the subthalamic nucleus (STN) is reduced - STN is released from inhibition
- STN sends excitatory (Glu) output to GPi/SNpr
- GPi becomes more active and sends more inhibitory GABA to thalamus
- Thalamus is more inhibited → less excitation of motor cortex
Net result: Movement is suppressed ("No-go" signal). Indirect pathway antagonizes direct pathway and suppresses competing/unwanted motor programs.
The direct pathway (excitatory output) and indirect pathway (inhibitory output) are balanced. Any disturbance upsets this balance - causing either too much or too little movement.
C. Dopaminergic Nigrostriatal Connection (Modulatory Loop)
The substantia nigra pars compacta (SNpc) projects dopaminergic fibers back to the striatum via the nigrostriatal pathway. Dopamine has a dual effect:
- Acts on D1 receptors on direct-pathway neurons → facilitates the direct pathway (promotes movement)
- Acts on D2 receptors on indirect-pathway neurons → inhibits the indirect pathway (further promotes movement)
Overall effect of dopamine: promotes movement initiation.
4. FUNCTIONS OF THE BASAL GANGLIA
| Function | Details |
|---|---|
| Motor planning & execution | Basal ganglia neurons discharge before movements begin; they help plan and program movement |
| Converting thought to action | They help convert abstract thought into voluntary motor action |
| Smooth movement | Aid in the execution of smooth, coordinated voluntary movements |
| Action selection | The direct pathway selects desired motor actions; indirect pathway suppresses competing/unwanted motor programs |
| Cognitive functions | The caudate nucleus plays a role in cognitive processes (object reversal, delayed alternation tasks) |
| Limbic/Affective | Connected to the amygdala and prefrontal cortex; involved in motivation, emotional regulation, and reward-based learning |
| Scaling of movement | Help scale the amplitude and velocity of movements |
(Costanzo Physiology, 7th Ed., p. 3469; Ganong's, p. 252; Neuroscience: Exploring the Brain, 5th Ed., p. 1352)
5. DISEASES / ABNORMALITIES OF THE BASAL GANGLIA
Three biochemical pathways normally operate in balance:
- Nigrostriatal dopaminergic system
- Intrastriatal cholinergic system
- GABAergic system (striatum → globus pallidus/substantia nigra)
When any one becomes dysfunctional, characteristic motor disorders occur. These fall into two broad categories:
| Category | Features | Examples |
|---|---|---|
| Hypokinetic | Decreased/absent movement | Parkinson's disease (akinesia, bradykinesia) |
| Hyperkinetic | Excessive/abnormal movement | Huntington's (chorea), Hemiballismus, Athetosis |
A. Parkinson's Disease (Hypokinetic)
Pathology: Degeneration of dopaminergic neurons in the substantia nigra pars compacta (SNpc) - the fibers to the putamen are most severely affected. First described by James Parkinson in 1817.
Mechanism:
- Loss of dopamine → D1 receptors on direct pathway are NOT stimulated → GPi is NOT inhibited → thalamus is overly inhibited → motor cortex receives less excitation → hypokinesia
- Loss of dopamine → D2 receptors on indirect pathway are NOT inhibited → indirect pathway is overactive → GPi receives more excitation → thalamus is even more inhibited → worse hypokinesia
- Net: the balance is shifted toward excess inhibition of thalamus and motor cortex
Clinical Features (tetrad):
- Tremor at rest - "pill-rolling" tremor, 4-8 Hz, disappears with voluntary movement (unlike cerebellar intention tremor)
- Rigidity - "lead pipe rigidity" (resistance to both flexion and extension); "cogwheel rigidity" (with superimposed tremor)
- Bradykinesia - slowness of all movements
- Akinesia - difficulty initiating voluntary movements; loss of postural reflexes; festinant gait, masked face, reduced arm swing
B. Huntington's Disease (Hyperkinetic - Chorea)
Pathology: Early degeneration of medium spiny GABAergic neurons in the striatum (especially those projecting to GPe - the indirect pathway neurons)
Mechanism:
- Loss of GABAergic striatal neurons to GPe → GPe is released from inhibition (disinhibited)
- Over-active GPe inhibits subthalamic nucleus (STN) more
- STN cannot excite GPi → GPi is under-active → thalamus is under-inhibited → motor cortex is over-excited → hyperkinesia (chorea)
Clinical Features:
- Early sign: jerky hand trajectory during reaching
- Choreiform movements - rapid, involuntary, irregular "dancing" movements that gradually worsen
- Progressive dementia
- Slurred speech, then incomprehensible speech
- Death usually within 10-15 years of onset
Genetics: Autosomal dominant; chromosome 4 short arm; CAG trinucleotide repeat expansion (normal: 11-34 repeats; disease: 42-86+ repeats). The gene codes for huntingtin protein. Greater the CAG repeats = earlier onset and more rapid progression.
C. Hemiballismus (Hyperkinetic)
Pathology: Lesion of the subthalamic nucleus (STN), usually due to a small infarct (lacunar stroke)
Mechanism:
- Damage to STN → loss of excitatory drive on GPi
- GPi becomes under-active → thalamus is under-inhibited → over-activation of motor cortex
- Results in violent, involuntary, flailing movements of one entire side of the body
Clinical Features:
- Ballism - violent, large-amplitude, flinging/flailing movements of the limbs ("ball-throwing" type movements)
- Usually affects one side (hemi-ballismus), corresponding to contralateral STN lesion
D. Wilson's Disease (Hepatolenticular Degeneration)
Pathology: Autosomal recessive disorder; mutation of ATP7B gene (chromosome 13q) - a copper-transporting ATPase. Copper accumulates in the liver, brain (especially putamen), and cornea.
Clinical Features:
- "Wing-beating" tremor (asterixis)
- Dysarthria, unsteady gait, rigidity
- Progressive liver damage
- Kayser-Fleischer rings (copper deposits at corneal periphery)
- Onset: age 6-25 years
E. Other Disorders
| Disorder | Key Feature |
|---|---|
| Athetosis | Slow, sinuous, writhing involuntary movements (especially of hands/fingers); due to striatal damage |
| Tardive Dyskinesia | Iatrogenic - caused by long-term use of dopamine-blocking drugs (neuroleptics like haloperidol, phenothiazines); causes uncontrolled involuntary movements of face and tongue; due to D3 receptor hypersensitivity |
6. SUMMARY TABLE: Direct vs. Indirect Pathway
| Feature | Direct Pathway | Indirect Pathway |
|---|---|---|
| Overall effect | Excitatory on cortex (promotes movement) | Inhibitory on cortex (suppresses movement) |
| Route | Striatum → GPi → Thalamus → Cortex | Striatum → GPe → STN → GPi → Thalamus → Cortex |
| Neurotransmitters | GABA (striatum→GPi), Glu (thalamus→cortex) | GABA + Glu + GABA (multiple steps) |
| Dopamine effect | D1 - facilitates (promotes direct pathway) | D2 - inhibits (suppresses indirect pathway) |
| Loss of dopamine | Suppresses movement (less excitation) | Over-activates inhibition (less movement) |
| Parkinson (dopamine loss) | Underactive → less movement | Overactive → less movement (both combine for hypokinesia) |
| Huntington (striatum loss) | Less striatal inhibition on GPi → disinhibits thalamus → more movement (hyperkinesia) |
7. QUICK MNEMONIC AID
Components of Basal Ganglia: "CanPut Good Stuff Sideways"
- Caudate nucleus
- Putamen
- Globus pallidus
- Subthalamic nucleus
- Substantia nigra
Direct = Double-negative = Positive (Go signal)
Indirect = Triple-negative = Negative (No-go signal)
Sources: Ganong's Review of Medical Physiology 26th Ed. (pp. 251-253); Costanzo Physiology 7th Ed.; Neuroscience: Exploring the Brain 5th Ed. (pp. 1352-1357)
This is a shared conversation. Sign in to Orris to start your own chat.