Blood note
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive material from the Medical Physiology textbook and Histology text. Let me compile a thorough blood physiology note.
🩸 Blood - Complete Physiology Notes
Sources: Medical Physiology (Boron & Boulpaep), Histology: A Text and Atlas (Ross)
1. Overview
Blood is a complex fluid consisting of:
- Plasma - extracellular fluid rich in proteins
- Formed elements - red blood cells (RBCs), white blood cells (WBCs), and platelets
Total blood volume:
- Adult woman: ~70 mL/kg body weight
- Adult man: ~80 mL/kg body weight
2. Blood Composition
Formed Elements (by centrifugation)
When blood is centrifuged at 10,000 g for ~5 minutes:
| Layer | Contents |
|---|---|
| Bottom | RBCs (erythrocytes) - highest density |
| Middle (buffy coat) | WBCs (leukocytes) + platelets - whitish-gray layer |
| Top | Plasma |
Hematocrit (packed cell volume)
- Fraction of total column occupied by RBCs
- Normal adult woman: ~40%
- Normal adult man: ~45%
- Newborn: ~55% (falls to ~35% at 2 months, rises again to adult values at puberty)
- Total RBC volume: ~28 mL/kg (women), ~36 mL/kg (men)
Clinical note: Hematocrit measures RBC concentration, not total red cell mass. Immediately after hemorrhage, hematocrit may appear normal despite blood loss.
3. Plasma
Plasma is a pale-white watery solution of:
- Electrolytes
- Plasma proteins
- Carbohydrates
- Lipids
Appearance clues:
- Pink plasma = hemolysis (free Hgb in plasma)
- Brown-green = elevated bilirubin
- Cloudy = cryoglobulinemias
Plasma Proteins (normal: ~7.0 g/dL)
Provide colloid osmotic (oncotic) pressure of ~25 mmHg.
| Protein | Normal Level | Key Facts |
|---|---|---|
| Albumin | 3.5-5.5 g/dL | Synthesized by liver; half-life ~20 days; rate ~120 mg/kg/day; total pool ~135 g |
| Fibrinogen | Key coagulation factor | Converted to fibrin clot |
| Globulins | Varied | Include immunoglobulins, transport proteins |
| Coagulation factors | Varied | Molecular weights up to 970 kDa |
Urinary albumin loss is normally negligible (<20 mg/day).
4. Red Blood Cells (Erythrocytes)
Structure
- Biconcave disc shape - maximizes surface area for gas exchange
- No nucleus or organelles in mature form
- Contains hemoglobin (Hgb) - the primary O₂-carrying protein
- Contains carbonic anhydrase II (CA II) - converts CO₂ ⇌ HCO₃⁻ at extraordinarily high speed (>1 million CO₂ molecules/second per enzyme molecule)
Life Span
- 120 days - entire life spent in circulating blood
Function
- O₂ transport - hemoglobin carries O₂ from lungs to tissues
- CO₂ transport - carbonic anhydrase converts CO₂ → HCO₃⁻ for transport to lungs (see CO₂ carriage below)
- pH buffering - hemoglobin acts as a buffer
CO₂ Transport
CA II catalyzes: CO₂ + H₂O ⇌ HCO₃⁻ + H⁺
- HCO₃⁻ exits RBC via Cl⁻/HCO₃⁻ exchanger (band 3 protein) - the chloride shift
- This allows 70% of CO₂ to be carried as plasma HCO₃⁻
5. White Blood Cells (Leukocytes)
Leukocytes migrate out of circulation shortly after entering from bone marrow; they perform all their functions in the tissues.
Classification
Granulocytes (polymorphonuclear):
| Cell | % of WBC | Key Function |
|---|---|---|
| Neutrophils | 50-70% | First responders; phagocytosis of bacteria |
| Eosinophils | 1-4% | Anti-parasitic; modulate allergic responses |
| Basophils | 0.5-1% | Histamine release; allergic reactions |
Agranulocytes:
| Cell | % of WBC | Key Function |
|---|---|---|
| Lymphocytes | 20-40% | Adaptive immunity (T cells, B cells, NK cells) |
| Monocytes | 2-8% | Phagocytosis; differentiate into macrophages in tissues |
6. Platelets (Thrombocytes)
- Anucleate cell fragments derived from megakaryocytes
- Life span: 10 days - entire life spent in circulating blood
- Function: primary hemostasis (platelet plug formation), coagulation support
- Mean platelet volume (MPV) reflects average platelet size
7. Blood Cell Formation (Hemopoiesis / Hematopoiesis)
Hemopoiesis = erythropoiesis + leukopoiesis + thrombopoiesis
Goal: Maintain a constant level of all blood cell types. Blood cells have a limited lifespan and are continuously produced and destroyed.
In adults, all formed elements originate from a single pluripotent hemopoietic stem cell (HSC) in the red bone marrow.
Developmental Phases (Ontogeny)
| Phase | Timing | Site |
|---|---|---|
| Yolk sac phase | Week 3 of gestation | Yolk sac "blood islands" |
| Hepatic phase | Early fetal life | Liver (also spleen) |
| Myeloid phase | 3rd trimester onward, postnatal | Red bone marrow (permanent) |
Lymphocytes are also formed in lymphatic tissues (lymph nodes, thymus, spleen) in addition to bone marrow.
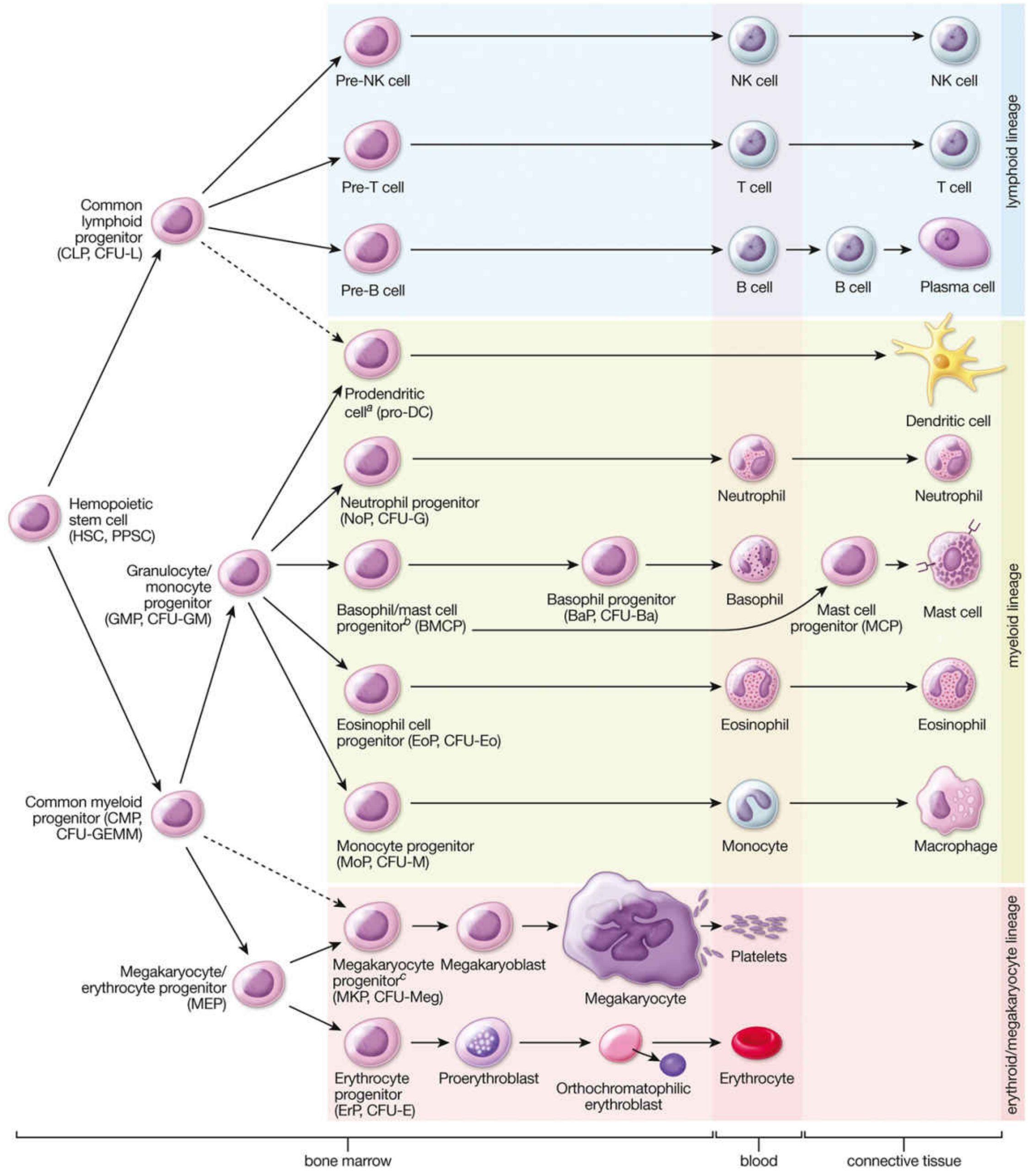
Stem Cell Hierarchy
Hemopoietic Stem Cell (HSC/PPSC)
│
├─► Common Myeloid Progenitor (CMP/CFU-GEMM)
│ │
│ ├─► Granulocyte/Monocyte Progenitor (GMP)
│ │ ├─► Neutrophil progenitor → Neutrophil
│ │ ├─► Basophil/Mast cell progenitor → Basophil / Mast cell
│ │ ├─► Eosinophil progenitor → Eosinophil
│ │ └─► Monocyte progenitor → Monocyte → Macrophage
│ │
│ └─► Megakaryocyte/Erythrocyte Progenitor (MEP)
│ ├─► Megakaryocyte progenitor → Megakaryocyte → Platelets
│ └─► Erythrocyte progenitor (CFU-E) → Erythrocytes
│
└─► Common Lymphoid Progenitor (CLP/CFU-L)
├─► Pre-NK cell → NK cell
├─► Pre-T cell → T cell
└─► Pre-B cell → B cell → Plasma cell
Erythropoiesis (RBC maturation sequence)
Proerythroblast
→ Basophilic erythroblast (ribosome-rich, basophilic)
→ Polychromatophilic erythroblast (last stage capable of mitosis; ~30 hrs)
→ Orthochromatophilic erythroblast / normoblast
(nucleus ejected; Howell-Jolly bodies = nuclear remnants; ~48 hrs)
→ Polychromatophilic erythrocyte (reticulocyte)
→ Mature erythrocyte
Key events during maturation:
- Progressive hemoglobin accumulation (cytoplasm shifts from basophilic → eosinophilic)
- Progressive RNA loss (organelles disappear)
- Nuclear condensation and ejection at orthochromatophilic stage
- Reticulocytes retain some polyribosomes; still synthesize Hgb
Regulation of Erythropoiesis
- Erythropoietin (EPO) - ~34 kDa glycoprotein; acts via tyrosine kinase-associated receptor
- In adults: produced mainly by fibroblast-like type I interstitial cells of renal cortex/outer medulla
- In fetal life: produced mainly by liver; liver (Kupffer cells) produce some EPO in adults too
- Stimulus: hypoxia (low O₂ delivery to kidney)
- Effect: stimulates proerythroblast production; accelerates RBC progenitor development
Thrombopoiesis (platelet formation)
- Megakaryocytes in bone marrow shed cytoplasmic fragments → platelets
- Regulated by thrombopoietin (TPO)
8. Key Normal Blood Values (Reference)
| Parameter | Normal Range |
|---|---|
| Hematocrit (women) | ~40% |
| Hematocrit (men) | ~45% |
| Plasma albumin | 3.5-5.5 g/dL |
| Total plasma protein | ~7.0 g/dL |
| Oncotic pressure | ~25 mmHg |
| RBC life span | 120 days |
| Platelet life span | 10 days |
| Neutrophils (% WBC) | 50-70% |
| Lymphocytes (% WBC) | 20-40% |
| Monocytes (% WBC) | 2-8% |
| Eosinophils (% WBC) | 1-4% |
| Basophils (% WBC) | 0.5-1% |
| Transferrin | 200-400 mg/dL |
9. Quick Summary Table: Formed Elements
| Cell | Origin | Life Span | Where Active | Key Role |
|---|---|---|---|---|
| Erythrocyte | Bone marrow | 120 days | Blood | O₂/CO₂ transport |
| Platelet | Bone marrow (megakaryocytes) | 10 days | Blood | Hemostasis |
| Neutrophil | Bone marrow | Hours-days | Tissues | Bacterial phagocytosis |
| Eosinophil | Bone marrow | Days | Tissues | Anti-parasitic, allergy |
| Basophil | Bone marrow | Days | Tissues/blood | Histamine release |
| Monocyte/Macrophage | Bone marrow | Days-years | Tissues | Phagocytosis, antigen presentation |
| Lymphocyte (T/B/NK) | Bone marrow + lymphoid tissue | Days-years | Tissues/blood | Adaptive & innate immunity |
- Medical Physiology (Boron & Boulpaep), Chapter 18 - Blood
- Histology: A Text and Atlas (Ross), Chapter 10 - Blood and Hemopoiesis
Blood note for dmlt
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have rich DMLT-focused content from Henry's Clinical Diagnosis & Lab Methods and the Histology textbook. Let me compile the comprehensive DMLT-oriented blood note.
🩸 Blood - Notes for DMLT (Diploma in Medical Laboratory Technology)
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods | Histology: A Text and Atlas (Ross) | Medical Physiology (Boron & Boulpaep)
UNIT 1: BLOOD COLLECTION & SPECIMEN HANDLING
1.1 Venipuncture - Key Points
- Patient should be seated/supine for 15-20 min before blood draw to avoid hemoconcentration
- Tourniquet application: <60 seconds (longer causes hemoconcentration)
- Allow alcohol to dry completely before puncture (wet alcohol causes hemolysis)
- Use correct gauge needle; pulling syringe plunger too fast = hemolysis
- Preferred site: antecubital fossa (reduces hemolysis)
- Mix anticoagulant tubes immediately after filling by gentle inversion
1.2 Blood Collection Tubes - Color Code System
| Cap Color | Additive | Used For |
|---|---|---|
| Red | None (plain) | Serum chemistry, serology |
| Purple/Lavender | EDTA | CBC, blood film, ESR |
| Blue | Sodium citrate | Coagulation tests (PT, APTT) |
| Green | Heparin | Plasma chemistry |
| Grey | Sodium fluoride + oxalate | Blood glucose, lactate |
| Yellow | SST (clot activator + gel) | Serum chemistry |
Correct order of draw: Blood culture → Blue → Red/SST → Green → Purple → Grey
1.3 Causes & Effects of Hemolysis
Hemolysis occurs when: needle too small, syringe pulled too fast, vigorous shaking, blood expelled forcefully, or alcohol not dry.
| Analyte falsely INCREASED by hemolysis |
|---|
| Potassium (K⁺) - clinically dangerous |
| Magnesium, Iron, Phosphorus |
| LDH (LD), Total protein, Ammonium |
Important: Strong hemolysis can raise K⁺ by 2-3 mEq/L into a critical range.
1.4 Preanalytical Variables Affecting Results
| Variable | Effect |
|---|---|
| Posture (standing vs supine) | Increases protein, Hb, Hct |
| Exercise | Increases CK, LDH, WBC |
| Diet (non-fasting) | Increases glucose, triglycerides |
| Biotin supplements | Falsely high/low immunoassay results (TSH, troponin, hormones) |
| Age & Sex | Reference ranges differ |
UNIT 2: BLOOD COMPOSITION
2.1 What is Blood?
Blood = Plasma (55%) + Formed Elements (45%)
- Total volume: ~70 mL/kg (women) | ~80 mL/kg (men)
- Hematocrit = % of blood occupied by RBCs
| Population | Normal Hematocrit |
|---|---|
| Adult male | ~45% |
| Adult female | ~40% |
| Newborn | ~55% |
| 2 months old | ~35% (lowest point) |
2.2 Plasma
Pale-yellow fluid containing:
- Electrolytes (Na⁺, K⁺, Cl⁻, HCO₃⁻)
- Plasma proteins (~7.0 g/dL total)
- Glucose, lipids, hormones, waste products
Plasma Proteins
| Protein | Level | Function |
|---|---|---|
| Albumin | 3.5-5.5 g/dL | Oncotic pressure, transport (drugs, bilirubin, Ca²⁺) |
| Fibrinogen | 200-400 mg/dL | Coagulation (converted to fibrin) |
| Globulins | ~2.5-3.5 g/dL | Immunoglobulins (IgG, IgA, IgM), transport proteins |
| Coagulation factors | Trace | Clotting cascade |
- Oncotic pressure = ~25 mmHg (prevents fluid leaking out of capillaries)
- Albumin made by liver; half-life ~20 days
Lab note: Serum = plasma minus fibrinogen (after clot formation)
UNIT 3: FORMED ELEMENTS (BLOOD CELLS)
3.1 Red Blood Cells (Erythrocytes)
| Feature | Detail |
|---|---|
| Shape | Biconcave disc |
| Diameter | 6-8 μm |
| Thickness | 2 μm (centre) |
| No nucleus/organelles | (mature RBC) |
| Life span | 120 days |
| Destruction site | Spleen (extravascular hemolysis) |
| MCV | 80-100 fL |
| MCH | 27-33 pg |
| MCHC | 31.5-36 g/dL |
Functions:
- O₂ transport via hemoglobin (Hgb)
- CO₂ transport via carbonic anhydrase (CA-II): CO₂ + H₂O ⇌ HCO₃⁻ + H⁺ → Chloride shift
- Buffering (hemoglobin acts as buffer)
Hemoglobin
- Normal Hgb: 13.5-17.5 g/dL (men) | 12.0-15.5 g/dL (women)
- Structure: 4 globin chains + 4 heme groups (each contains Fe²⁺)
- Types: HbA (α₂β₂ - adult) | HbF (α₂γ₂ - fetal) | HbA₂ (α₂δ₂)
Abnormal RBC Morphology on Peripheral Smear
| Cell Shape | Name | Associated Condition |
|---|---|---|
| Sphere-shaped RBCs | Spherocytes | Hereditary spherocytosis, autoimmune hemolysis |
| Fragmented RBCs | Schistocytes | Microangiopathic hemolytic anemia (TTP, DIC) |
| Sickle-shaped | Drepanocytes | Sickle cell disease |
| Target cells | Codocytes | Thalassemia, liver disease, HbC |
| Oval macrocytes | Macro-ovalocytes | Megaloblastic anemia (B12/folate deficiency) |
| Tear-drop shaped | Dacrocytes | Myelofibrosis, megaloblastic anemia |
| Small dense cells | Microcytes | Iron deficiency anemia, thalassemia |
| Nuclear remnants | Howell-Jolly bodies | Post-splenectomy, megaloblastic anemia |
| Iron granules in ring | Ring sideroblasts | Sideroblastic anemia |
3.2 White Blood Cells (Leukocytes)
Total WBC count: 4,000-11,000/mm³
| Cell Type | % (Normal) | Size (μm) | Nucleus | Granules | Function |
|---|---|---|---|---|---|
| Neutrophil | 50-70% | 10-12 | Multi-lobed (2-5 lobes) | Fine, pink-lilac (specific) + azurophilic | Phagocytosis of bacteria; first responder |
| Eosinophil | 1-4% | 10-14 | Bilobed | Large, bright red-orange | Anti-parasitic; modulates allergy |
| Basophil | 0.5-1% | 8-10 | S-shaped/irregular | Large, dark blue-purple (mask nucleus) | Histamine/heparin release; allergy |
| Lymphocyte | 20-40% | 7-18 | Round, dense (small), indented (medium) | Rare azurophilic | Adaptive immunity (T, B, NK cells) |
| Monocyte | 2-8% | 14-20 | Kidney/horseshoe-shaped | Fine azurophilic | Phagocytosis; differentiates → macrophage |
Neutrophil Granules (Important for DMLT)
- Azurophilic (primary) granules - lysosomes; contain myeloperoxidase (MPO), defensins, cathelicidin, acid hydrolases
- Specific (secondary) granules - contain lactoferrin, lysozyme, collagenase
- Gelatinase (tertiary) granules - contain gelatinase/MMP-9
Drumstick appendage on neutrophil nucleus = Barr body (inactive X chromosome; seen in females)
Neutrophil Killing Mechanisms
- Oxygen-dependent (main): NADPH oxidase → superoxide (O₂⁻) → H₂O₂ → hypochlorite (via MPO) = respiratory burst
- Oxygen-independent: Defensins, lysozyme, lactoferrin, cathepsins
CGD (Chronic Granulomatous Disease) = NADPH oxidase mutation → recurrent bacterial infections
Lymphocyte Types
| Type | Marker | Function |
|---|---|---|
| T cell | CD3, CD4 or CD8 | Cell-mediated immunity |
| - CD4+ T helper | CD4 | Activates B cells, macrophages (MHC II restricted) |
| - CD8+ Cytotoxic T | CD8 | Kills infected cells (MHC I restricted) |
| B cell | CD19, CD20 | Antibody production → becomes plasma cell |
| NK cell | CD16, CD56 | Kills tumor cells and virus-infected cells (no prior sensitization) |
3.3 Platelets (Thrombocytes)
| Feature | Detail |
|---|---|
| Origin | Megakaryocyte fragments |
| Size | 2-4 μm |
| Normal count | 1.5-4.0 × 10⁵/mm³ (150,000-400,000/μL) |
| Life span | 10 days |
| No nucleus | Anucleate |
| MPV | Reflects platelet size (large = young platelets) |
Functions:
- Primary hemostasis - adhere to damaged vessel wall → form platelet plug
- Support coagulation - provide phospholipid surface for coagulation factors
UNIT 4: BLOOD FILM - PREPARATION & STAINING
4.1 Peripheral Blood Smear Preparation (Wedge Method)
- Place small drop of blood 1-2 cm from one end of slide
- Place spreader slide at 30-45° angle in front of the drop
- Pull back to touch the drop, then push forward smoothly
- Dry rapidly by waving in air
- Label with pencil at the thick end
Areas of the smear:
- Thick end - good for scanning, not examining cell morphology
- Body - RBCs overlapping
- Feather edge (thin end) - ideal area for differential count; WBCs well-spread; monolayer of RBCs
Caution on wedge smear: monocytes concentrate at the tip/feather edge; neutrophils crowd the lateral edges
4.2 Staining Methods
Romanowsky Stains (most common for blood films)
All Romanowsky stains = combination of basic dye (methylene blue/thiazine) + acid dye (eosin)
| Stain | Key Features |
|---|---|
| Wright's stain | Most commonly used in routine labs; methyl alcohol base (acts as fixative too); buffer pH 6.4 |
| Leishman's stain | Widely used in India/UK; similar to Wright's |
| Giemsa stain | Preferred for parasites (malaria); pH 7.2 ideal |
| May-Grünwald Giemsa (MGG) | Combination; excellent nuclear detail |
| JSB (Jenner-Giemsa) | Used in some labs |
Wright's Stain Procedure (Step-by-Step)
- Prepare and air-dry blood film
- Fix with absolute methanol for 1-2 minutes
- Cover with undiluted Wright's stain for 2 minutes
- Add equal volume of buffer (pH 6.4), mix gently (blow); stain for 4-6 minutes
- Flush with distilled water/buffer
- Allow to dry; examine under oil immersion (100×)
Staining Characteristics (What stains what)
| Component | Color with Romanowsky Stain |
|---|---|
| RBCs | Eosinophilic (pink-red) |
| Neutrophil granules | Neutral (lilac-pink) |
| Eosinophil granules | Bright orange-red |
| Basophil granules | Dark blue-purple |
| Lymphocyte nucleus | Deep purple |
| Monocyte nucleus | Blue-grey, kidney shaped |
| Platelets | Purple granules |
| Malarial parasites | Blue cytoplasm, red/purple nucleus |
4.3 Special Stains Used in DMLT
| Stain | Purpose |
|---|---|
| Prussian Blue (Perls') | Detects iron in RBCs; identifies ring sideroblasts |
| PAS (Periodic Acid-Schiff) | Detects glycogen; used in leukemia classification |
| Sudan Black B | Lipids in granulocytes; positive in myeloid leukemia |
| Toluidine Blue | Mast cell granules |
| Reticulocyte stain (New Methylene Blue / BCB) | Stains residual RNA in reticulocytes (appears blue) |
UNIT 5: HEMATOPOIESIS (Blood Cell Formation)
5.1 Sites of Hematopoiesis (Developmental Stages)
| Phase | Gestational Age | Site |
|---|---|---|
| Mesoblastic (Yolk sac) | Week 3 of gestation | Yolk sac blood islands |
| Hepatic | 2nd-7th month | Liver (primary), spleen |
| Myeloid (Medullary) | 3rd trimester → life | Red bone marrow (permanent) |
Extramedullary hematopoiesis = blood cell formation outside bone marrow (spleen/liver) - seen in thalassemia, myelofibrosis
5.2 Sites of Red Bone Marrow in Adults
- Flat bones: sternum, ribs, vertebrae, skull
- Upper ends of long bones: femur, humerus
- Iliac crest (site of bone marrow biopsy/aspiration)
5.3 Stem Cell Hierarchy
Pluripotent Hemopoietic Stem Cell (HSC)
│
├─► Common Myeloid Progenitor (CMP/CFU-GEMM)
│ ├─► GMP → Neutrophil, Eosinophil, Basophil, Monocyte
│ └─► MEP → Megakaryocyte (→Platelets) + Erythrocyte
│
└─► Common Lymphoid Progenitor (CLP)
├─► T cell (matures in thymus)
├─► B cell (matures in bone marrow → plasma cell)
└─► NK cell
CFU = Colony Forming Unit (old nomenclature):
- CFU-E = erythrocyte, CFU-G = granulocyte, CFU-M = monocyte, CFU-Meg = megakaryocyte, CFU-GEMM = pluripotent myeloid
5.4 Erythropoiesis - Maturation Sequence
| Stage | Key Features |
|---|---|
| Proerythroblast | Large cell, basophilic cytoplasm, large nucleus |
| Basophilic erythroblast | Intensely basophilic (RNA rich), nucleus visible |
| Polychromatophilic erythroblast | Mixed basophilic + eosinophilic; last stage to divide (~30 hrs) |
| Orthochromatophilic erythroblast (Normoblast) | Pink cytoplasm, dense pyknotic nucleus; nucleus ejected (~48 hrs); Howell-Jolly bodies may appear |
| Reticulocyte | No nucleus; residual RNA stains blue with NMB; slightly larger than mature RBC |
| Mature Erythrocyte | Biconcave, no nucleus, eosinophilic |
As cells mature: nucleus shrinks → cytoplasm turns from blue to pink → cell gets smaller → nucleus expelled
Regulation of Erythropoiesis
- Erythropoietin (EPO): ~34 kDa glycoprotein
- Adults: produced by peritubular fibroblasts in renal cortex
- Fetus: produced by liver
- Trigger: hypoxia → increases EPO → stimulates RBC progenitors
- Used clinically in anemia of CKD (recombinant EPO / Darbepoetin)
5.5 Granulopoiesis (Granulocyte Maturation)
Myeloblast → Promyelocyte → Myelocyte → Metamyelocyte → Band (Stab) → Mature Neutrophil
- Myeloblast: large nucleus, no granules
- Promyelocyte: primary (azurophilic) granules appear
- Myelocyte: specific granules appear; last stage capable of division
- Metamyelocyte: indented kidney-shaped nucleus; non-dividing
- Band (Stab) cell: horseshoe-shaped nucleus; immature neutrophil in peripheral blood
- Mature neutrophil: 2-5 lobed nucleus
"Shift to the left" = increase in band cells/immature neutrophils = bacterial infection/stress response
UNIT 6: HAEMATOLOGICAL INDICES & REFERENCE VALUES
6.1 Complete Blood Count (CBC) - Normal Reference Values
| Parameter | Male | Female |
|---|---|---|
| Hemoglobin (g/dL) | 13.5-17.5 | 12.0-15.5 |
| Hematocrit (%) | 40-52 | 35-47 |
| RBC count (×10⁶/μL) | 4.5-5.5 | 3.8-5.0 |
| MCV (fL) | 80-100 | 80-100 |
| MCH (pg) | 27-33 | 27-33 |
| MCHC (g/dL) | 31.5-36 | 31.5-36 |
| WBC (×10³/μL) | 4.0-11.0 | 4.0-11.0 |
| Platelets (×10³/μL) | 150-400 | 150-400 |
| Reticulocytes (%) | 0.5-2.5% | 0.5-2.5% |
| ESR (mm/hr) | 0-15 | 0-20 |
6.2 RBC Indices Interpretation
| Index | Formula | Interpretation |
|---|---|---|
| MCV | Hct (%) × 10 / RBC count | <80 = microcytic; 80-100 = normocytic; >100 = macrocytic |
| MCH | Hgb (g/dL) × 10 / RBC | <27 = hypochromic |
| MCHC | Hgb / Hct × 100 | >36 = hyperchromic (rare); seen in spherocytosis |
| RDW | Variation in RBC size | >14.5% = anisocytosis; helps differentiate iron def. from thalassemia |
6.3 Anemia Classification by MCV
| Type | MCV | Causes |
|---|---|---|
| Microcytic | <80 fL | Iron deficiency, thalassemia, sideroblastic, lead poisoning |
| Normocytic | 80-100 fL | Acute blood loss, hemolysis, aplastic anemia, CKD |
| Macrocytic | >100 fL | B12/folate deficiency (megaloblastic); hypothyroidism; liver disease |
6.4 Reticulocyte Count
- Stained with New Methylene Blue (NMB) or Brilliant Cresyl Blue (BCB) - precipitates residual RNA
- Normal: 0.5-2.5%
- High (reticulocytosis) = active RBC production = hemorrhage, hemolysis, treatment response
- Low (reticulocytopenia) = bone marrow failure, aplastic anemia, B12/folate deficiency
6.5 ESR (Erythrocyte Sedimentation Rate)
- Westergren method (gold standard): blood drawn into sodium citrate (4:1); measured at 1 hour
- Normal: men 0-15 mm/hr; women 0-20 mm/hr
- Increased ESR: inflammation, infection, malignancy, pregnancy, anemia
- Decreased ESR: polycythemia, sickle cell disease, spherocytosis
UNIT 7: BONE MARROW EXAMINATION
7.1 Indications
- Unexplained cytopenia (low RBC, WBC, or platelets)
- Suspected leukemia/lymphoma
- Staging of malignancies
- Diagnosis of aplastic anemia, MDS, myeloma
7.2 Sites for Aspiration/Biopsy
- Posterior superior iliac crest (most common)
- Sternum (aspiration only)
- Anterior iliac crest
7.3 Bone Marrow Cellularity (Normal by Age)
- Normal cellularity at 50 years: vertebrae ~75%, sternum ~60%, iliac crest ~50%, rib ~30%
- Hypercellular marrow = increased hematopoiesis (leukemia, hemolysis, B12 deficiency)
- Hypocellular marrow = aplastic anemia
7.4 Myeloid : Erythroid (M:E) Ratio
- Normal: 3:1 to 4:1
- Increased (>5:1): infection, leukemia, erythroid hypoplasia
- Decreased (<2:1): megaloblastic anemia, hemolytic anemia (erythroid hyperplasia)
7.5 Differential Count from Bone Marrow Aspirate
- 300-500 cells are counted
- Scan under low then high magnification
- Allows assessment of maturation, dysplasia, and lineage proportions
UNIT 8: KEY DMLT EXAM POINTS (QUICK RECALL)
| Topic | Fact |
|---|---|
| RBC life span | 120 days |
| Platelet life span | 10 days |
| WBC life span | Neutrophils: hours-days; Lymphocytes: years |
| Hematopoiesis regulation | EPO (RBC), TPO (platelets), G-CSF (neutrophils) |
| Site of RBC destruction | Spleen (extravascular); vessels (intravascular) |
| Anticoagulant for CBC | EDTA (lavender/purple tube) |
| Anticoagulant for ESR | Sodium citrate (blue tube, 4:1 ratio) |
| Anticoagulant for bone marrow | EDTA or heparin |
| Stain for reticulocytes | New Methylene Blue (NMB) |
| Stain for iron in marrow | Prussian Blue (Perls') |
| Stain for malaria | Giemsa (pH 7.2) |
| Serum vs Plasma | Serum = no fibrinogen (after clot) |
| Barr body location | Drumstick appendage on neutrophil nucleus (females) |
| Shift to the left | Increased band cells = bacterial infection |
| CGD disease | NADPH oxidase defect → recurrent infections |
| Ring sideroblasts (>5 lobes) | ≥5% neutrophils = hypersegmentation = megaloblastic anemia |
- Henry's Clinical Diagnosis and Management by Laboratory Methods, Chapters 3 & 31
- Histology: A Text and Atlas (Ross), Chapter 10
- Medical Physiology (Boron & Boulpaep), Chapter 18
This is a shared conversation. Sign in to Orris to start your own chat.