Heme and bilirubin metabolism
Reading File
Finding Sources
Finding Sources
Searching Images
heme bilirubin metabolism pathway diagram
Finding Sources
Finding Sources
Searching Images
bilirubin conjugation liver jaundice pathway
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive content and excellent diagrams. Let me compile the full answer.
Heme and Bilirubin Metabolism
1. Heme Biosynthesis
Heme synthesis involves eight enzymatic steps converting glycine and succinyl-CoA to heme. These eight enzymes are encoded by nine genes (two genes encode the first enzyme, ALA-synthase). The pathway is split between mitochondria (first and last three enzymes) and cytosol (middle four enzymes).
| Step | Enzyme | Location | Product |
|---|---|---|---|
| 1 | ALA-synthase (ALAS1/ALAS2) | Mitochondria | δ-Aminolevulinic acid (ALA) |
| 2 | ALA-dehydratase | Cytosol | Porphobilinogen (PBG) |
| 3 | HMB-synthase (PBG-deaminase) | Cytosol | Hydroxymethylbilane |
| 4 | Uroporphyrinogen III synthase | Cytosol | Uroporphyrinogen III |
| 5 | Uroporphyrinogen decarboxylase | Cytosol | Coproporphyrinogen III |
| 6 | Coproporphyrinogen oxidase | Mitochondria | Protoporphyrinogen IX |
| 7 | Protoporphyrinogen oxidase | Mitochondria | Protoporphyrin IX |
| 8 | Ferrochelatase | Mitochondria | Heme |
Key points:
- ALA-synthase is the rate-limiting enzyme. It condenses glycine (activated by pyridoxal phosphate) + succinyl-CoA → ALA.
- ALAS1 (housekeeping, chromosome 3p21.1) is induced in the liver by drugs, steroids, and chemicals.
- ALAS2 (erythroid-specific, chromosome Xp11.2): loss-of-function → X-linked sideroblastic anemia (XLSA); gain-of-function → X-linked erythropoietic protoporphyria (XLP).
- ~85% of daily heme synthesis occurs in erythroid precursors (for hemoglobin); hepatocytes account for most of the remainder (primarily for CYP450 enzymes).
— Harrison's Principles of Internal Medicine 22E, p. 3386; Tietz Textbook of Laboratory Medicine 7e
2. Heme Catabolism: Heme → Biliverdin → Bilirubin
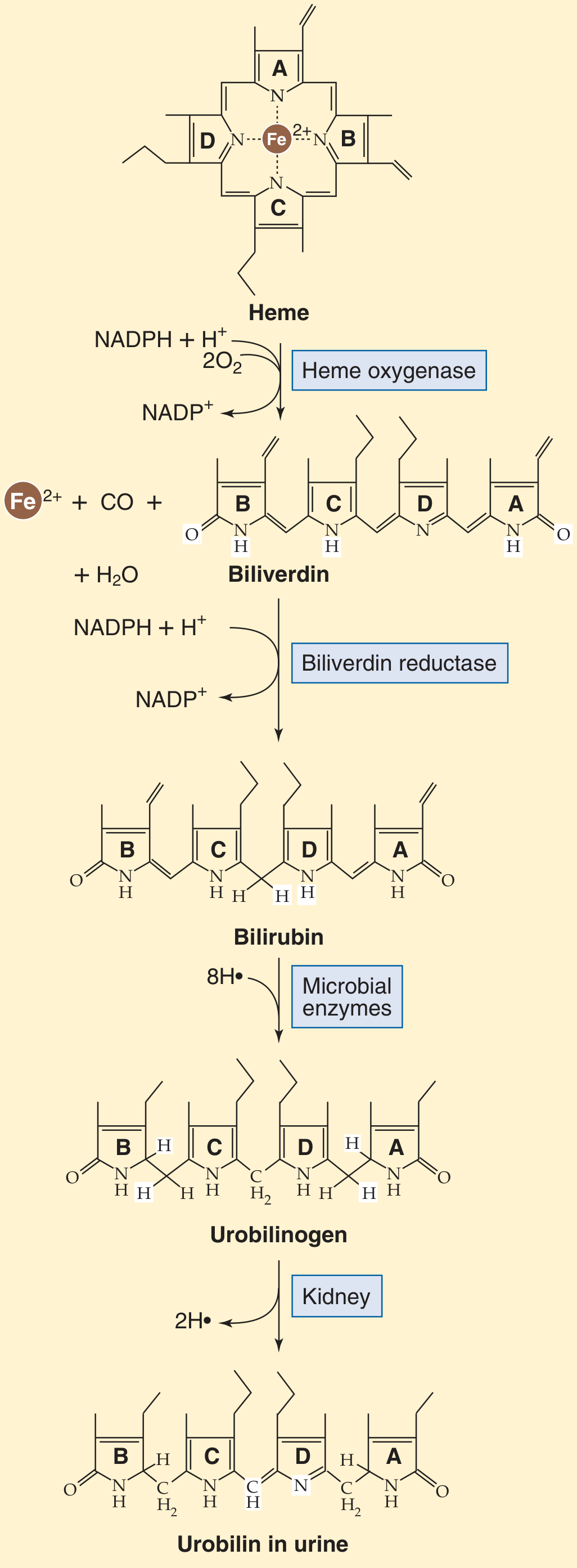
Figure 46-6A — Medical Physiology (Boron & Boulpaep)
Heme is degraded in the reticuloendothelial system (macrophages in spleen, liver, bone marrow):
-
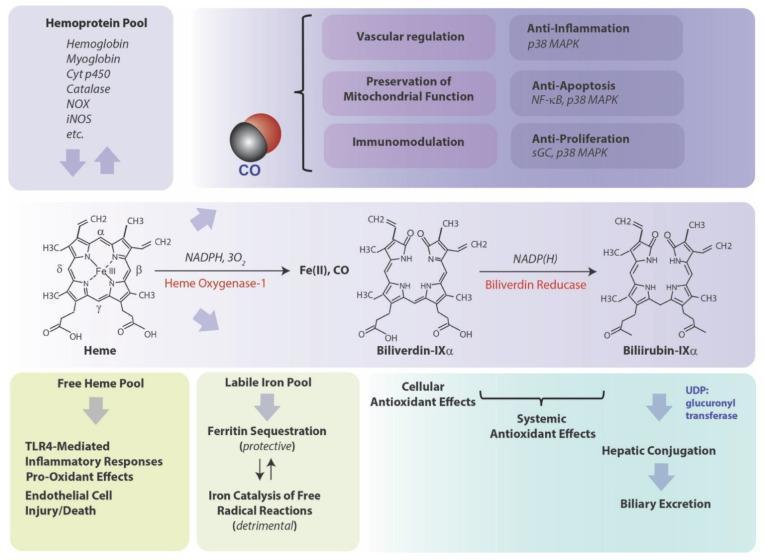
Heme oxygenase (HO-1 inducible, HO-2 constitutive) cleaves the α-methene bridge of the porphyrin ring using NADPH + 3O₂, releasing:
- Biliverdin-IXα (green tetrapyrrole)
- CO (carbon monoxide — signaling molecule with vasodilatory, anti-apoptotic, anti-inflammatory effects via p38 MAPK, NF-κB, sGC)
- Fe²⁺ (ferrous iron — recycled via transferrin; sequestered by ferritin to prevent Fenton reaction ROS)
-
Biliverdin reductase reduces biliverdin → bilirubin-IXα (yellow pigment) using NADPH.
Sources of bilirubin:
- 65–80% from hemoglobin of senescent red cells (RBC lifespan ~120 days)
- ~15% from myoglobin, cytochromes, and other hemoproteins
- ~10–15% from "ineffective erythropoiesis" (premature destruction of RBC precursors)
— Medical Physiology (Boron & Boulpaep), p. 1410
3. Bilirubin Transport and Hepatic Uptake
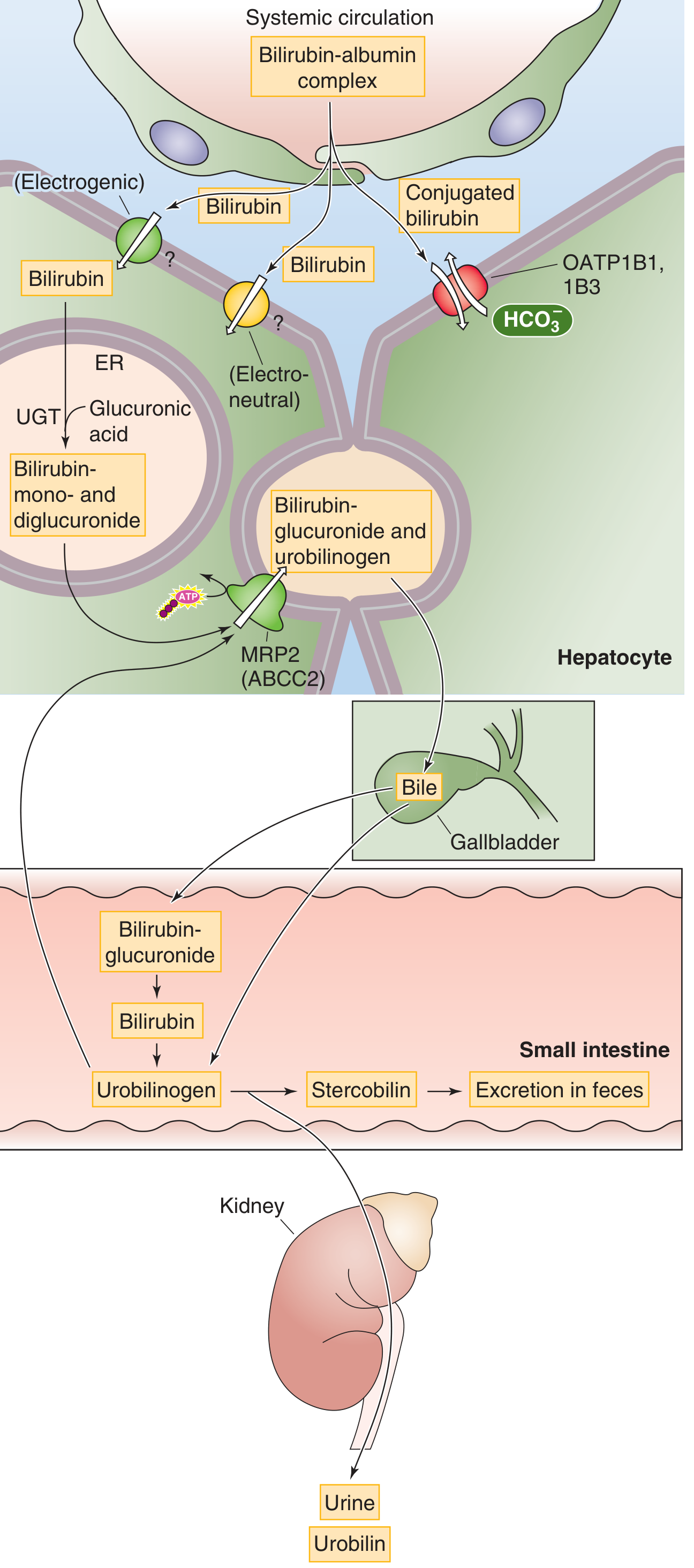
Figure 46-6B — Medical Physiology (Boron & Boulpaep)
Unconjugated (indirect) bilirubin is:
- Lipophilic and water-insoluble → cannot be excreted in urine or bile directly
- Bound reversibly to albumin in plasma (normally ~0.5 mg/dL total bilirubin, mostly unconjugated)
- Taken up by hepatocytes via OATP1B1 and OATP1B3 (organic anion transporting polypeptides) at the basolateral membrane
4. Hepatic Conjugation
Inside the hepatocyte endoplasmic reticulum, the enzyme UGT1A1 (UDP-glucuronosyltransferase 1A1) conjugates bilirubin with glucuronic acid:
- Bilirubin monoglucuronide (BMG)
- Bilirubin diglucuronide (BDG) — predominant form in bile
Conjugated bilirubin is water-soluble and can be excreted. It cannot be reabsorbed by biliary or intestinal epithelia once secreted.
Clinically important UGT1A1 defects:
| Disorder | UGT1A1 Activity | Bilirubin type | Features |
|---|---|---|---|
| Gilbert syndrome | Mildly reduced (~30%) | Unconjugated ↑ | Benign, common; exacerbated by fasting/stress |
| Crigler-Najjar type I | Absent | Unconjugated ↑↑↑ | Kernicterus, fatal without liver transplant |
| Crigler-Najjar type II | Severely reduced | Unconjugated ↑↑ | Less severe; responds to phenobarbital |
— Medical Physiology, p. 1410
5. Biliary Secretion and Intestinal Fate
Conjugated bilirubin is exported from the hepatocyte into the bile canaliculus via MRP2 (ABCC2) — an ATP-dependent efflux pump. It then flows through bile ducts → gallbladder → small intestine.
In the terminal ileum and colon:
- Intestinal bacteria (β-glucuronidases) deconjugate bilirubin glucuronides → free bilirubin
- Microbial enzymes reduce bilirubin → urobilinogen (colorless)
- Urobilinogen → stercobilin (brown pigment of feces) in the colon
- ~20% of urobilinogen is reabsorbed (enterohepatic circulation) → re-excreted in bile; small fraction reaches kidney → oxidized to urobilin (yellow pigment of urine)
6. Clinical Correlations: Jaundice
Jaundice (icterus) appears when serum bilirubin rises to 1.5–3 mg/dL. Normal total bilirubin is ≤1 mg/dL.
Classification of Hyperbilirubinemia
| Type | Mechanism | Bilirubin | Urine Bilirubin | Urine Urobilinogen | Stool Color |
|---|---|---|---|---|---|
| Pre-hepatic (hemolytic) | ↑ RBC destruction | Unconjugated ↑ | Absent (albumin-bound) | ↑↑ | Normal/dark |
| Hepatocellular | Liver disease (hepatitis, cirrhosis) | Mixed ↑ | Present | Variable | Pale |
| Post-hepatic (obstructive) | Bile duct obstruction | Conjugated ↑ | Present (dark urine) | Absent | Pale/clay-colored |
Diagnostic Approach
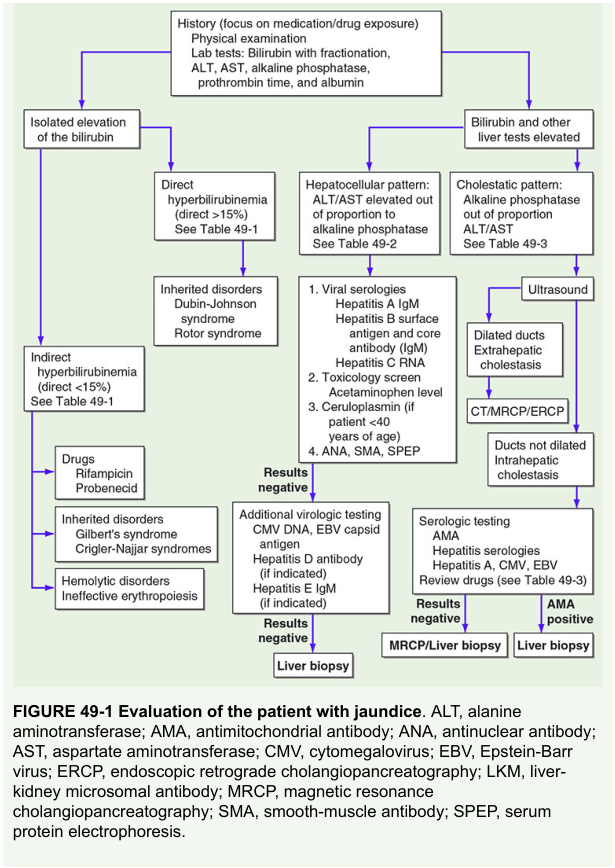
Figure 49-1 — Harrison's Principles of Internal Medicine, Evaluation of jaundice
Key inherited direct hyperbilirubinemia syndromes:
- Dubin-Johnson syndrome — defective MRP2; conjugated bilirubin cannot be exported into canaliculus; black liver pigment; benign
- Rotor syndrome — defective OATP1B1/1B3 re-uptake; conjugated bilirubin leaks into plasma
7. Laboratory Measurement of Bilirubin
The Jendrassik-Gróf method is the most common clinical assay:
- Diazotized sulfanilic acid reacts with bilirubin's pyrrole rings to form colored phenyl-azo adducts (absorbance at 600 nm)
- Direct bilirubin = conjugated bilirubin that reacts without a dissociating agent
- Total bilirubin = reacts after adding caffeine-benzoate (displaces albumin-bound unconjugated bilirubin)
- Indirect bilirubin = total − direct (≈ unconjugated bilirubin)
— Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 527
8. Neonatal Jaundice
Physiological neonatal jaundice results from:
- ↑ RBC turnover (fetal hemoglobin replacement)
- Immature UGT1A1 conjugation capacity
- Enhanced enterohepatic circulation (higher intestinal β-glucuronidase activity)
Treatment with phototherapy converts bilirubin to photoisomers and oxidation products that are less lipophilic and can be excreted without hepatic conjugation (photoisomers → bile; oxidation products → urine).
Extreme unconjugated hyperbilirubinemia → kernicterus (bilirubin deposition in basal ganglia and brainstem nuclei, causing brain damage).
Summary Pathway
Hemoglobin (senescent RBCs, ~80%)
↓ [Macrophages - RES]
Heme
↓ Heme Oxygenase (NADPH, O₂) → CO + Fe²⁺
Biliverdin
↓ Biliverdin Reductase (NADPH)
Unconjugated Bilirubin (lipophilic)
↓ [Bound to albumin in plasma]
Liver (OATP1B1/1B3 uptake)
↓ UGT1A1 (ER)
Conjugated Bilirubin (water-soluble)
↓ MRP2/ABCC2
Bile → Intestine
↓ Bacterial β-glucuronidase + reduction
Urobilinogen
↙ ↘
Stercobilin Reabsorbed → Re-excreted in bile
(feces, brown) Small fraction → Kidney → Urobilin (urine, yellow)
Sources: Medical Physiology (Boron & Boulpaep), p. 1409–1411 | Harrison's 22E, pp. 3386–3387 | Henry's Clinical Diagnosis and Management by Laboratory Methods | Tietz Textbook of Laboratory Medicine 7e
This is a shared conversation. Sign in to Orris to start your own chat.