Asprin
Reading File
Asking for Preferences
Finding Sources
Searching the Web
aspirin pharmacology mechanism indications side effects 2024
Reading File
Reading File
Reading File
Searching PubMed
aspirin antiplatelet therapy cardiovascular
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a comprehensive overview of Aspirin (Acetylsalicylic Acid).
Aspirin (Acetylsalicylic Acid) — Full Overview
Chemical Identity
Aspirin is acetylsalicylic acid (ASA), a salicylate derived from willow bark. It belongs to the NSAID class but has unique, irreversible activity that distinguishes it from other members.
Mechanism of Action
Aspirin is a weak organic acid that irreversibly acetylates the serine residue (Ser-530) of cyclooxygenase (COX) enzymes, permanently inactivating them. This blocks the conversion of arachidonic acid (from membrane phospholipids) → prostaglandin H₂ → thromboxane A₂ (TXA₂).
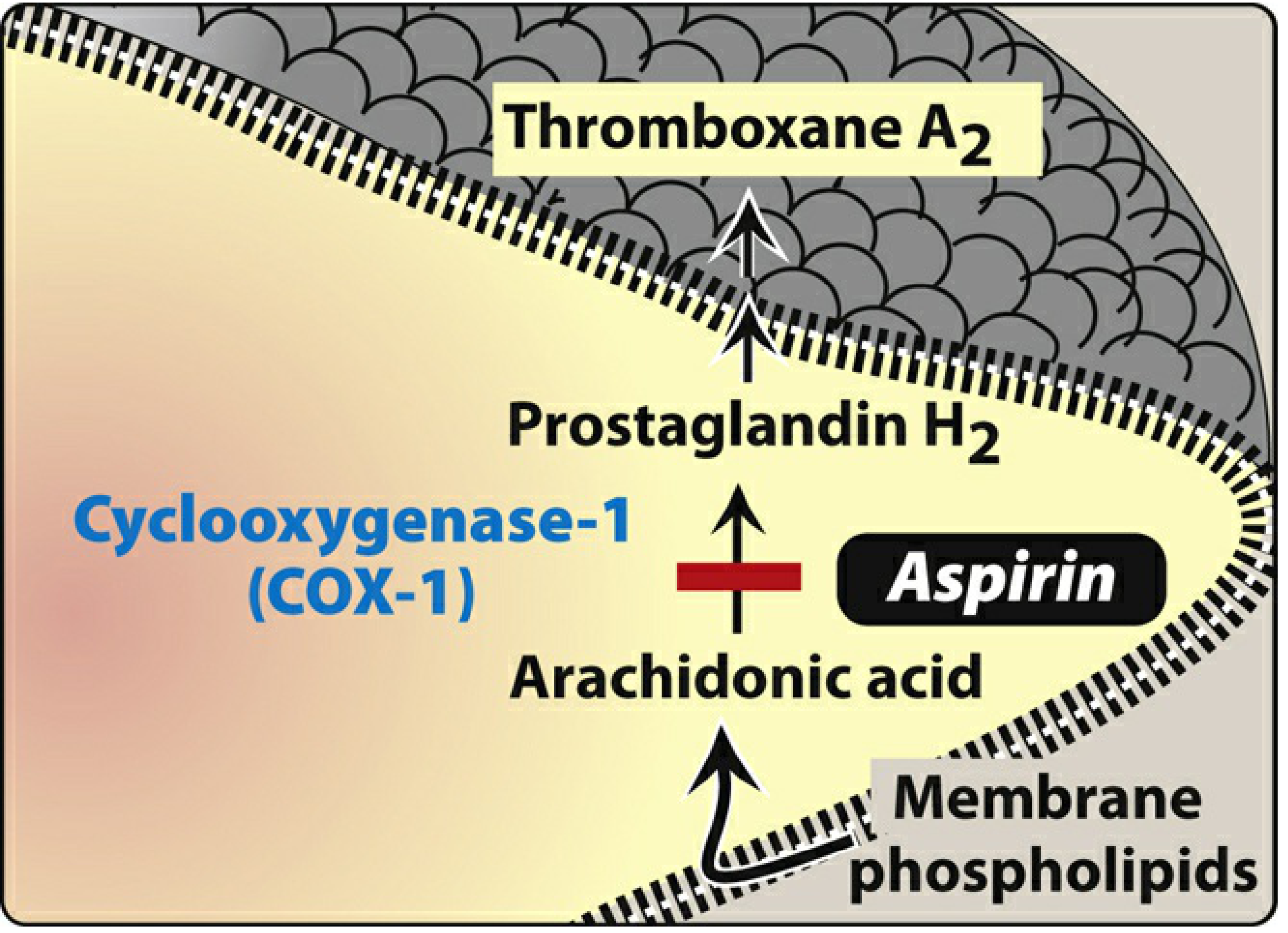
Figure: Aspirin blocks the COX-1 pathway — arachidonic acid → PGH₂ → TXA₂ — in platelets.
COX isoforms affected:
| Dose | COX-1 | COX-2 |
|---|---|---|
| Low (75–325 mg) | Irreversibly inhibited | Minimal effect |
| High (~1 g/day) | Inhibited | Also inhibited (including prostacyclin synthesis in endothelium) |
Because platelets lack nuclei, they cannot regenerate COX. The antiplatelet effect of a single aspirin dose therefore lasts 7–10 days (the platelet lifespan). This is the basis of its antiplatelet potency.
- Lippincott Pharmacology, p. 440; Harrison's 22E, p. [block 13]
Three Core Pharmacological Actions
| Action | Mechanism | Clinical Use |
|---|---|---|
| Anti-inflammatory | ↓ Prostaglandins (mediators of inflammation) | Arthritis, rheumatic fever |
| Analgesic | ↓ PGE₂ → less sensitization of pain receptors | Mild–moderate pain, headache, dysmenorrhea |
| Antipyretic | ↓ PGE₂ in hypothalamus → resets thermostat | Fever reduction |
NSAIDs do NOT affect normal body temperature — antipyretic effect is selective to febrile states.
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Oral; passive diffusion |
| Hydrolysis | Rapidly → salicylic acid (mainly in liver) |
| Half-life (aspirin) | 15–20 minutes |
| Half-life (salicylate) | 3–12 hours (dose-dependent) |
| Protein binding | High (salicylate) |
| Excretion | Renal (pH-dependent); alkaline urine promotes excretion |
Enteric-coated formulations delay absorption but do not eliminate GI side effects.
Clinical Indications
1. Antiplatelet / Cardiovascular
- Secondary prevention of MI, stroke, TIA, and peripheral artery disease: ~25% reduction in cardiovascular death, MI, or stroke
- ACS/STEMI: Load with ≥160 mg non-enteric-coated; maintain 75–100 mg/day
- Post-PCI / post-CABG: Dual antiplatelet therapy (with a P2Y₁₂ inhibitor)
- Primary prevention: No longer routine. Recommended only if 10-year cardiovascular risk ≥10% AND low bleeding risk — recent RCTs show GI/intracerebral hemorrhage risk outweighs benefit in lower-risk individuals
2. Anti-inflammatory / Analgesic
- Rheumatic fever: 4–8 g/day in divided doses
- Osteoarthritis, RA (older use, now largely replaced by other NSAIDs/DMARDs)
- Mild–moderate pain: headache, myalgia, dysmenorrhea
3. Antipyretic
- Fever management in adults (not children — see contraindications)
4. Colorectal Cancer Prevention
- Long-term low-dose aspirin may reduce colorectal cancer risk; also gastric cancer (but increases GI bleeding risk)
Dosing
| Indication | Dose |
|---|---|
| Antiplatelet (maintenance) | 75–100 mg/day |
| Antiplatelet (loading, rapid effect) | 160–325 mg (non-enteric-coated) |
| Analgesic / antipyretic | 325–1000 mg q4–6h |
| Anti-inflammatory (rheumatic fever) | 4–8 g/day in divided doses |
Higher antiplatelet doses are not more effective and carry greater bleeding risk. Some analyses suggest reduced antiplatelet efficacy at higher doses.
Side Effects
Gastrointestinal (most common, dose-related)
- Dyspepsia, nausea
- Erosive gastritis, peptic ulcer
- GI bleeding and perforation
- Major bleeding risk: 1–3% per year
- Enteric-coated/buffered aspirin does not eliminate this risk
- Risk mitigation: PPI co-administration; H. pylori eradication in peptic ulcer patients
Bleeding
- Prolonged bleeding time (irreversible platelet inhibition)
- Risk 2–3× higher with dual antiplatelet therapy (+ clopidogrel/ticagrelor) or anticoagulants (+ warfarin)
Respiratory / Hypersensitivity
- Aspirin-exacerbated respiratory disease (AERD): Bronchospasm in ~0.3% general population; more common in asthmatics, those with nasal polyps/chronic rhinitis
- Universal cross-reactivity with other NSAIDs
- COX-2 inhibitors are generally tolerated in AERD patients
Drug Interactions
- Ibuprofen: Competes at COX-1 catalytic site. If ibuprofen is taken within 2 hours before aspirin, it blocks acetylation → negates antiplatelet effect. Aspirin should be taken ≥60 min before or ≥8 hours after ibuprofen.
- Warfarin / anticoagulants: Significantly increased bleeding risk
- Methotrexate: Aspirin reduces renal clearance → toxicity risk
Contraindications & Cautions
| Contraindication | Reason |
|---|---|
| Children/teenagers with viral illness | Reye syndrome (hepatic encephalopathy) |
| Aspirin allergy / AERD | Bronchospasm risk |
| Active peptic ulcer / GI bleeding | Worsens hemorrhage |
| Severe hepatic or renal impairment | Toxicity risk |
| Pregnancy (≥20 weeks, high doses) | Premature closure of ductus arteriosus |
| Gout (low-dose) | Low-dose aspirin reduces uric acid excretion → can precipitate gout |
Aspirin Resistance
- True pharmacological resistance is rare
- Pseudo-resistance: delayed/reduced absorption (common with enteric-coated), non-compliance, drug interactions (ibuprofen), accelerated platelet turnover
- Clinical "resistance" = failure to prevent ischemic events despite therapy — multifactorial
Toxicity / Overdose (Salicylate Poisoning)
Acute ingestion >200 mg/kg is likely to produce intoxication.
Pathophysiology: Uncoupling of oxidative phosphorylation + medullary stimulation
Classic acid-base pattern:
- Respiratory alkalosis (early) — medullary stimulation → hyperventilation
- Metabolic acidosis (later) — lactate accumulation + bicarbonate excretion → increased anion gap
- ABG often shows a mixed respiratory alkalosis + metabolic acidosis
Other features: Tinnitus, fever (hyperthermia), vomiting, dehydration, seizures, coma, pulmonary edema, cardiovascular collapse in severe cases
Management:
| Severity | Treatment |
|---|---|
| All | Supportive care; IV fluids |
| Massive ingestion | Gastric lavage + activated charcoal + whole bowel irrigation |
| Moderate | IV sodium bicarbonate → alkalinize urine → trap ionized salicylate → promote excretion |
| Severe (coma, acidosis, salicylate >90–100 mg/dL) | Emergency hemodialysis |
Recent Evidence Update
Recent systematic reviews (2024–2025) are shifting practice on post-PCI antiplatelet therapy:
- A 2025 meta-analysis in The Lancet (PMID 40902613) found clopidogrel monotherapy may be superior to aspirin monotherapy for secondary prevention of coronary artery disease after initial dual antiplatelet therapy.
- A 2025 BMJ meta-analysis (PMID 40467090) confirmed that P2Y₁₂ inhibitor monotherapy (dropping aspirin after the initial DAPT period) after PCI is associated with lower bleeding without increasing ischemic events — challenging aspirin's traditional role as the default long-term agent post-stenting.
Sources: Harrison's Principles of Internal Medicine 22E · Braunwald's Heart Disease · Lippincott Illustrated Reviews Pharmacology · Katzung's Basic & Clinical Pharmacology · Goodman & Gilman's Pharmacological Basis of Therapeutics · Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.