tredelenbarg test
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Trendelenburg Test
What It Tests
The Trendelenburg test assesses the strength and integrity of the hip abductor mechanism - primarily the gluteus medius and gluteus minimus muscles, acting on a stable fulcrum between the pelvis and femur.
How to Perform
- Ask the patient to stand on the unaffected limb first - the buttock on the affected side automatically rises (normal).
- Ask the patient to stand on the affected limb - watch the pelvis from behind.
- Observe the iliac crests and gluteal folds for any drop.
The examiner should stand behind the patient to best visualize pelvic tilt.
Interpreting the Result
| Finding | Interpretation |
|---|---|
| Normal (negative): Standing on one leg causes pelvis to rise on the opposite (swing) side | Abductors functioning normally |
| Positive: Pelvis drops/sags on the unsupported (swing) side | Abductor mechanism failure on the stance side |
Remember the mnemonic: the pelvis drops away from (opposite to) the weak side.
Clinical Photos
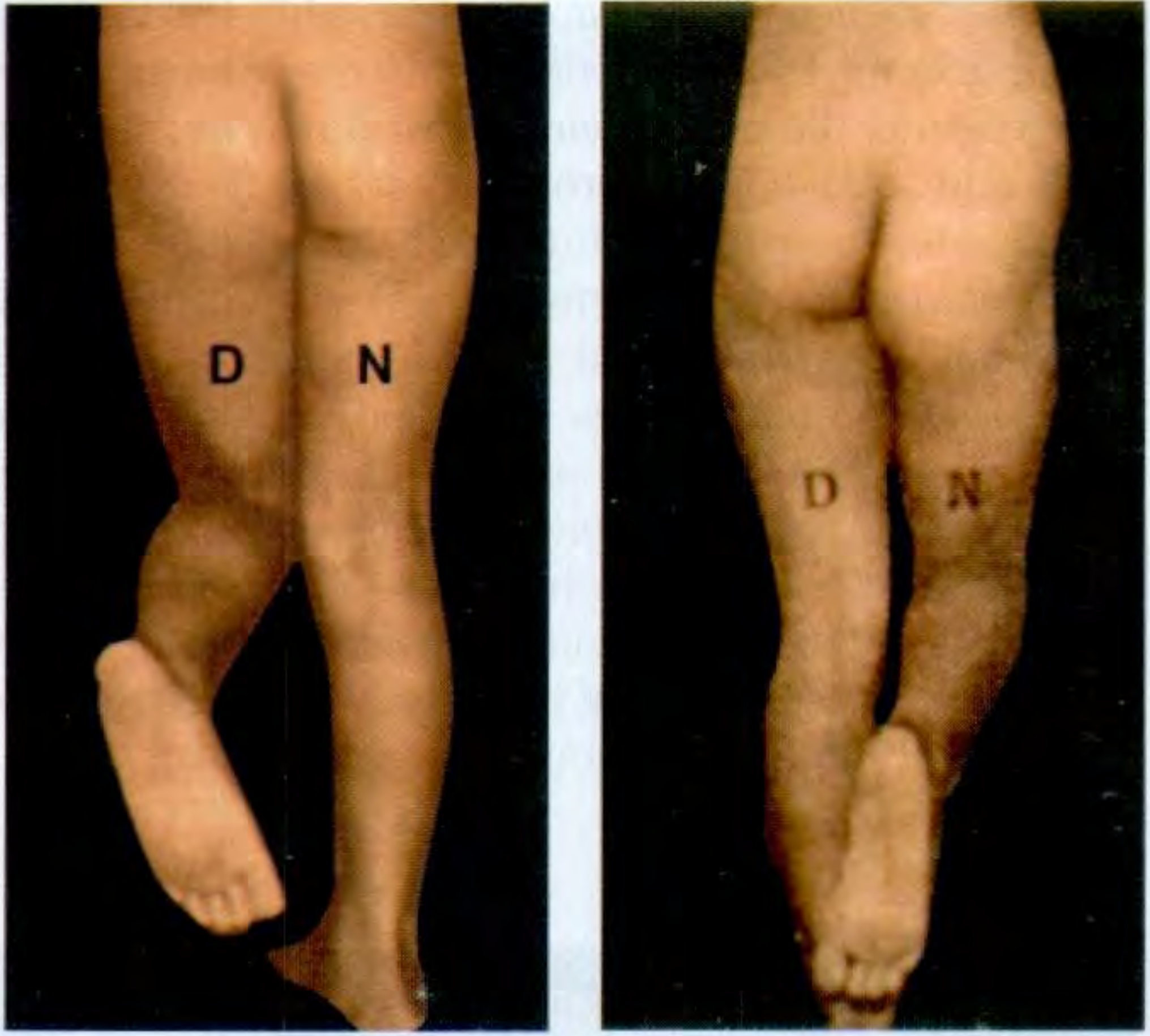
Left panel: standing on normal (N) leg - pelvis on diseased (D) side rises normally. Right panel: standing on diseased (D) leg - pelvis drops on normal (N) side = positive test.
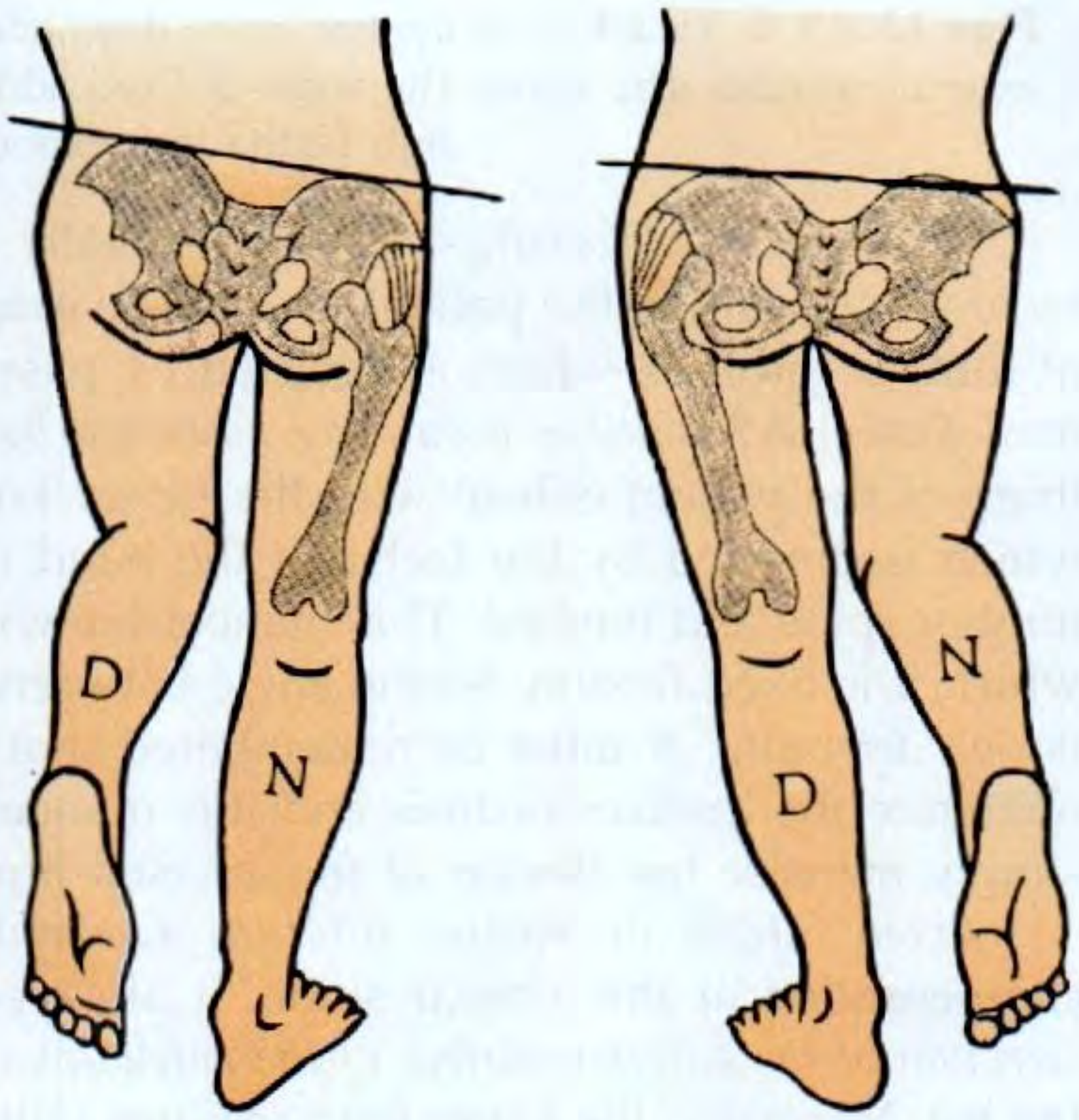
Diagrammatic cross-section showing pelvic tilt in the two positions - D = diseased side, N = normal side.
Causes of a Positive Trendelenburg Sign
The test reflects failure of the osseomuscular mechanism between pelvis and femur. It becomes positive in four broad categories:
- Weak abductors - poliomyelitis, muscular dystrophies, motor neurone disease, superior gluteal nerve damage
- Unstable fulcrum - congenital or pathological dislocation of the hip (muscles cannot act without a stable pivot)
- Broken lever system - fracture neck of femur, coxa vara, Perthes' disease
- Pain inhibition - any arthritis of the hip causing the patient to avoid loading the affected side
Nerve Involved
A positive sign most commonly reflects damage to the superior gluteal nerve (L4, L5, S1), which supplies gluteus medius, gluteus minimus, and tensor fasciae latae. Causes include:
- Pelvic fractures
- Space-occupying lesions in the greater sciatic foramen
- Hip surgery with disruption/atrophy of the gluteus medius/minimus tendon insertion on the greater trochanter
Gait Consequence: The Duchenne Limp / Waddling Gait
When the abductors fail, the pelvis drops toward the swing side during the stance phase. The patient compensates by lurching the trunk toward the affected side (Duchenne limp) - this shifts the centre of gravity over the stance limb and reduces the pelvic drop. With bilateral small gluteal weakness, this produces a characteristic waddling gait.
- Unilateral weakness = Trendelenburg sign + Duchenne limp
- Bilateral weakness = waddling (gluteal) gait
Brodie-Trendelenburg Test (Vascular - Different Test)
Note there is also a separate Brodie-Trendelenburg test used in vascular surgery to assess sapheno-femoral valve incompetence in varicose veins. The leg is elevated to drain varicosities, a tourniquet is applied at the suspected incompetent feeding vein, and the patient stands. If varices remain empty with the tourniquet in place but fill immediately on release, the site of incompetence has been correctly identified. This is an entirely different test despite sharing the Trendelenburg name.
Sources: S Das - A Manual on Clinical Surgery 13th Ed, p. 240 | Gray's Anatomy for Students | THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System | Pye's Surgical Handicraft 22nd Ed | Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.