Colonic polyposis syndrome
colonic polyposis syndrome genetics management
Colonic Polyposis Syndromes
Classification (Sleisenger & Fordtran's GI and Liver Disease)
| Category | Syndromes |
|---|---|
| Adenomatous | Classic FAP, Attenuated FAP (AFAP), Gardner syndrome, Turcot syndrome, MUTYH-associated polyposis (MAP), Polymerase proofreading-associated polyposis (PPAP), NTHL1 polyposis |
| Serrated | Serrated polyposis syndrome |
| Hamartomatous | Peutz-Jeghers syndrome, Juvenile polyposis, Cowden disease, Bannayan-Ruvalcaba-Riley syndrome |
| Rare hamartomatous | Hereditary mixed polyposis, Intestinal ganglioneuromatosis, Basal cell nevus syndrome |
| Non-inherited | Cronkhite-Canada syndrome, Lymphomatous polyposis |
I. Adenomatous Polyposis Syndromes
1. Familial Adenomatous Polyposis (FAP)
- Diagnosis requires >100 synchronous colonic adenomas (classic FAP); thousands may be present
- Polyps are morphologically indistinguishable from sporadic adenomas
- Predominantly in the rectum and left colon; appear in adolescence (present in 15% by age 10, 75% by age 20)
- Without prophylactic colectomy, CRC risk approaches 100% by age 35-40 years
- Duodenal adenomas: >95% of FAP patients; most common around the ampulla of Vater; develop ~15 years after colonic polyps. Duodenal cancer (in 5-10%) is the 2nd leading cause of death in FAP. Staged by the Spiegelman scoring system (Stage IV = 36% cancer risk at 10 years)
- Gastric: Fundic gland polyps (30-90%, low malignant potential); gastric adenomas (10-30%, antrum, higher risk in Japanese/Korean patients)
| Feature | Frequency |
|---|---|
| Osteomas (mandible, skull, long bones) | 50-90% |
| Congenital hypertrophic retinal pigment epithelium (CHRPE) | 70-80% |
| Epidermoid/sebaceous cysts | 50% |
| Desmoid tumors | 10-24% (3rd leading cause of death) |
| Fibromas | 25-50% |
| Thyroid cancer (papillary) | 2-3% |
| Dental abnormalities / supernumerary teeth | Variable |
| Hepatoblastoma | Rare |
| Medulloblastoma (Turcot variant) | Rare |
- Annual flexible sigmoidoscopy/colonoscopy from age 10-12 years
- Upper endoscopy (EGD) from age 20-25 years
- Annual thyroid ultrasound
| Operation | Indications |
|---|---|
| Total abdominal colectomy (TAC) + ileorectal anastomosis (IRA) | Colon cancer; rectum has <20 polyps manageable endoscopically |
| Total proctocolectomy (TPC) + ileal pouch-anal anastomosis (IPAA) | Profuse polyposis; rectal cancer; rectal polyp burden >20 |
2. Attenuated FAP (AFAP)
- Gene: APC mutations at the very proximal (5') or distal (3') ends of the gene
- Fewer adenomas (typically <100), flat growth pattern, cluster in the proximal colon
- Present in adulthood rather than adolescence; CRC risk still high but occurs later (≥55 years)
- Surveillance: colonoscopy every 1-2 years from age 25 years
- Upper GI surveillance similar to classic FAP
3. Gardner Syndrome
- Prominent osteomas, epidermoid cysts, desmoid tumors
- Supernumerary teeth, dental abnormalities
- Now considered part of the FAP spectrum, not a separate entity
4. Turcot Syndrome (Glioma-Polyposis)
- Colonic polyposis + primary CNS tumors
- Represents two genetically distinct entities:
- APC mutation → colonic polyposis + medulloblastoma
- DNA mismatch repair (MMR) gene mutation → Lynch syndrome-type polyposis + glioblastoma multiforme
- Management of CRC risk differs depending on which gene is mutated
5. MUTYH-Associated Polyposis (MAP)
- Usually 5-100 colonic adenomas (florid polyposis can occur)
- Phenotype appears later than classic FAP
- CRC risk is high (usually microsatellite-stable tumors)
- Extra-colonic: gastric cancer, duodenal adenomas, CHRPE, osteomas
6. Polymerase Proofreading-Associated Polyposis (PPAP)
- Genes: POLE or POLD1 (DNA polymerase subunits); autosomal dominant
- "Ultramutator" phenotype; typically <100 colonic adenomas
- High CRC risk; endometrial cancer (especially POLD1 mutations)
7. NTHL1-Associated Polyposis
- Gene: NTHL1 (base-excision repair gene, similar to MUTYH); autosomal recessive
- ~50 colonic adenomas in adulthood; high CRC risk
- Broader extra-colonic spectrum: endometrial, breast, and skin cancers
- Management similar to MAP
II. Serrated Polyposis Syndrome
- Also formerly called hyperplastic polyposis syndrome
- Characterized by multiple serrated polyps (hyperplastic, sessile serrated, or traditional serrated adenomas) throughout the colon
- Associated with increased CRC risk, particularly through the serrated neoplasia pathway (BRAF mutation, CpG island methylation)
- No single gene mutation has been consistently identified
III. Hamartomatous Polyposis Syndromes
| Syndrome | Gene | Polyp Type | GI Location | Key Extra-intestinal Features |
|---|---|---|---|---|
| Peutz-Jeghers | STK11/LKB1 | Hamartoma (smooth muscle core) | Small intestine, stomach, colon | Mucocutaneous pigmentation; breast, pancreatic, ovarian, GI cancers |
| Juvenile polyposis | SMAD4, BMPR1A, ENG | Juvenile polyps (dilated crypts) | Colon, small intestine, stomach | Colon cancer; congenital abnormalities; HHT phenotype (SMAD4) |
| Cowden disease | PTEN | Hamartomas (disorganized muscularis mucosae) | Stomach, colon | Trichilemmomas; breast + thyroid cancer |
| Bannayan-Ruvalcaba-Riley | PTEN | Juvenile polyps | Colon | Macrocephaly; developmental delay; pigmented penile spots |
Peutz-Jeghers Syndrome (PJS)
Juvenile Polyposis Syndrome (JPS)
- Most common hamartomatous syndrome (incidence 1 per 100,000)
- Polyps in colon, small intestine, and stomach
- Significant CRC risk; upper GI surveillance required for SMAD4 carriers
- ~30% of patients have congenital abnormalities
- SMAD4 carriers: risk of hereditary hemorrhagic telangiectasia (HHT) phenotype
Cowden Syndrome (PTEN Hamartoma Tumor Syndrome)
- Trichilemmomas (benign hair follicle tumors) - pathognomonic
- Oral papillomas
- Increased risk of breast cancer (25-50% lifetime) and thyroid cancer
- Macrocephaly
IV. Non-inherited Polyposis
Cronkhite-Canada Syndrome
- Acquired (non-inherited), extremely rare
- Diffuse GI hamartomatous polyposis with characteristic ectodermal changes: alopecia, nail dystrophy, hyperpigmentation of the skin
- Associated with protein-losing enteropathy, diarrhea, and malabsorption
Key Comparisons at a Glance
| Feature | FAP | MAP | PJS | JPS |
|---|---|---|---|---|
| Gene | APC | MUTYH | STK11 | SMAD4/BMPR1A |
| Inheritance | AD | AR | AD | AD |
| Polyp type | Adenoma | Adenoma | Hamartoma | Hamartoma (juvenile) |
| No. of polyps | >100 to thousands | 5-100 (usually) | Hundreds (small bowel >> colon) | Multiple (usually <100) |
| CRC risk | ~100% | High | ~40% (all cancers) | High |
| Key extra-colonic finding | Osteomas, CHRPE, desmoids | CHRPE, osteomas | Mucocutaneous pigmentation | Congenital anomalies (HHT if SMAD4) |
| Screening start | Age 10-12 | Age 25 | Infancy (testicular) | Childhood |
Make it into a ppt
ls /home/daytona/workspace/
mkdir -p /home/daytona/workspace/colonic-polyposis-ppt
~/colonic-polyposis-ppt/make_ppt.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ─── Fetch images ────────────────────────────────────────────────────────────
const imgUrls = [
"https://cdn.orris.care/cdss_images/4566501cb12efb4d13ba792e8d3b323765e3f865ccf89212e397314585ec27d6.png",
"https://cdn.orris.care/cdss_images/a38620b7eb609e06e2c1fb5c2cc5b8702b5f219d4409081cd0f096506b3f427d.png"
];
const imgs = JSON.parse(
execSync(
`node /home/daytona/skills/shared/scripts/fetch_images.js ${imgUrls.map(u => `"${u}"`).join(" ")}`
).toString()
);
const [adenomaImg, juvenileImg] = imgs;
// ─── Palette ─────────────────────────────────────────────────────────────────
const C = {
navy: "0D2B45",
teal: "1A7A6E",
mint: "2FB8A0",
amber: "E8A020",
gold: "F5C842",
white: "FFFFFF",
offwhite:"F4F7FA",
ltgray: "D6E4EF",
midgray: "7A97B0",
dark: "0A1E30",
red: "C0392B",
orange: "E67E22",
purple: "7B3FA0",
green: "27AE60"
};
let pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Colonic Polyposis Syndromes";
pres.author = "Orris Medical";
// ─── Helper: section header bar ──────────────────────────────────────────────
function addHeaderBar(slide, text, barColor) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.72,
fill: { color: barColor || C.navy },
line: { color: barColor || C.navy }
});
slide.addText(text, {
x: 0.3, y: 0, w: 9.4, h: 0.72,
fontSize: 22, bold: true, color: C.white,
valign: "middle", margin: 0
});
}
// ─── Helper: footer ──────────────────────────────────────────────────────────
function addFooter(slide, note) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 5.35, w: 10, h: 0.275,
fill: { color: C.navy }, line: { color: C.navy }
});
slide.addText(note || "Colonic Polyposis Syndromes | Orris Medical", {
x: 0.2, y: 5.35, w: 9.6, h: 0.275,
fontSize: 8, color: C.ltgray, valign: "middle", margin: 0
});
}
// ─── Helper: info card ───────────────────────────────────────────────────────
function addCard(slide, x, y, w, h, title, titleColor, body) {
slide.addShape(pres.shapes.RECTANGLE, {
x, y, w, h,
fill: { color: C.white },
line: { color: C.ltgray, width: 0.5 },
shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.08 }
});
// title bar
slide.addShape(pres.shapes.RECTANGLE, {
x, y, w, h: 0.32,
fill: { color: titleColor || C.teal },
line: { color: titleColor || C.teal }
});
slide.addText(title, {
x: x + 0.08, y, w: w - 0.16, h: 0.32,
fontSize: 9.5, bold: true, color: C.white,
valign: "middle", margin: 0
});
// body bullets
if (body && body.length) {
const items = body.map((b, i) => ({
text: b,
options: { bullet: { type: "bullet" }, breakLine: i < body.length - 1, fontSize: 8.5, color: C.navy }
}));
slide.addText(items, {
x: x + 0.1, y: y + 0.36, w: w - 0.2, h: h - 0.44,
valign: "top", margin: 0
});
}
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 1 — Title
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
// Full background
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 5.625,
fill: { color: C.dark }, line: { color: C.dark }
});
// Accent stripe
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 0.18, h: 5.625,
fill: { color: C.mint }, line: { color: C.mint }
});
// Bottom bar
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 4.9, w: 10, h: 0.725,
fill: { color: C.teal }, line: { color: C.teal }
});
s.addText("COLONIC POLYPOSIS SYNDROMES", {
x: 0.5, y: 1.5, w: 9, h: 1.0,
fontSize: 36, bold: true, color: C.white,
align: "center", charSpacing: 2
});
s.addText("Classification • Genetics • Clinical Features • Management", {
x: 0.5, y: 2.65, w: 9, h: 0.5,
fontSize: 16, color: C.mint, align: "center", italic: true
});
s.addShape(pres.shapes.RECTANGLE, {
x: 3.5, y: 3.3, w: 3, h: 0.03,
fill: { color: C.gold }, line: { color: C.gold }
});
s.addText("Sleisenger & Fordtran • Robbins & Kumar • Sabiston • Yamada", {
x: 0.5, y: 4.92, w: 9, h: 0.5,
fontSize: 9, color: C.white, align: "center", italic: true
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 2 — Overview / Classification
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "Overview: Classification of GI Polyposis Syndromes", C.navy);
addFooter(s);
const cats = [
{ label: "ADENOMATOUS", color: C.teal, items: ["Classic FAP", "Attenuated FAP (AFAP)", "Gardner Syndrome", "Turcot Syndrome", "MAP (MUTYH)", "PPAP (POLE/POLD1)", "NTHL1 Polyposis"] },
{ label: "SERRATED", color: C.orange, items: ["Serrated Polyposis Syndrome", "(formerly Hyperplastic\nPolyposis Syndrome)"] },
{ label: "HAMARTOMATOUS", color: C.purple, items: ["Peutz-Jeghers Syndrome", "Juvenile Polyposis", "Cowden Disease (PTEN)", "Bannayan-Ruvalcaba-Riley Syndrome"] },
{ label: "NON-INHERITED", color: C.midgray, items: ["Cronkhite-Canada Syndrome", "Lymphomatous Polyposis", "Nodular Lymphoid Hyperplasia"] }
];
const xs = [0.15, 2.65, 5.15, 7.65];
const w = 2.3;
cats.forEach((cat, i) => {
const x = xs[i];
s.addShape(pres.shapes.RECTANGLE, {
x, y: 0.85, w, h: 4.35,
fill: { color: C.white },
line: { color: C.ltgray, width: 0.5 },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.1 }
});
s.addShape(pres.shapes.RECTANGLE, {
x, y: 0.85, w, h: 0.4,
fill: { color: cat.color }, line: { color: cat.color }
});
s.addText(cat.label, {
x: x + 0.08, y: 0.85, w: w - 0.16, h: 0.4,
fontSize: 10, bold: true, color: C.white,
valign: "middle", align: "center", margin: 0
});
const items = cat.items.map((t, idx) => ({
text: t,
options: { bullet: { type: "bullet", characterCode: "25B6" }, breakLine: idx < cat.items.length - 1, fontSize: 9, color: C.navy }
}));
s.addText(items, {
x: x + 0.1, y: 1.3, w: w - 0.2, h: 3.8,
valign: "top", margin: 0
});
});
s.addText("Most polyposis syndromes are inherited and carry significant CRC or extra-intestinal cancer risk", {
x: 0.15, y: 5.08, w: 9.7, h: 0.26,
fontSize: 8, italic: true, color: C.midgray, align: "center"
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 3 — FAP: Genetics & Pathogenesis
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "Familial Adenomatous Polyposis (FAP): Genetics & Pathogenesis", C.teal);
addFooter(s);
// Left panel
s.addShape(pres.shapes.RECTANGLE, {
x: 0.15, y: 0.85, w: 4.6, h: 4.35,
fill: { color: C.white }, line: { color: C.ltgray, width: 0.5 },
shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.08 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0.15, y: 0.85, w: 4.6, h: 0.35,
fill: { color: C.teal }, line: { color: C.teal }
});
s.addText("GENETICS", { x: 0.23, y: 0.85, w: 4.44, h: 0.35, fontSize: 10, bold: true, color: C.white, valign: "middle", margin: 0 });
const genItems = [
{ text: "Gene: APC (Adenomatous Polyposis Coli) on chromosome 5q21", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Most mutations between codons 168–1640; key codons: 1061 & 1309", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Inheritance: Autosomal dominant, penetrance 80–100%", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Prevalence: 1 in 5,000–7,500", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "20–25% arise from de novo mutations (no family history)", options: { bullet: true, breakLine: true, fontSize: 9, color: C.orange, bold: true } },
{ text: "Pathogenesis: APC is a key negative regulator of Wnt signaling. One mutant allele inherited; second allele lost somatically → adenoma formation (two-hit hypothesis)", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "APC protein: 300 kDa scaffolding protein; promotes β-catenin degradation", options: { bullet: true, fontSize: 9, color: C.navy } }
];
s.addText(genItems, { x: 0.25, y: 1.24, w: 4.4, h: 3.85, valign: "top", margin: 0 });
// Right panel
s.addShape(pres.shapes.RECTANGLE, {
x: 5.0, y: 0.85, w: 4.85, h: 4.35,
fill: { color: C.white }, line: { color: C.ltgray, width: 0.5 },
shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.08 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 5.0, y: 0.85, w: 4.85, h: 0.35,
fill: { color: C.navy }, line: { color: C.navy }
});
s.addText("COLONIC FEATURES", { x: 5.08, y: 0.85, w: 4.68, h: 0.35, fontSize: 10, bold: true, color: C.white, valign: "middle", margin: 0 });
const colonItems = [
{ text: "Classic FAP: >100 synchronous adenomas (thousands possible)", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Polyps predominate in rectum and left colon", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Present by age 10 in ~15% of patients; 75% by age 20", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Morphologically identical to sporadic adenomas", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Flat/depressed adenomas and microscopic adenomas also common", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "CRC risk approaches 100% if untreated; typically by age 35–40", options: { bullet: true, breakLine: true, fontSize: 9.5, color: C.red, bold: true } },
{ text: "Symptoms: bleeding, diarrhea, abdominal pain, mucous discharge", options: { bullet: true, fontSize: 9, color: C.navy } }
];
s.addText(colonItems, { x: 5.1, y: 1.24, w: 4.65, h: 3.85, valign: "top", margin: 0 });
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 4 — FAP Extracolonic Manifestations
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "FAP: Extracolonic Manifestations & Surveillance", C.teal);
addFooter(s);
// Left: GI + extra-GI
addCard(s, 0.15, 0.85, 4.6, 2.3, "EXTRA-INTESTINAL GI DISEASE", C.teal, [
"Duodenal adenomas: >95% of FAP patients (periampullary region)",
"Duodenal cancer in 5–10% — 2nd leading cause of FAP death",
"Gastric fundic gland polyps: 30–90% (low malignant potential)",
"Gastric adenomas: 10–30% (antrum; higher in Asian populations)",
"Spiegelman staging guides surveillance intervals"
]);
addCard(s, 0.15, 3.25, 4.6, 1.9, "CAUSE OF DEATH IN FAP", C.red, [
"1st: Metastatic colorectal carcinoma",
"2nd: Duodenal / periampullary adenocarcinoma",
"3rd: Desmoid tumors (locally invasive fibromatoses)"
]);
// Right: non-GI
addCard(s, 5.0, 0.85, 4.85, 2.3, "BENIGN EXTRA-INTESTINAL LESIONS", C.navy, [
"Osteomas (mandible, skull, long bones): 50–90%",
"CHRPE (detectable at birth): 70–80%",
"Epidermoid / sebaceous cysts: 50%",
"Fibromas: 25–50%",
"Desmoid tumors: 10–24%",
"Dental abnormalities / supernumerary teeth"
]);
addCard(s, 5.0, 3.25, 4.85, 1.9, "MALIGNANT EXTRA-INTESTINAL", C.orange, [
"Papillary thyroid carcinoma: 2–3%",
"Hepatoblastoma (childhood)",
"Medulloblastoma (Turcot variant)",
"Adrenal tumors"
]);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 5 — FAP Endoscopy Image + Histology
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "FAP: Adenoma Morphology", C.teal);
addFooter(s);
if (adenomaImg && !adenomaImg.error) {
s.addImage({ data: adenomaImg.base64, x: 0.3, y: 0.85, w: 9.4, h: 4.05 });
}
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 4.9, w: 10, h: 0.45, fill: { color: "00000088" }, line: { color: "00000088" } });
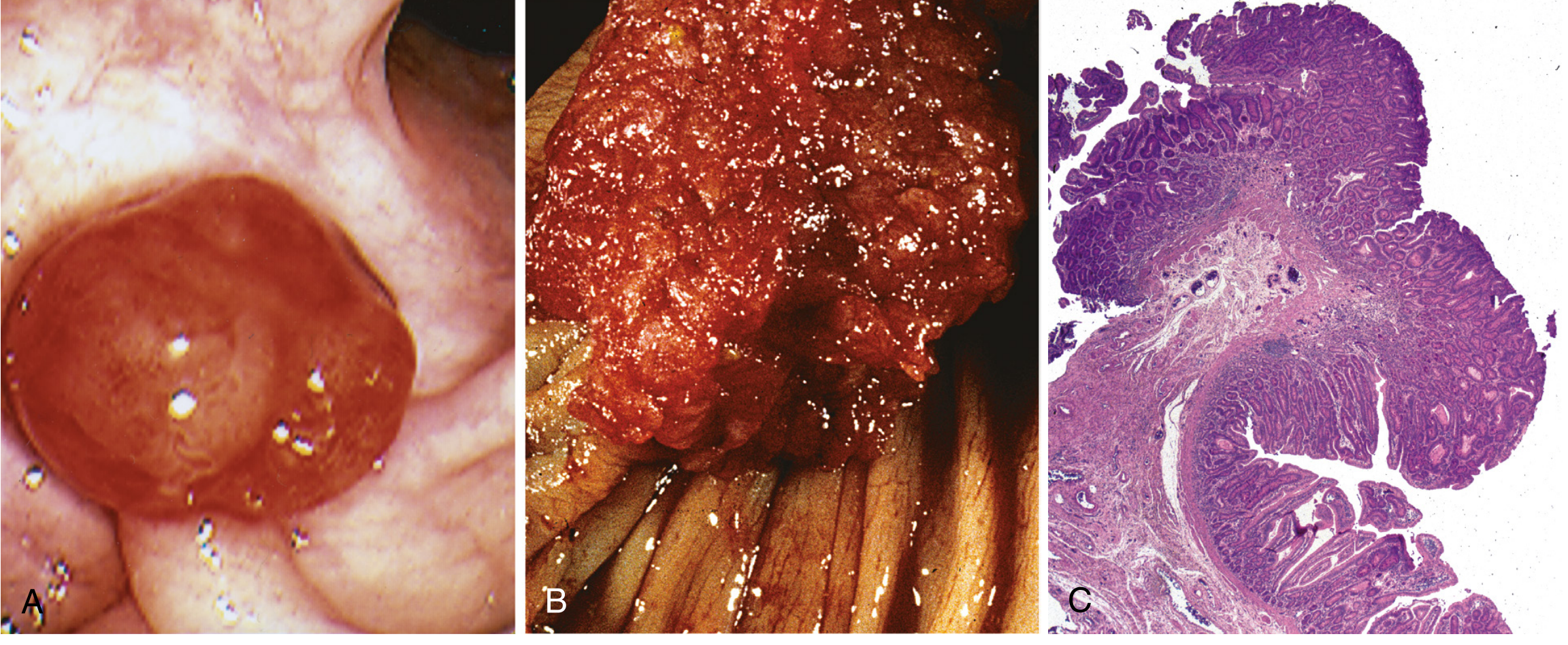
s.addText(
"(A) Pedunculated adenoma (endoscopy) | (B) Adenoma with velvety surface | (C) Histology: tubular adenoma (low-power) — Robbins & Kumar Pathologic Basis of Disease",
{ x: 0.2, y: 4.9, w: 9.6, h: 0.45, fontSize: 8, color: C.white, align: "center", valign: "middle", italic: true }
);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 6 — FAP Surgery & Screening
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "FAP: Surgical Management & Screening", C.teal);
addFooter(s);
// Surgical options table
s.addShape(pres.shapes.RECTANGLE, {
x: 0.15, y: 0.85, w: 9.7, h: 0.38,
fill: { color: C.teal }, line: { color: C.teal }
});
["Procedure", "Indication", "Comment"].forEach((h, i) => {
s.addText(h, {
x: [0.2, 3.55, 6.95][i], y: 0.85, w: [3.2, 3.2, 2.85][i], h: 0.38,
fontSize: 9.5, bold: true, color: C.white, valign: "middle", margin: 4
});
});
const rows = [
["Total Abdominal Colectomy + IRA", "Colon cancer; rectum <20 polyps", "Rectum managed endoscopically"],
["Total Proctocolectomy + IPAA", "Profuse polyposis; rectal cancer;\nrectal polyps >20", "Stapled anastomosis if anal transition zone clear"],
["Pancreas-sparing Duodenectomy", "Spiegelman Stage IV duodenal disease", "Expert centers only"]
];
rows.forEach((row, ri) => {
const y = 1.23 + ri * 0.72;
const bg = ri % 2 === 0 ? C.white : "EAF4F1";
s.addShape(pres.shapes.RECTANGLE, { x: 0.15, y, w: 9.7, h: 0.7, fill: { color: bg }, line: { color: C.ltgray, width: 0.5 } });
row.forEach((cell, ci) => {
s.addText(cell, {
x: [0.2, 3.55, 6.95][ci], y, w: [3.2, 3.2, 2.85][ci], h: 0.7,
fontSize: 8.5, color: C.navy, valign: "middle", margin: 4
});
});
});
// Screening panel
s.addShape(pres.shapes.RECTANGLE, {
x: 0.15, y: 3.45, w: 9.7, h: 0.35,
fill: { color: C.navy }, line: { color: C.navy }
});
s.addText("SCREENING SCHEDULE", {
x: 0.25, y: 3.45, w: 9.5, h: 0.35,
fontSize: 10, bold: true, color: C.white, valign: "middle", margin: 0
});
const screenItems = [
["Age 10–12 yrs", "Annual colonoscopy (or flexible sigmoidoscopy if known FAP)"],
["Age 20–25 yrs", "Upper endoscopy (EGD with side-viewer for periampullary region)"],
["Ongoing", "Annual thyroid ultrasound | Desmoid awareness | Spiegelman duodenal staging"]
];
screenItems.forEach((item, i) => {
const y = 3.84 + i * 0.36;
s.addShape(pres.shapes.RECTANGLE, {
x: 0.15, y, w: 1.6, h: 0.34,
fill: { color: C.mint }, line: { color: C.mint }
});
s.addText(item[0], { x: 0.2, y, w: 1.5, h: 0.34, fontSize: 8.5, bold: true, color: C.dark, valign: "middle", align: "center", margin: 0 });
s.addText(item[1], { x: 1.85, y, w: 7.9, h: 0.34, fontSize: 8.5, color: C.navy, valign: "middle", margin: 4 });
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 7 — FAP Variants (AFAP, Gardner, Turcot)
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "FAP Variants: AFAP, Gardner Syndrome, Turcot Syndrome", C.navy);
addFooter(s);
addCard(s, 0.15, 0.85, 3.1, 4.3, "ATTENUATED FAP (AFAP)", C.teal, [
"Same APC gene — mutations at 5' or 3' ends",
"<100 adenomas (usually fewer)",
"Flat polyp growth pattern",
"Proximal colon predominance",
"Presents in adulthood (not adolescence)",
"CRC risk still high but onset ≥55 years",
"Colonoscopy every 1–2 years from age 25",
"Same upper GI surveillance as classic FAP"
]);
addCard(s, 3.45, 0.85, 3.1, 4.3, "GARDNER SYNDROME", C.orange, [
"APC gene variant — same locus as FAP",
"Classic FAP + prominent extracolonic features",
"Prominent osteomas (mandible, skull)",
"Epidermoid cysts",
"Desmoid tumors (mesentery, abdominal wall)",
"Supernumerary teeth / dental anomalies",
"Now considered a phenotypic variant of FAP, NOT a separate entity"
]);
addCard(s, 6.75, 0.85, 3.1, 4.3, "TURCOT SYNDROME", C.purple, [
"Colonic polyposis + primary CNS tumors",
"Two distinct genetic subtypes:",
" APC mutation → FAP-like polyposis + medulloblastoma",
" MMR gene mutation → Lynch-type colonic lesions + glioblastoma multiforme",
"CRC management depends on which mutation is present",
"Brain tumor screening for mutation-positive family members"
]);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 8 — MAP, PPAP, NTHL1
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "Other Adenomatous Polyposis Syndromes: MAP, PPAP, NTHL1", C.navy);
addFooter(s);
// MAP left + center
s.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 0.85, w: 6.3, h: 4.3, fill: { color: C.white }, line: { color: C.ltgray, width: 0.5 }, shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.08 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.15, y: 0.85, w: 6.3, h: 0.35, fill: { color: C.teal }, line: { color: C.teal } });
s.addText("MUTYH-ASSOCIATED POLYPOSIS (MAP)", { x: 0.23, y: 0.85, w: 6.12, h: 0.35, fontSize: 10, bold: true, color: C.white, valign: "middle", margin: 0 });
const mapItems = [
{ text: "Gene: MUTYH (MYH) — base-excision repair gene", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Inheritance: AUTOSOMAL RECESSIVE — unique among polyposis syndromes", options: { bullet: true, breakLine: true, fontSize: 9, color: C.red, bold: true } },
{ text: "Common mutations: Y179C and G396D", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Pathogenesis: Defective MUTYH → G:C→T:A transversions → somatic APC loss → adenomas", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "5–100 adenomas (usually); florid polyposis can occur; later onset than FAP", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Extra-colonic: CHRPE, osteomas, gastric cancer, duodenal adenomas", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "CRC risk: HIGH (MSS tumors); colonoscopy every 1–2 yrs from age 25", options: { bullet: true, breakLine: true, fontSize: 9, color: C.navy } },
{ text: "Test all patients with >10 adenomas for biallelic MUTYH mutations", options: { bullet: true, breakLine: true, fontSize: 9, color: C.orange } },
{ text: "Genetic counseling → directed toward SIBLINGS (not parents/children)", options: { bullet: true, fontSize: 9, color: C.purple, bold: true } }
];
s.addText(mapItems, { x: 0.25, y: 1.24, w: 6.1, h: 3.85, valign: "top", margin: 0 });
// PPAP + NTHL1 right column
addCard(s, 6.6, 0.85, 3.25, 2.0, "PPAP (POLE / POLD1)", C.orange, [
"Autosomal dominant",
"'Ultramutator' phenotype",
"<100 colonic adenomas",
"High CRC + endometrial cancer risk (POLD1)"
]);
addCard(s, 6.6, 3.0, 3.25, 2.15, "NTHL1 POLYPOSIS", C.purple, [
"Autosomal recessive (like MAP)",
"~50 adenomas in adulthood",
"High CRC risk",
"Broader extra-colonic: endometrial,\nbreast, skin cancers",
"Management similar to MAP"
]);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 9 — Peutz-Jeghers Syndrome
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "Peutz-Jeghers Syndrome (PJS)", C.purple);
addFooter(s);
addCard(s, 0.15, 0.85, 3.0, 4.3, "GENETICS", C.purple, [
"Gene: STK11/LKB1 (serine-threonine kinase)",
"Chromosome 19p",
"Autosomal dominant, variable penetrance",
"80% of families have identifiable STK11 mutation",
"STK11 regulates AMPK — controls cell polarization and growth"
]);
addCard(s, 3.3, 0.85, 3.3, 4.3, "CLINICAL FEATURES", C.navy, [
"Mucocutaneous pigmentation in 95%:",
" Lips, buccal mucosa (pathognomonic), hands, feet, genitalia, perianal",
" Dark melanin deposits, appear in infancy",
"GI polyps: predominantly small intestine, also stomach & colon",
"Risk of intussusception (can be fatal)",
"Polyp histology: arborizing smooth muscle network + normal epithelium"
]);
addCard(s, 6.75, 0.85, 3.1, 4.3, "CANCER RISKS (~40% lifetime)", C.red, [
"Colorectal cancer",
"Gastric & small intestinal cancer",
"Pancreatic cancer (highest relative risk)",
"Breast cancer",
"Ovarian, uterine, lung cancer",
"Sex cord tumors (testes)",
"Surveillance from BIRTH (testicular) through adulthood"
]);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 10 — Juvenile Polyposis + Histology Image
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "Juvenile Polyposis Syndrome (JPS)", C.purple);
addFooter(s);
addCard(s, 0.15, 0.85, 4.5, 4.3, "GENETICS & FEATURES", C.purple, [
"Genes: SMAD4 (chr 18q) and BMPR1A (chr 10q22) — both TGF-β pathway",
"Inheritance: Autosomal dominant",
"Most common hamartomatous syndrome (1 per 100,000)",
"Polyp histology: cystically dilated crypts, edematous lamina propria, surface erosion",
"SMAD4 mutations (~20–25%): higher malignancy potential, massive gastric polyposis",
"BMPR1A mutations (~20%): similar but less severe gastric involvement",
"ENG mutations: associated with Hereditary Hemorrhagic Telangiectasia (HHT)",
"30% of patients have congenital abnormalities",
"CRC risk: HIGH — colonoscopic surveillance from childhood",
"Upper GI endoscopy required for SMAD4 mutation carriers"
]);
if (juvenileImg && !juvenileImg.error) {
s.addImage({ data: juvenileImg.base64, x: 4.85, y: 0.85, w: 4.9, h: 3.25 });
}
s.addShape(pres.shapes.RECTANGLE, { x: 4.85, y: 4.1, w: 4.9, h: 0.5, fill: { color: C.dark }, line: { color: C.dark } });
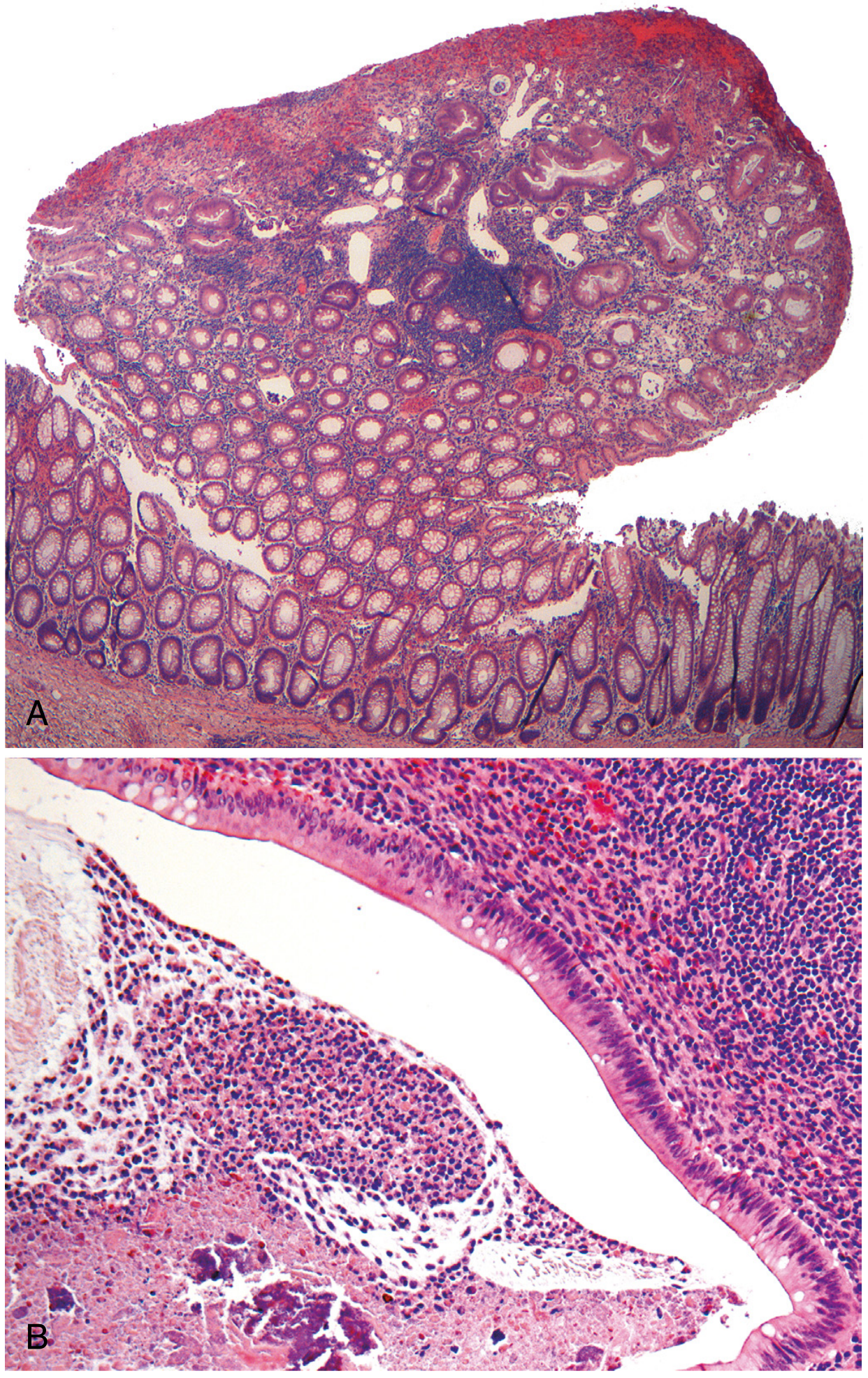
s.addText("(A) Juvenile polyp: cystically dilated crypts | (B) Dilated crypts with inspissated mucus and inflammatory cells — Robbins & Kumar", {
x: 4.95, y: 4.1, w: 4.7, h: 0.5,
fontSize: 7.5, color: C.white, align: "center", valign: "middle", italic: true
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 11 — Cowden + Serrated + Cronkhite-Canada
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "Cowden Syndrome, Serrated Polyposis & Cronkhite-Canada", C.navy);
addFooter(s);
addCard(s, 0.15, 0.85, 3.1, 4.3, "COWDEN SYNDROME\n(PTEN Hamartoma)", C.purple, [
"Gene: PTEN (tumor suppressor)",
"Autosomal dominant",
"Multiple GI hamartomas (stomach + colon predominant)",
"Hallmark: Trichilemmomas (benign hair follicle tumors — pathognomonic)",
"Oral papillomas",
"Macrocephaly",
"Breast cancer risk: 25–50% lifetime",
"Thyroid cancer (follicular)",
"Bannayan-Riley-Ruvalcaba: PTEN variant with macrocephaly + penile pigmentation"
]);
addCard(s, 3.45, 0.85, 3.1, 4.3, "SERRATED POLYPOSIS\nSYNDROME", C.orange, [
"Multiple serrated polyps throughout colon",
"Types: hyperplastic, sessile serrated, traditional serrated adenomas",
"No single causative gene identified",
"Pathway: BRAF mutation + CpG island methylator phenotype (CIMP)",
"Significant CRC risk — through serrated neoplasia pathway",
"WHO criteria: ≥5 serrated polyps proximal to sigmoid, ≥2 with diameter ≥10 mm",
"Regular colonoscopic surveillance required"
]);
addCard(s, 6.75, 0.85, 3.1, 4.3, "CRONKHITE-CANADA\nSYNDROME", C.midgray, [
"NON-inherited (acquired) — extremely rare",
"Diffuse GI hamartomatous polyposis",
"Characteristic ECTODERMAL triad:",
" Alopecia (hair loss)",
" Nail dystrophy (onychodystrophy)",
" Skin hyperpigmentation",
"Protein-losing enteropathy, diarrhea, malabsorption",
"Not classified as a genetic syndrome"
]);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 12 — Comparison Table
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offwhite }, line: { color: C.offwhite } });
addHeaderBar(s, "Comparison: Key Polyposis Syndromes at a Glance", C.navy);
addFooter(s);
const headers = ["Feature", "FAP", "AFAP", "MAP", "PJS", "JPS", "Cowden"];
const colW = [1.35, 1.35, 1.35, 1.35, 1.35, 1.35, 1.35];
const startX = 0.1;
const rows = [
["Gene", "APC", "APC (5'/3')", "MUTYH", "STK11", "SMAD4/BMPR1A", "PTEN"],
["Inheritance", "AD", "AD", "AR ⬅", "AD", "AD", "AD"],
["Polyp type", "Adenoma", "Adenoma", "Adenoma", "Hamartoma", "Hamartoma (juvenile)", "Hamartoma"],
["Polyp count", ">100–1000s", "<100", "5–100", "Multiple (SI>>colon)", "Multiple", "Multiple"],
["CRC risk", "~100%", "High", "High", "~40% (all Ca)", "High", "Moderate"],
["Key finding", "Osteomas, CHRPE, desmoids", "Proximal colon, flat polyps", "AR; CHRPE", "Mucocut. pigment", "Congenital anomalies", "Trichilemmomas"],
["Screen age", "10–12 yrs", "25 yrs", "25 yrs", "Birth (testicular)", "Childhood", "Adult"]
];
// Header row
s.addShape(pres.shapes.RECTANGLE, { x: startX, y: 0.82, w: 9.8, h: 0.36, fill: { color: C.navy }, line: { color: C.navy } });
headers.forEach((h, i) => {
s.addText(h, {
x: startX + i * colW[i], y: 0.82, w: colW[i], h: 0.36,
fontSize: 8.5, bold: true, color: C.white, valign: "middle", align: "center", margin: 2
});
});
// Data rows
rows.forEach((row, ri) => {
const y = 1.18 + ri * 0.59;
const bg = ri % 2 === 0 ? C.white : "EEF4F9";
s.addShape(pres.shapes.RECTANGLE, { x: startX, y, w: 9.8, h: 0.57, fill: { color: bg }, line: { color: C.ltgray, width: 0.5 } });
row.forEach((cell, ci) => {
const bold = ci === 0;
const color = (cell.includes("AR") || cell === "~100%") ? C.red : C.navy;
s.addText(cell, {
x: startX + ci * colW[ci], y, w: colW[ci], h: 0.57,
fontSize: ci === 0 ? 8 : 7.8, bold, color,
valign: "middle", align: ci === 0 ? "left" : "center", margin: 3
});
});
});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 13 — Key Take-Aways
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.dark }, line: { color: C.dark } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: C.mint }, line: { color: C.mint } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 4.9, w: 10, h: 0.725, fill: { color: C.teal }, line: { color: C.teal } });
s.addText("KEY TAKE-AWAYS", {
x: 0.5, y: 0.25, w: 9, h: 0.55,
fontSize: 26, bold: true, color: C.gold, align: "center", charSpacing: 3
});
const points = [
{ icon: "▶", text: "FAP (APC gene, chr 5q21) carries near-100% lifetime CRC risk if untreated; prophylactic colectomy is standard of care" },
{ icon: "▶", text: "De novo mutations account for 20–25% of FAP — absence of family history does NOT exclude the diagnosis" },
{ icon: "▶", text: "MUTYH-Associated Polyposis is the only AUTOSOMAL RECESSIVE adenomatous polyposis syndrome; test siblings, not parents/children" },
{ icon: "▶", text: "Turcot syndrome has two distinct subtypes: APC mutation → medulloblastoma; MMR mutation → glioblastoma" },
{ icon: "▶", text: "Peutz-Jeghers (STK11) = hamartomatous polyps + mucocutaneous melanin pigmentation (95%) + ~40% lifetime cancer risk including pancreatic" },
{ icon: "▶", text: "SMAD4 mutations in JPS carry higher gastric polyposis burden and are linked to HHT phenotype; require upper GI surveillance" },
{ icon: "▶", text: "Cowden syndrome (PTEN) = trichilemmomas + high breast/thyroid cancer risk; Cronkhite-Canada is the only non-inherited polyposis" }
];
points.forEach((pt, i) => {
s.addText([
{ text: pt.icon + " ", options: { color: C.gold, bold: true, fontSize: 9.5 } },
{ text: pt.text, options: { color: C.white, fontSize: 9.5 } }
], {
x: 0.4, y: 0.95 + i * 0.52, w: 9.4, h: 0.5,
valign: "middle", margin: 0
});
});
s.addText("Sources: Sleisenger & Fordtran | Robbins & Kumar | Sabiston | Current Surgical Therapy | Yamada's Gastroenterology | Emery's Medical Genetics", {
x: 0.5, y: 4.92, w: 9, h: 0.32,
fontSize: 7.5, color: C.white, align: "center", italic: true
});
}
// ─── Write file ───────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/colonic-polyposis-ppt/Colonic_Polyposis_Syndromes.pptx" })
.then(() => console.log("✅ Done: Colonic_Polyposis_Syndromes.pptx"))
.catch(e => { console.error("Error:", e); process.exit(1); });
cd /home/daytona/workspace/colonic-polyposis-ppt && node make_ppt.js 2>&1
cd /home/daytona/workspace/colonic-polyposis-ppt && node /home/daytona/skills/shared/scripts/fetch_images.js "https://cdn.orris.care/cdss_images/4566501cb12efb4d13ba792e8d3b323765e3f865ccf89212e397314585ec27d6.png" > /tmp/img1.json 2>&1; echo "exit: $?"
node /home/daytona/skills/shared/scripts/fetch_images.js "https://cdn.orris.care/cdss_images/a38620b7eb609e06e2c1fb5c2cc5b8702b5f219d4409081cd0f096506b3f427d.png" > /tmp/img2.json 2>&1; echo "exit: $?"
node -e "const d=JSON.parse(require('fs').readFileSync('/tmp/img1.json')); console.log(d[0].error, d[0].base64 ? d[0].base64.substring(0,60) : 'null')"
~/colonic-polyposis-ppt/make_ppt.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/colonic-polyposis-ppt/make_ppt.js'
~/colonic-polyposis-ppt/make_ppt.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/colonic-polyposis-ppt/make_ppt.js'
cd /home/daytona/workspace/colonic-polyposis-ppt && node make_ppt.js 2>&1
ls -lh /home/daytona/workspace/colonic-polyposis-ppt/Colonic_Polyposis_Syndromes.pptx
Colonic Polyposis Syndromes
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title slide (dark navy + teal) |
| 2 | Full classification overview - 4 category cards |
| 3 | FAP: Genetics & Pathogenesis |
| 4 | FAP: Extracolonic manifestations (GI + non-GI cards) |
| 5 | FAP: Adenoma morphology - real textbook histology image |
| 6 | FAP: Surgical management table + screening schedule |
| 7 | FAP Variants: AFAP, Gardner, Turcot |
| 8 | MAP, PPAP, NTHL1 polyposis |
| 9 | Peutz-Jeghers Syndrome |
| 10 | Juvenile Polyposis - with real histology image of juvenile polyps |
| 11 | Cowden Syndrome, Serrated Polyposis, Cronkhite-Canada |
| 12 | Comparison table (all 6 major syndromes side-by-side) |
| 13 | Key take-aways (dark slide) |