Intussusception in children
Reading File
Finding Sources
Searching PubMed
intussusception children diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
I now have comprehensive content from multiple textbooks. Let me compile the full, well-structured response.
Intussusception in Children
Definition and Mechanism
Intussusception is the telescoping (invagination) of a proximal segment of bowel (the intussusceptum) into a more distal segment (the intussuscipiens), driven by peristaltic force acting on a lead point. This causes mechanical bowel obstruction, followed by venous congestion, bowel wall edema, ischemia, and - if untreated - gangrene and perforation.
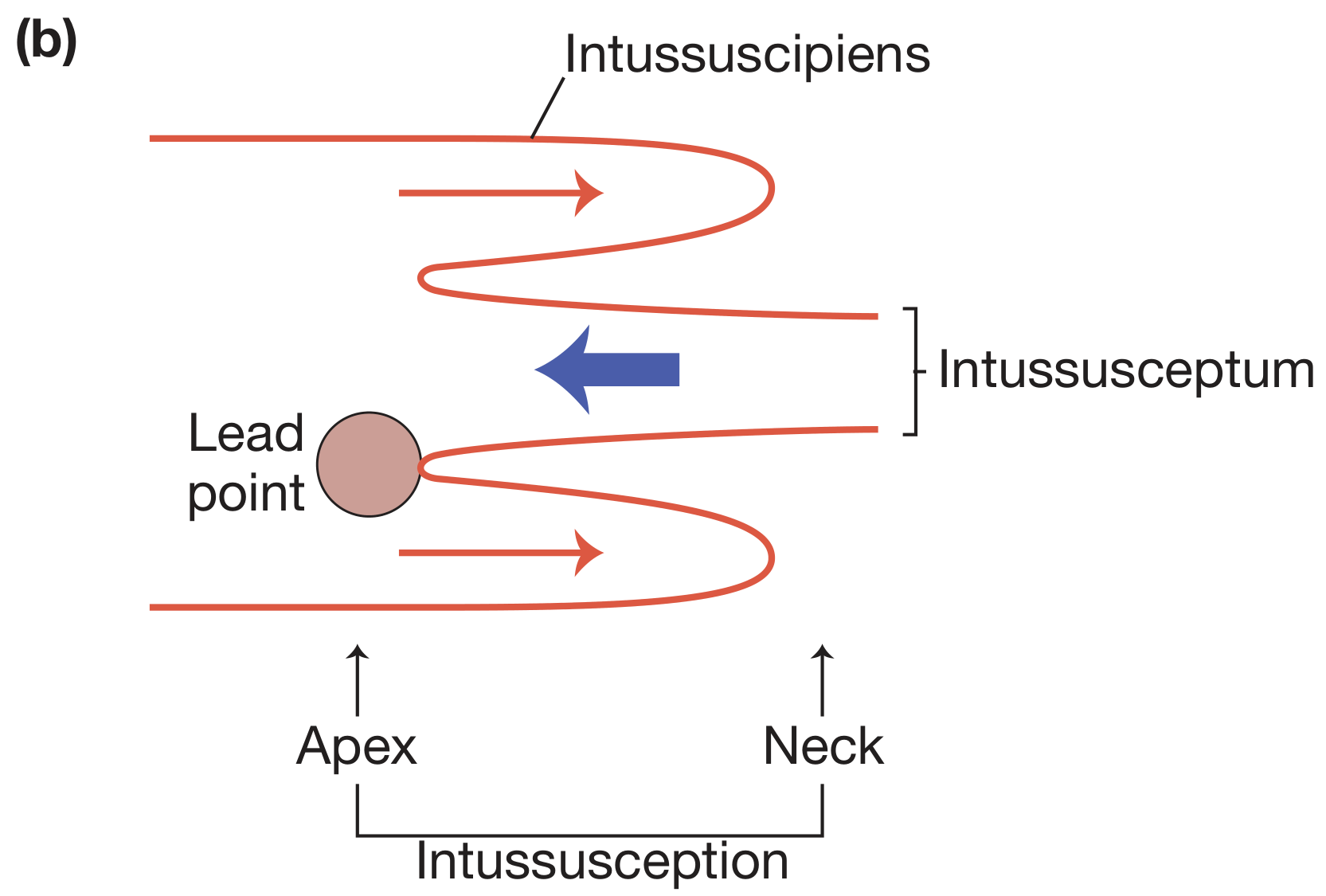
Schematic: the lead point drives the intussusceptum into the intussuscipiens. The apex is the most distal point; the neck is the entry point.
Epidemiology
- Most common cause of intestinal obstruction in children under 2 years; second most common pediatric acute abdomen after appendicitis
- Peak incidence: 5-12 months of age (most series say 5-9 months)
-
50% occur under age 1; <25% occur after age 2
- Male predominance (approximately 3:2)
Types
| Type | Frequency | Notes |
|---|---|---|
| Ileocolic | >80% | Most common; ileum telescopes through ileocecal valve into colon |
| Ileoileocolic | Uncommon | |
| Ileo-ileal | Rare | More likely in HSP; not amenable to enema reduction |
| Colocolic | Rare |
Etiology and Lead Points
Idiopathic (>90% in young children): Caused by hypertrophy of Peyer's patches - typically following a viral infection (gastroenteritis, upper respiratory infection). The rotavirus vaccine has also been implicated in triggering lymphoid swelling.
Pathologic lead points (5-12%): More common in children >5-6 years old and in recurrences. Causes include:
- Meckel's diverticulum (most common pathologic lead point)
- Intestinal polyps
- Intestinal duplication cyst
- Submucosal hemorrhage from Henoch-Schönlein Purpura (HSP)
- Lymphoma
- Appendiceal inflammation
- Foreign body
- Ectopic gastric/pancreatic tissue
- Nasojejunal tubes (iatrogenic)
- Cystic fibrosis, celiac disease, postsurgical adhesions
Clinical Presentation
The classic triad - present together in only a minority of patients:
- Colicky abdominal pain - the most consistent symptom. Episodic, severe, lasting 10-15 minutes with 15-30 minute pain-free intervals; child draws legs up, is inconsolable during attacks, appears well between episodes
- "Currant jelly" stool - bloody mucus stool; a late finding, seen in <50%; indicates bowel ischemia
- Palpable sausage-shaped abdominal mass - in the right upper/mid abdomen; present in <50%
Other features:
- Vomiting (common, initially non-bilious)
- Dehydration
- Lethargy or altered consciousness - an important atypical presentation; can mimic neurologic emergencies
- Pallor
- Progressive abdominal distension
- Signs of shock if presentation is delayed
Differential Diagnosis
| Condition | Distinguishing features |
|---|---|
| Appendicitis | Fever, RLQ tenderness, WBC rise, gradual onset |
| Volvulus | Bilious vomiting, more sudden, neonates |
| Meckel diverticulitis | Painless rectal bleeding typical |
| Gastroenteritis | No obstruction pattern, diarrhea predominates |
| HSP | Rash, arthritis, hematuria |
| Incarcerated hernia | Groin/scrotal mass |
| Testicular/ovarian torsion | Sudden severe pain, groin/pelvic location |
Imaging and Diagnosis
Ultrasound (modality of choice)
Sensitivity and specificity approaching 100% in trained hands. Key findings:
- Target sign / Bull's eye / Doughnut sign - transverse view shows concentric rings of bowel wall (3-5 cm mass)
- Pseudokidney sign / Sandwich sign - longitudinal view showing the intussusceptum protruding into the colon
- Crescent-in-doughnut sign - hyperechoic crescentic mesenteric fat pulled into the intussusceptum
- Lymph nodes and fluid may be visible within the mass
- Look for secondary lead points and free fluid
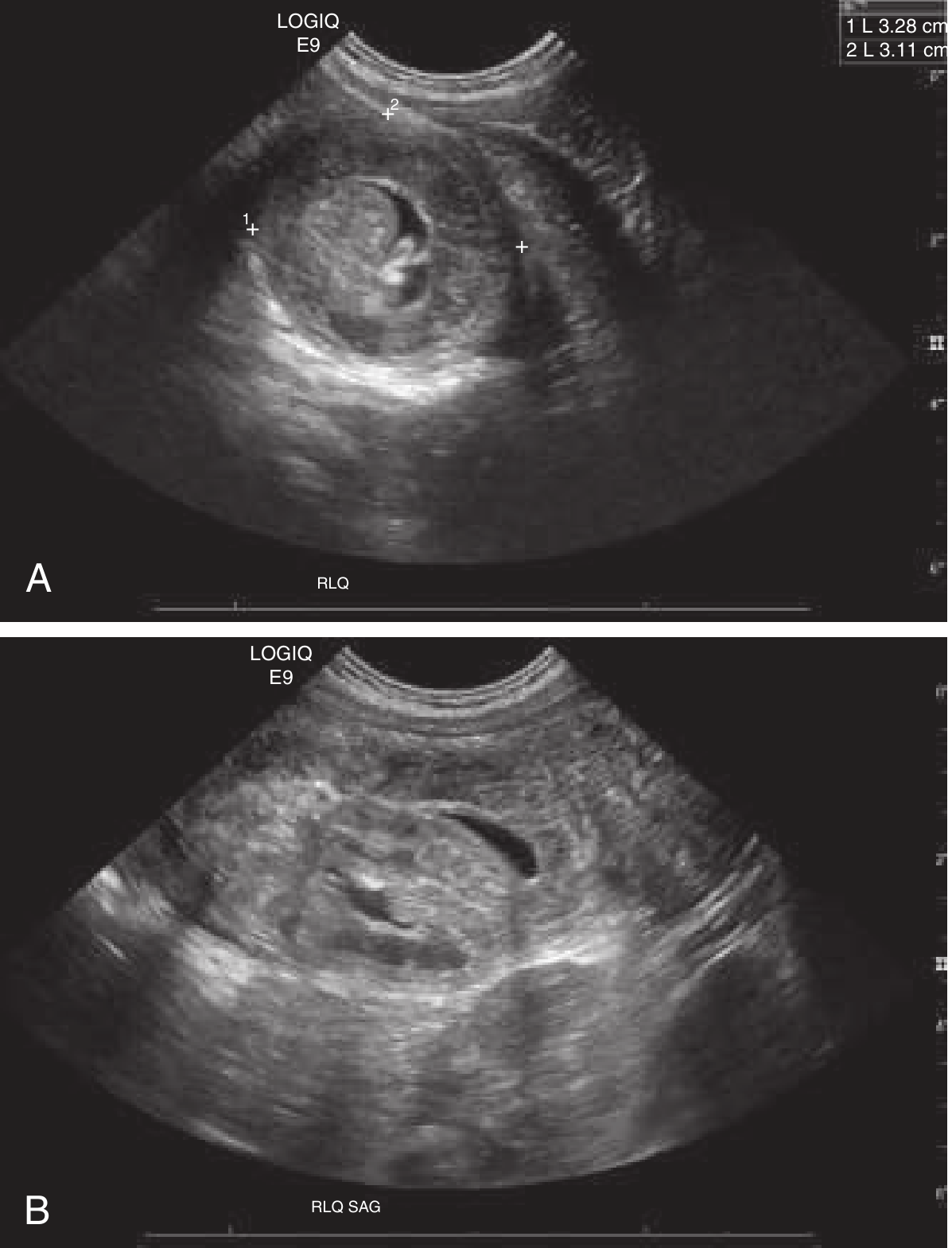
(A) Transverse view: the classic "target sign" - multilayered concentric ring appearance. (B) Longitudinal (sagittal) view: the "pseudokidney sign."
Plain Abdominal Radiograph
Not routinely recommended as a first-line test, but may show:
- Meniscus sign - soft tissue mass contrasting against air-filled bowel
- Paucity of gas in RIF (cecum may be absent from its usual location)
- Dilated proximal small bowel loops (obstruction)
- Free intraperitoneal air (perforation - rare but important to exclude before reduction)
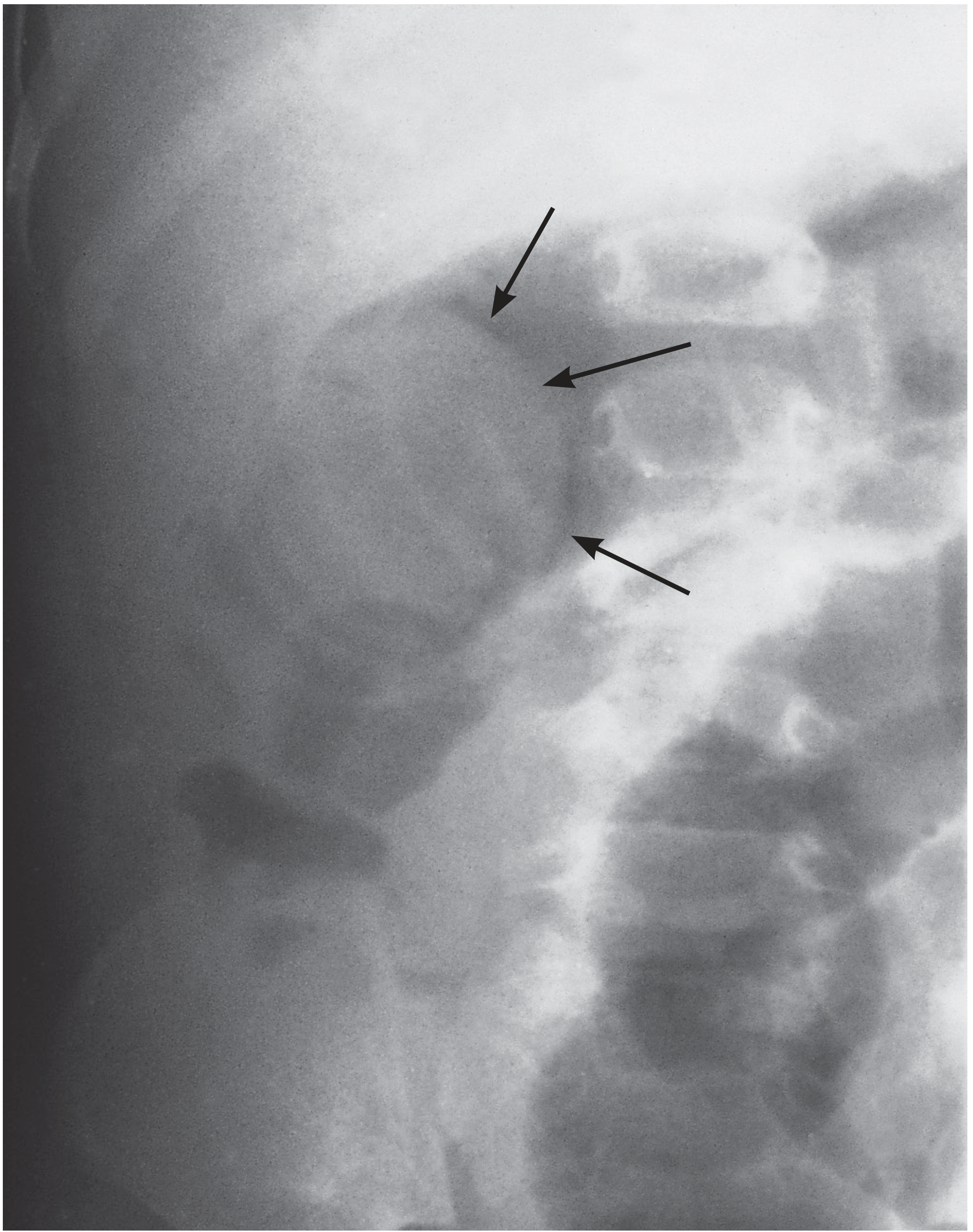
Abdominal X-ray: arrows point to the soft tissue shadow of the intussusceptum producing a meniscus appearance.
Management
Initial Resuscitation
- IV access and fluid boluses (20 mL/kg normal saline) until hemodynamically stable
- NPO, nasogastric tube if vomiting/distended
- Broad-spectrum antibiotics (given risk of ischemic bowel)
- Prompt surgical consultation before any reduction attempt
Non-Operative Reduction (First-line)
Pneumatic (air) enema is preferred at most centers:
- Air is insufflated under fluoroscopic guidance
- Confirms reduction when air flows freely into terminal ileum
- Overall success rate 80-90% for ileocolic intussusception
- Faster, no radiation from contrast, equally efficacious compared to barium/water-soluble enema
Hydrostatic (contrast) enema:
- Barium or water-soluble contrast under fluoroscopic control
- Equivalent success rates
Contraindications to non-operative reduction:
- Free intraperitoneal air (perforation)
- Clinical peritonitis
- Hemodynamic instability / shock
- Entirely small bowel intussusception (not amenable to enema)
Complications: Colonic perforation (rare but can cause tension pneumoperitoneum if air enema).
Operative Management
Indicated when:
- Non-operative reduction fails
- Peritonitis or perforation present
- Hemodynamic instability
- Multiple recurrences (third recurrence)
- Known/suspected pathologic lead point
Technique: Open or laparoscopic. Retrograde squeezing (pushing, not pulling) of the intussusceptum proximally. Bowel viability is assessed after reduction. If non-viable bowel or pathologic lead point: resection + primary anastomosis. The lymphoid tissue at the ileocecal valve may be deliberately excised (incidental appendectomy also done by many surgeons).

Intraoperative photograph of ileocolic intussusception showing the characteristic appearance during surgical reduction.
Recurrence
- After non-operative reduction: ~5-11% recurrence rate, usually within 24-48 hours
- Most recurrences are managed with repeat enema
- A third recurrence is an indication for operative management (to exclude a pathologic lead point and prevent future episodes)
- Observation for 6 hours post-reduction is appropriate; if tolerating oral fluids, discharge is safe
Disposition
- Brief observation (6 hours) after successful non-operative reduction
- Children tolerating oral intake can be discharged home
- Fever is common after reduction and typically resolves without specific treatment
- Return precautions for recurrence symptoms
Key Points Summary
| Feature | Detail |
|---|---|
| Age | Peak 5-12 months; most under 2 years |
| Most common type | Ileocolic (>80%) |
| Most common lead point in >2yr | Meckel's diverticulum |
| Pathognomonic stool | "Currant jelly" (late, <50%) |
| Imaging of choice | Ultrasound (sensitivity/specificity ~100%) |
| Treatment of choice | Pneumatic (air) enema reduction |
| Success rate | 80-90% |
| Recurrence | ~5-11%; repeat enema usually effective |
| Surgery indication | Failed reduction, peritonitis, perforation, shock |
Sources: Rosen's Emergency Medicine (9th ed.) - Ch. 166; Bailey and Love's Surgery (28th ed.) - Ch. 17; Sabiston Textbook of Surgery; Grainger & Allison's Diagnostic Radiology - Ch. 71; Fischer's Mastery of Surgery (8th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.