Vertigo menuvers
Reading File
Finding Sources
Searching PubMed
"BPPV" AND "canalith repositioning" AND maneuver
Finding Sources
Searching the Web
Epley maneuver Semont Barbecue roll BPPV vertigo repositioning steps 2025
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of vertigo maneuvers, covering diagnosis, treatment, and the latest evidence.
Vertigo Maneuvers
Background: What Is BPPV?
Benign Paroxysmal Positional Vertigo (BPPV) is the most common cause of vertigo, accounting for 38-56% of all peripheral vestibular disorders. It results from displaced calcium carbonate crystals (otoliths/canaliths) that migrate from the utricle into the semicircular canals. The posterior canal is most commonly affected; the horizontal (lateral) canal is less common.
Diagnostic Maneuver: Dix-Hallpike Test
Before any treatment, you must identify the affected ear and canal.
Steps:
- Patient sits upright on the exam table, head turned 45° toward the suspected ear
- Rapidly lower the patient to supine with the head hanging 20-30° below horizontal (ear now pointing down)
- Observe for nystagmus and ask about vertigo
Positive result: Rotatory-vertical nystagmus appearing after a 1-10 second latency, lasting <60 seconds. The upper pole of the eyes beats toward the dependent (affected) ear. - Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1459
The side that produces greater nystagmus identifies the affected ear. Atypical nystagmus (purely vertical, no latency, no fatigue) should raise suspicion for a central cause.
Contraindications to Dix-Hallpike (and all repositioning maneuvers):
- Severe cervical spine disease
- Unstable spinal injury
- High-grade carotid stenosis
Treatment Maneuvers
1. Epley Maneuver (Posterior Canal BPPV - First Line)
The Epley (canalith repositioning procedure) is the gold standard for posterior canal BPPV, effective in >80% of cases with a single treatment. - Cummings Otolaryngology Head and Neck Surgery
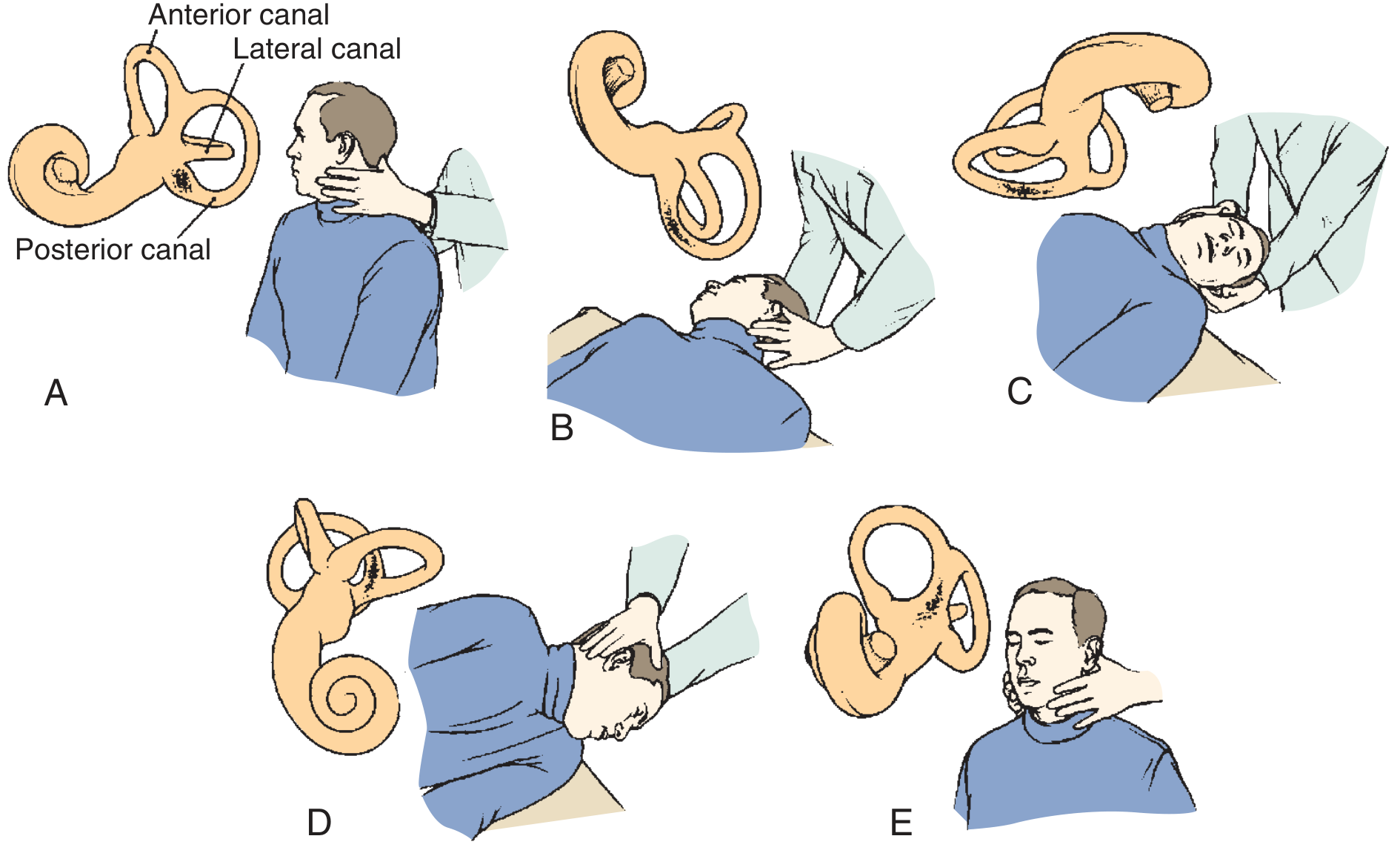
Steps (for right ear BPPV):
| Step | Position | Hold Time |
|---|---|---|
| A | Sit upright, head turned 45° toward right (affected) ear | Start position |
| B | Rapidly recline to supine with head hanging, turned 45° right (Dix-Hallpike position) | Until nystagmus resolves |
| C | Rotate head 90° to the left (nose pointing left) | Until nystagmus resolves |
| D | Roll head and body together 90° further to the left (face-down, nose toward floor) | 20-30 seconds |
| E | Slowly return to sitting upright | - |
- Repeat until no nystagmus is elicited
- En-bloc head-body movement is preferred (no isolated head turning)
- Premedicate with low-dose meclizine or a benzodiazepine 1 hour before if the patient is very anxious or vomit-prone
- Advise the patient to remain upright for 24 hours post-procedure
2. Semont Maneuver (Posterior Canal BPPV - Alternative)
Also effective for posterior canal BPPV but involves more abrupt movements and is slightly less comfortable than the Epley. - Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1460
Steps (for left ear BPPV):
- Patient sits on bed, head turned 45° toward the unaffected (right) side
- Quickly lay the patient down onto the affected (left) side - head stays turned 45°, so patient looks toward the ceiling
- Hold 1-2 minutes (until vertigo resolves)
- Rapidly swing the patient through sitting to the opposite side-lying position (right side down) - head still in the same rotation, now facing toward the floor
- Hold 1-2 minutes, then slowly return to upright
The key difference from Epley: movements are rapid and the head position on the body stays fixed while the body swings.
3. Barbecue Roll / Lempert Maneuver (Horizontal Canal BPPV)
Used when the horizontal (lateral) canal is affected. Diagnosed with the Roll Test (patient supine, head turned 90° to each side while lying flat - geotropic or apogeotropic nystagmus).
Steps (for right horizontal canal BPPV):
- Patient lies supine, head turned 90° to the right (affected side). Hold 30 seconds
- Roll 90° to face up (supine). Hold 30 seconds
- Roll 90° to face left (unaffected ear down). Hold 30 seconds
- Roll 90° face-down (prone), chin slightly tucked. Hold 30 seconds
- Roll 90° back to right side again. Hold 30 seconds
- Slowly sit up - keep chin level
The maneuver completes one full 360° revolution. Each stop allows canaliths to roll toward the utricle exit. Repeat as needed.
A demonstration of the Roll Test and BBQ Roll maneuver:
4. Brandt-Daroff Exercises (Home Exercises)
Used for cases where office maneuvers fail, or for patient self-treatment. Less effective than the Epley for clearing canaliths, but useful for habituation.
Steps:
- Sit upright on the edge of the bed
- Quickly lie down to one side with the head angled 45° upward (as if looking at the ceiling corner)
- Hold 30 seconds (or until vertigo stops)
- Return to sitting, hold 30 seconds
- Repeat to the other side
- Perform 5 repetitions each side, 2-3 times per day
Efficacy Summary
| Maneuver | Canal | Success Rate | Evidence |
|---|---|---|---|
| Epley | Posterior | >80-85% | RCTs, first-line |
| Semont | Posterior | ~80-90% (similar to Epley) | RCTs |
| BBQ Roll | Horizontal | 70-80% | RCTs |
| Brandt-Daroff | Posterior | ~50% | Habituation only |
A 2026 network meta-analysis (Frontiers in Neurology, 2026) confirmed that the Epley and Semont maneuvers have optimal short-term efficacy for posterior canal BPPV and should be recommended as first-line strategies.
Post-Maneuver Instructions
- Remain upright for 24 hours after a successful procedure
- Avoid sleeping on the affected side for 1-2 nights
- Expect that ~20% of patients will have recurrence within 2 weeks, and up to 50% long-term
- Nausea occurs in 16-32% during the Epley maneuver - this is normal
- If vertigo worsens after a maneuver, conversion to a different canal (e.g., posterior to horizontal) may have occurred - re-examine and retreat
Complications
- Transient intense vertigo and nausea during the maneuver (expected)
- Canal conversion (posterior to horizontal BPPV) during Epley - ~1-2% of cases
- Postural crisis (falls) - rare but documented in systematic review (PMID: 39833058)
- BPPV recurrence: a 2025 meta-analysis identified key risk factors including vitamin D deficiency, osteoporosis, and head trauma (PMID: 40211383)
Sources: Cummings Otolaryngology Head and Neck Surgery; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Textbook of Family Medicine 9e; Frontiers in Neurology 2026 network meta-analysis.
This is a shared conversation. Sign in to Orris to start your own chat.